
Abstract
The innate immune receptor toll-like receptor 4 (TLR4) has been implicated in mediating some of the effects of dietary lipids on inflammation and type 2 diabetes (T2D). Similar to TLR4, the nucleotide-binding oligomerization domains (Nods) 1 and 2 are also proteins of innate immunity, which can respond to lipids and initiate pro-inflammatory signalling that plays a role in the aetiology of T2D. The objective was to determine the effect of Nod1 (Glu266Lys) and Nod2 (Ser268Pro) genotypes on factors associated with the metabolic syndrome (MetS), and whether they modify the association between dietary lipids and biomarkers of the MetS. Men and women (n = 998) between the ages of 20–29 years were genotyped for both polymorphisms, completed a one-month, semiquantitative food frequency questionnaire and provided a fasting blood sample. The Glu266Lys polymorphism in Nod1 was not associated with any of the biomarkers of the MetS, but modified the association between dietary saturated fat (SFA) and insulin sensitivity, as measured by HOMA-IR (p for interaction = 0.04). Individuals with the Glu/Glu or Glu/Lys genotype showed no significant relationship between dietary SFA and HOMA-IR (β = −0.002 ± 0.006, p = 0.77; and β = −0.003 ± 0.006, p = 0.61), while those with the Lys/Lys genotype showed a positive association (β = 0.033 ± 0.02, p = 0.03). The Nod2 Ser268Pro polymorphism was not associated with components of the MetS and did not modify the relationship between dietary lipid intake and the biomarkers of MetS. In summary, the Nod1 Glu266Lys polymorphism modifies the relationship between dietary SFA intake and HOMA-IR, suggesting that Nod1 may act as an intracellular lipid sensor affecting insulin sensitivity.
Similar content being viewed by others


Introduction
Although the mechanisms by which the metabolic syndrome (MetS) and type 2 diabetes (T2D) develop are still unknown, there is growing evidence that chronic, low-grade inflammation may play a role in promoting the development of these conditions (Pradhan 2007; Wellen and Hotamisligil 2005). Environmental factors such as dietary fat as well as individual genetic variation can both influence an individual’s inflammatory status and contribute to the pathogenesis of T2D (Peeters et al. 2008; Mann 2006). However, the role of various diet–gene interactions remains unknown.
The innate immune receptor toll-like receptor 4 (TLR4) has been shown to play a role in high-fat-diet-induced insulin resistance as mice lacking a functional TLR4 show blunted inflammation and do not develop insulin resistance despite the consumption of a high-fat diet (Tsukumo et al. 2007; Shi et al. 2006). However, the absence of TLR4 has been found to be insufficient to completely block the effects of fatty acids on insulin action, in vitro. This suggests that TLR4 is not the sole pathway by which fatty acids affect insulin sensitivity (Radin et al. 2008). In addition to toll-like receptors, the nucleotide-binding oligomerization domains (Nods) 1 and 2 are cytosolic proteins of innate immunity (Girardin et al. 2003). The Nod proteins play a role in innate immunity by detecting peptidoglycan structures. Nod1 detects structures unique to gram-negative bacteria, while Nod2 detects structures found in both gram-negative and gram-positive bacteria (Girardin et al. 2003a, b). Similar to TLR4, Nods recognize these structures through the leucine-rich repeat domain at the carboxy terminus (Chamaillard et al. 2003; Inohara and Nunez 2003) and activate common NF-κB pathways (Inohara et al. 2000; Abbott et al. 2004). Both Nod1 and Nod2 have been shown to be modulated by fatty acids. Using colonic epithelial cells free of TLR4, (Zhao et al. 2007), showed that SFAs dose dependently activated NF-κB and increased IL-8 expression through the Nod proteins. Conversely, PUFAs inhibited these effects also through the Nod proteins (Zhao et al. 2007).
Polymorphisms in the Nod proteins have been implicated in a number of inflammatory diseases. Single nucleotide polymorphisms (SNPs) in Nod1 have been associated with increased risk for atopic eczema, asthma, elevated levels of immunoglobulin E (Zhao et al. 2007; Weidinger et al. 2005) and inflammatory bowel disease in some populations (Hysi et al. 2005). SNPs in Nod2 have been associated with Crohn’s disease and ulcerative colitis (McGovern et al. 2005; Entrez 2011), Blau disease (Hugot et al. 2001) and early onset sarcoidosis (Ogura et al. 2001). Despite the emerging role of innate immunity-related inflammation in the MetS and T2D (Miceli-Richard et al. 2001), the relationship between polymorphisms in Nod proteins and risk of these conditions has not yet been examined.
The objective of the present study was to determine whether polymorphisms in Nod1 and Nod2 genes are associated with markers of T2D or influence the association between dietary fat intake and insulin sensitivity in a population of young adults. The polymorphisms selected in Nod1 (rs2075820—G1319A in exon 6 resulting in Glu266Lys) and Nod2 (rs2066842—T907C in exon 4 resulting in Pro268Ser) are non-synonymous SNPs that could affect protein function, and the minor alleles have been shown to occur at high frequencies in certain populations (Kanazawa et al. 2005).
Methods
Study population
The Toronto Nutrigenomics and Health (TNH) study explores the role of genetics and nutrition in health and chronic disease (Radin et al. 2008; Badawi et al. 2010; Fontaine-Bisson et al. 2007; Cahill et al. 2009; Eny et al. 2008). Subjects (n = 998) were recruited from the University of Toronto, Canada, and are between 20 and 29 years of age. Anthropometric measurements were taken, and a general health and lifestyle questionnaire, physical activity questionnaire and food frequency questionnaire were completed by each subject. Pregnant or breastfeeding women were excluded from the study. Individuals who may have underreported (≤800 kcal/day) or over-reported (≥3,500 kcal/day female, ≥4,000 kcal/day male) their dietary intake on their food frequency questionnaire were excluded from the analysis (n = 96) as were subjects with diabetes, Crohn’s disease, ulcerative colitis or arthritis (n = 14). Individuals with inflammation due to other factors (n = 64) were excluded from the analysis and was defined as those with CRP ≥ 10 mg/L or those who reported infection, fever, dental surgery, or being tattooed or pierced within the week before their blood draw. Individuals who were missing data relevant to the MetS were also excluded (n = 20). Written informed consent was obtained from all participants, and the study was approved by the Ethics Review Committee at the University of Toronto.
Dietary assessment
A 196-item Toronto-modified Willett food frequency questionnaire (FFQ) was used to assess habitual dietary intake over the last month. Each subject was instructed on how to complete the FFQ using visual aids of portion sizes to improve the accuracy of self-reported food intake. Subject responses to each food item were converted to daily number of servings for each. Total, saturated, monounsaturated and polyunsaturated fat intake was assigned to a serving of each food item based on the nutrient contents listed for the food in the US Department of Agriculture database.
Anthropometrics and energy expenditure
Anthropometric measurements included height and weight, from which BMI (kg/m2) was calculated, and waist circumference. Modifiable activity was measured by questionnaire as previously described (Ainsworth et al. 1993; Paffenbarger et al. 1993), and a metabolic equivalent hours per day (MET h/day) was calculated. This variable represents both leisure and occupational activity, not including hours spent sleeping or sitting. One MET h is equal to 1 kcal expended per kg body weight per hour sitting at rest (Fontaine-Bisson et al. 2009).
Laboratory measurements
A venous blood sample was taken from each subject after a 12 h overnight fast and used to measure biomarkers of glucose and lipid metabolism (glucose, insulin, total- and HDL-cholesterol, triglycerides, free fatty acids), and inflammation (hs-CRP) using standard clinical procedures. LDL-cholesterol was calculated using the Friedewald equation, while HOMA-IR and HOMA-β were calculated using the following equations:
Genotyping
DNA was isolated from whole blood using the GenomicPrep Blood DNA Isolation kit (Amersham Pharmacia Biotech, Piscataway, NJ). The Nod1 and Nod2 polymorphisms were detected using TaqMan® allelic discrimination assays (ABI no. C-2641989-10 for the Nod1 Glu266Lys and ABI no. C-11717470-20 for the Nod2 Pro268Ser) from Applied Biosystems (Foster City, CA), with real-time PCR on an ABI 7000 Sequence Detection System. PCR conditions were 95°C for 10 min and 40 cycles of 95°C for 15 s and 60°C for 1 min.
Statistical analysis
All statistical analyses were performed using SAS version 9.1 (SAS Institute Inc., Cary, NC). The SAS procedure GLM was used to perform a one-way analysis of variance to test for differences in the characteristics between genotypes (Glu/Glu, Glu/Lys and Lys/Lys; Pro/Pro and Ser carriers for the Nod1 and Nod2 SNPs, respectively) and the CONTRAST statement used for pairwise group comparisons. The χ2 test was used to analyse categorical variables (ethnicity, gender, smoking status, family history of diabetes). Non-normally distributed variables (BMI, waist circumference, free fatty acids, insulin, HOMA-IR, HOMA-β, triglycerides (TG), monounsaturated fat intake (MUFA) and polyunsaturated fat intake (PUFA)) were loge-transformed for analysis, and their antilogs are reported. Hs-CRP was transformed following a gamma distribution using the GENMOD procedure, and the median and interquartile range values for this variable are given. Any anthropometric, dietary and lifestyle variables that were significantly different across genotypes were adjusted for in analysis of metabolic characteristics, and all subject characteristics are presented in Table 2.
The GLM procedure was also used to test whether the effect of dietary total, SFA, MUFA or PUFA as a continuous or categorical variable on different components of the metabolic syndrome or diabetes varied across the various genotypes for each polymorphism. A diet–gene interaction was found for dietary SFA and the Nod1 Glu266Lys (rs2075820) polymorphism on HOMA-IR. The model included HOMA-IR as the response variable and genotype, SFA and their interaction as the predictor variables. Covariates that were significantly associated with the outcome and reduced the variance of the relationship were included in the model (fibre intake, HDL:total cholesterol ratio, CRP and waist circumference). Potential covariates that were associated with the outcome or differed between genotypes were added individually to the model to test whether the interaction changed and were not included in the final model. Dietary SFA was adjusted for total energy intake by using the nutrient density method (% of energy from dietary fatty acids) (Ainsworth et al. 1993). Slopes of the three lines were estimated using the GLM procedure on a fully adjusted model including the genotype and genotype × SFA interaction terms. No interactions were found between Nod1 genotype and any of these potential confounders. Departure of genotype distributions from Hardy–Weinberg equilibrium was assessed using a χ2 test with 1 df and confirmed using the HAPLOVIEW software. Significant p values are two-sided and less than 0.05. Tukey’s post hoc test was used to correct for multiple comparisons when appropriate.
Results
The allele frequencies for the Nod1 Gly266Lys SNP were 48% for the Glu/Glu, 43% for the Glu/Lys and 9% for the Lys/Lys. The minor allele (Lys) was present in 30% of the total population. Distribution of the polymorphism was significantly different between ethnicities (p = 0.003, χ2 test) as the polymorphism was less frequent in Caucasians when compared to the other groups (Table 1). Genotype frequency in the total population did not deviate from Hardy–Weinberg equilibrium (p = 0.87).
The Glu266Lys polymorphism was associated with differences in total cholesterol levels, which was primarily due to LDL-cholesterol (Table 2). Carriers of the Lys allele had significantly lower total- and LDL-cholesterol levels compared to the Glu/Glu homozygotes (p = 0.004 and p = 0.003, respectively), although the difference was small and not likely to be biologically significant in this population. None of the other metabolic characteristics differed between genotypes.
The polymorphism in Nod1 modified the association between dietary SFA intake and HOMA-IR, a calculated measurement of insulin sensitivity. A significant diet–gene interaction was found between SFA intake and the Glu266Lys polymorphism on HOMA-IR (p = 0.04, adjusted for dietary fibre, total:HDL cholesterol, waist circumference and hs-CRP). Adjustment for alcohol intake and ethnicity, which differed significantly across the genotypes, did not change the interaction (p = 0.04). Further adjustment for variables that were associated with the outcome did not alter the results. A positive association between SFA intake (% energy) and HOMA-IR was only seen in individuals who were homozygous for the Lys allele (Table 3), while no significant relationship was present in the other genotypes. The slope of the relationship between SFA and HOMA-IR in Lys/Lys individuals was 0.033 ± 0.02 (p = 0.03) and was significantly different from the slope of the other two genotypes (p = 0.03 for Glu/Glu and p = 0.02 for Glu/Lys). The slopes of this relationship in the other two genotypes (Glu/Glu and Glu/Lys) were not significantly different from each other (p = 0.81). This effect did not differ between the different ethnocultural groups (p = 0.22 for the three way interaction between genotype × SFA × ethnocultural group). No diet–gene interaction was found for any of the other factors associated with the MetS (waist circumference, TG, HDL, glucose, systolic and diastolic blood pressure) or inflammation (hs-CRP).
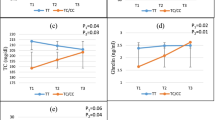
SFA intake was also divided into a binary variable according to recommended intake levels (≤10% energy intake) in order to account for assumptions of linearity (Fig. 1). The interaction approached significance when this method was used (p = 0.08, adjusted for dietary fibre, total:HDL cholesterol, waist circumference and hs-CRP). Contrasting the highest and lowest intakes of SFA by genotype, mean HOMA-IR was significantly higher in individuals consuming above recommended levels of SFA in the Lys/Lys genotype (p = 0.02). There were no differences in HOMA-IR according to SFA intake in the other two genotypes (p = 0.55 for Glu/Glu and p = 0.55 for Glu/Lys).

Nod1 Glu266Lys polymorphism (rs2075820) modifies the association between dietary SFA intake and HOMA-IR in a population of young adults (p for interaction = 0.08) Values are means ± SEM adjusted for fibre intake (% carbohydrates), total:HDL cholesterol ratio, waist circumference and hs-CRP
The frequency of the Nod2 Ser268Pro genotypes in this population were 75% for Ser/Ser, 22% Ser/Pro and 3% Pro/Pro. Because of the low frequency of the Pro/Pro genotype, these individuals were combined with the Ser/Pro genotype to create a Pro carrier group. When analysed by ethnocultural group, the frequency of the Pro allele in East Asians was 2%, so this group was excluded from the population to avoid ethnocultural confounding. The frequency of this polymorphism was in Hardy–Weinberg equilibrium when East Asians were excluded (p = 0.29).
The Ser268Pro polymorphism in Nod2 was not associated with differences in any factors related to the MetS. It also did not modify the relationship between total fat, MUFA, PUFA or SFA intake and these factors (waist circumference, TG, HDL, glucose, systolic and diastolic blood pressure, hs-CRP and HOMA-IR).
Discussion
The objective of this study was to investigate whether polymorphisms in Nod1 (Glu266Lys) or Nod2 (Ser268Pro) were associated with differences in biomarkers of the MetS and whether these polymorphisms modified the association between dietary fat and insulin sensitivity. The Glu266Lys SNP in Nod1 was found to modify the association between dietary SFA and insulin sensitivity, as determined by HOMA-IR. There was a positive association between dietary SFA and HOMA-IR in individuals who were Lys/Lys homozygous for the polymorphism, while no relationship was observed for the other genotypes.
Individuals homozygous for the polymorphism and consuming a high-SFA diet (≥10% energy) had a mean HOMA-IR of 1.64 that was significantly higher than homozygous individuals consuming a low-SFA diet (<10% energy), who had a mean HOMA-IR of 1.25. A HOMA-IR value of 2.60 is a commonly used cut-off for insulin resistance (Ascaso et al. 2003); however, a prospective study in a multi-ethnocultural cohort of women found that individuals who had a HOMA-IR > 1.439 had a 3.97 times increased risk of developing T2D (5.9 years follow-up) compared to those with a HOMA-IR ≤ 1.439 (Song et al. 2007). Thus, in the present study, homozygous individuals (Lys/Lys) consuming a high-SFA diet may be at higher risk of developing T2D than Lys/Lys individuals consuming a low-SFA diet.
The effect of the Glu266Lys polymorphism on Nod1 function is not known; however; it appears as though it may affect the individual’s response to lipid intake. Nod1 has been found to respond to lipids (Lee et al. 2003), eliciting a pro-inflammatory response to SFAs. Higher intakes of SFA could be promoting Nod1 signalling, either directly or indirectly, which would lead to an NF-κB-mediated inflammatory response. Another innate immune protein, TLR4, has been implicated in the development of T2D as a result of a high-fat diet (Shi et al. 2006). Both Nod1 and TLR4 share similar structures and signalling pathways. Cross-talk between TLRs and Nod proteins has also been observed, as expression of Nod1 and Nod2 mRNA is induced by TLR activation (Willet 1998; Rosenstiel et al. 2003). While TLR4 provides a possible role of innate immunity in linking dietary fat to insulin resistance, it does not consider intracellular fatty acids, which are associated with insulin resistance (Takahashi et al. 2006).
Epidemiological evidence suggests that the consumption of a Western diet, high in SFAs, correlates with the development of insulin resistance (Pan et al. 1997; Parker et al. 1993), and in vitro studies using muscle cells have shown that SFAs can cause insulin resistance (Maron et al. 1991; Chavez and Summers 2003). Animal studies have also shown that a high-SFA diet can promote the accumulation of intramuscular lipids, which have been highly associated with insulin resistance (Montell et al. 2001). In humans, insulin resistance directly correlates with increased SFAs in skeletal muscle triglycerides (Lee et al. 2006; Manco et al. 2000). However, data from clinical trials have not supported this role of a high-SFA diet in insulin resistance (Tierney et al. 2011). Mechanisms by increased SFAs in triglycerides may increase insulin resistance include the inhibitory effects of these lipid metabolites on the insulin receptor. Skeletal muscle exposed to SFAs can also produce TNF-α and IL-6 (Jove et al. 2005; Jove et al. 2006), but no mechanism has been found to explain this.
It is well known that Nod1 can be found in glucose-metabolizing tissues, including muscle cells (Inohara et al. 1999), liver and adipose (Dharancy et al. 2009). Thus, there is a potential that Nod1 in these cells may act as a sensor for intracellular fats and lead to impaired insulin sensitivity. In order to affect Nod1, SFAs must be transported into the cell or be incorporated into cell membrane phospholipids. It is difficult to estimate the effects of dietary fat on lipid constituents of the plasma membrane as many saturated and monounsaturated fatty acids in the diet can also be synthesized endogenously. However, although weakly correlated, dietary fat is a determinant of cell membrane structure (Clandinin et al. 1991). Nod1 associated with the plasma membrane might be able to sense these lipids upon their release by phospholipases. Fatty acids entering the cell through mechanisms such as lipid transporters or from the cell membrane would also be exposed to cytosolic Nod1. However, whether the pro-inflammatory response from Nod1 affects insulin sensitivity remains to be determined, although findings from the present study suggest that it may.
The Ser268Pro polymorphism in Nod2 was not associated with any of the metabolic characteristics of the study subjects and did not alter the relationship between dietary lipids and factors of the MetS. Unlike Nod1, which is fairly ubiquitous, Nod2 is expressed in a limited number of specific cell types, such as macrophages (Ogura et al. 2001), dendritic cells (Tada et al. 2005) and colonic epithelial cells (Hisamatsu et al. 2003). Our findings indicate that either the particular polymorphism examined does not affect the response of Nod2 to lipids, or that this protein does not play a significant role in mediating inflammation in response to diet in healthy individuals. In obesity, there is infiltration of the adipose tissue by macrophages, which can mediate an inflammatory response. It is possible, however, that Nod2 could play a more significant role in individuals with higher BMI. However, there were not enough obese individuals in the present population (n = 27) to evaluate this assumption.
In the present study, we report the first observation implicating Nod1 in promoting the intracellular pro-inflammatory response to lipids. The Nod1 Glu266Lys polymorphism modifies the association between dietary SFA and insulin sensitivity in a young, healthy population. These results support a possible role of Nod1-mediated innate immunity in modulating the effects of diet on the MetS.
Abbreviations
- BMI:
-
Body mass index
- CRP:
-
C-reactive protein
- FFQ:
-
Food frequency questionnaire
- HOMA-IR:
-
Homeostasis model assessment of insulin resistance
- HOMA-β:
-
Homeostasis model assessment of beta cell function
- hs-CRP:
-
High-sensitivity CRP
- MET:
-
Metabolic equivalent
- MetS:
-
Metabolic syndrome
- MUFA:
-
Monounsaturated fatty acids
- PUFA:
-
Polyunsaturated fatty acids
- SFA:
-
Saturated fatty acids
- T2D:
-
Type II diabetes mellitus
- TNH:
-
Toronto nutrigenomics and health study
References
Abbott DW, Wilkins A, Asara JM, Cantley LC (2004) The Crohn’s disease protein, NOD2, requires RIP2 in order to induce ubiquitinylation of a novel site on NEMO. Curr Biol 200414:2217–2227
Ainsworth BE, Haskell WL, Leon AS, Jacobs DR Jr, Montoye HJ, Sallis JF, Paffenbarger RS Jr (1993) Compendium of physical activities: classification of energy costs of human physical activities. Med Sci Sports Exerc 25:71–80
Ascaso JF, Pardo S, Real JT, Lorent RI, Priego A, Carmena R (2003) Diagnosing insulin resistance by simple quantitative methods in subjects with normal glucose metabolism. Diab Care 26:3320–3325
Badawi A, Klip A, Haddad P, Cole DE, Garcia-Bailo B, El-Sohemy A, Karmali M (2010) Type 2 diabetes mellitus and inflammation: prospects for biomarkers of risk and nutritional intervention. Diabetes Metab Syndr Obes 3:173–186
Cahill LE, Fontaine-Bisson B, El-Sohemy A (2009) Functional genetic variants of glutathione S-transferase protect against serum ascorbic acid deficiency. Am J Clin Nutr 90:1411–1417
Chamaillard M, Girardin SE, Viala J, Philpott DJ (2003) Nods, Nalps and Naip: intracellular regulators of bacterial-induced inflammation. Cell Microbiol 5:581–592
Chavez JA, Summers SA (2003) Characterizing the effects of saturated fatty acids on insulin signaling and ceramide and diacylglycerol accumulation in 3T3-L1 adipocytes and C2C12 myotubes. Arch Biochem Biophys 419:101–109
Clandinin MT, Cheema S, Field CJ, Garg ML, Venkatraman J, Clandinin TR (1991) Dietary fat: exogenous determination of membrane structure and cell function. FASEB J 5:2761–2769
Dharancy S, Body-Malapel M, Louvet A, Berrebi D, Gantier E, Gosset P, Viala J, Hollebecque A, Moreno C, Philpott DJ, Girardin SE, Sansonetti PJ, Desreumaux P, Mathurin P, Dubuquoy L (2009) Neutrophil migration during liver injury is under nucleotide-binding oligomerization domain 1 control. Gastroenterology 138:1546–1556
Entrez SNP (2011) Accessed on: 24 Oct, 2011. Available at: http://www.ncbi.nlm.nih.gov/snp
Eny KM, Wolever TM, Fontaine-Bisson B, El-Sohemy A (2008) Genetic variant in the glucose transporter type 2 is associated with higher intakes of sugars in two distinct populations. Physiol Genomics 33:355–360
Fontaine-Bisson B, Wolever TM, Chiasson JL, Rabasa-Lhoret R, Maheux P, Josse RG, Leiter LA, Rodger NW, Ryan EA, Connelly PW, Corey PN, El-Sohemy A (2007) Genetic polymorphisms of tumor necrosis factor-alpha modify the association between dietary polyunsaturated fatty acids and fasting HDL-cholesterol and apo A-I concentrations. Am J Clin Nutr 86:768–774
Fontaine-Bisson B, Wolever TM, Connelly PW, Corey PN, El-Sohemy A (2009) NF-kappaB -94Ins/Del ATTG polymorphism modifies the association between dietary polyunsaturated fatty acids and HDL-cholesterol in two distinct populations. Atherosclerosis 204:465–470
Girardin SE, Boneca IG, Carneiro LA, Antignac A, Jehanno M, Viala J, Tedin K, Taha MK, Labigne A, Zahringer U, Coyle AJ, DiStefano PS, Bertin J, Sansonetti PJ, Philpott DJ (2003a) Nod1 detects a unique muropeptide from gram-negative bacterial peptidoglycan. Science 300:1584–1587
Girardin SE, Boneca IG, Viala J, Chamaillard M, Labigne A, Thomas G, Philpott DJ, Sansonetti PJ (2003b) Nod2 is a general sensor of peptidoglycan through muramyl dipeptide (MDP) detection. J Biol Chem 278:8869–8872
Hisamatsu T, Suzuki M, Reinecker HC, Nadeau WJ, McCormick BA, Podolsky DK (2003) CARD15/NOD2 functions as an antibacterial factor in human intestinal epithelial cells. Gastroenterology 124:993–1000
Hugot JP, Chamaillard M, Zouali H, Lesage S, Cezard JP, Belaiche J, Almer S, Tysk C, O’Morain CA, Gassull M, Binder V, Finkel Y, Cortot A, Modigliani R, Laurent-Puig P, Gower-Rousseau C, Macry J, Colombel JF, Sahbatou M, Thomas G (2001) Association of NOD2 leucine-rich repeat variants with susceptibility to Crohn’s disease. Nature 411:599–603
Hysi P, Kabesch M, Moffatt MF, Schedel M, Carr D, Zhang Y, Boardman B, von Mutius E, Weiland SK, Leupold W, Fritzsch C, Klopp N, Musk AW, James A, Nunez G, Inohara N, Cookson WO (2005) NOD1 variation, immunoglobulin E and asthma. Hum Mol Genet 14:935–941
Inohara N, Nunez G (2003) NODs: intracellular proteins involved in inflammation and apoptosis. Nat Rev Immunol 3:371–382
Inohara N, Koseki T, del Peso L, Hu Y, Yee C, Chen S, Carrio R, Merino J, Liu D, Ni J, Nunez G (1999) Nod1, an Apaf-1-like activator of caspase-9 and nuclear factor-kappaB. J Biol Chem 274:14560–14567
Inohara N, Koseki T, Lin J, del Peso L, Lucas PC, Chen FF, Ogura Y, Nunez G (2000) An induced proximity model for NF-kappa B activation in the Nod1/RICK and RIP signaling pathways. J Biol Chem 275:27823–27831
Jove M, Planavila A, Laguna JC, Vazquez-Carrera M (2005) Palmitate-induced interleukin 6 production is mediated by protein kinase C and nuclear-factor kappaB activation and leads to glucose transporter 4 down-regulation in skeletal muscle cells. Endocrinology 146:3087–3095
Jove M, Planavila A, Sanchez RM, Merlos M, Laguna JC, Vazquez-Carrera M (2006) Palmitate induces tumor necrosis factor-alpha expression in C2C12 skeletal muscle cells by a mechanism involving protein kinase C and nuclear factor-kappaB activation. Endocrinology 147:552–561
Kanazawa N, Okafuji I, Kambe N, Nishikomori R, Nakata-Hizume M, Nagai S, Fuji A, Yuasa T, Manki A, Sakurai Y, Nakajima M, Kobayashi H, Fujiwara I, Tsutsumi H, Utani A, Nishigori C, Heike T, Nakahata T, Miyachi Y (2005) Early-onset sarcoidosis and CARD15 mutations with constitutive nuclear factor-kappaB activation: common genetic etiology with Blau syndrome. Blood 105:1195–1197
Lee JY, Ye J, Gao Z, Youn HS, Lee WH, Zhao L, Sizemore N, Hwang DH (2003) Reciprocal modulation of Toll-like receptor-4 signaling pathways involving MyD88 and phosphatidylinositol 3-kinase/AKT by saturated and polyunsaturated fatty acids. J Biol Chem 278:37041–37051
Lee JS, Pinnamaneni SK, Eo SJ, Cho IH, Pyo JH, Kim CK, Sinclair AJ, Febbraio MA, Watt MJ (2006) Saturated, but not n-6 polyunsaturated, fatty acids induce insulin resistance: role of intramuscular accumulation of lipid metabolites. J Appl Physiol 100:1467–1474
Manco M, Mingrone G, Greco AV, Capristo E, Gniuli D, De Gaetano A, Gasbarrini G (2000) Insulin resistance directly correlates with increased saturated fatty acids in skeletal muscle triglycerides. Metabolism 49:220–224
Mann JI (2006) Evidence-based nutrition recommendations for the treatment and prevention of type 2 diabetes and the metabolic syndrome. Food Nutr Bull 27:161–166
Maron DJ, Fair JM, Haskell WL (1991) Saturated fat intake and insulin resistance in men with coronary artery disease. The Stanford Coronary Risk Intervention Project Investigators and Staff. Circulation 84:2020–2027
McGovern DPB, Hysi P, Ahmad T, van Heel DA, Moffat MF, Carey A, Cookson WOC, Jewell DP (2005) Association between a complex insertion/deletion polymorphism in NOD1 (CARD4) and susceptibility to inflammatory bowel disease. Hum Mol Genet 14:1245–1250
Miceli-Richard C, Lesage S, Rybojad M, Prieur AM, Manouvrier-Hanu S, Hafner R, Chamaillard M, Zouali H, Thomas G, Hugot JP (2001) CARD15 mutations in Blau syndrome. Nat Genet 29:19–20
Montell E, Turini M, Marotta M, Roberts M, Noe V, Ciudad CJ, Mace K, Gomez-Foix AM (2001) DAG accumulation from saturated fatty acids desensitizes insulin stimulation of glucose uptake in muscle cells. Am J Physiol Endocrinol Metab 280:E229–E237
Ogura Y, Inohara N, Benito A, Chen FF, Yamaoka S, Nunez G (2001a) A frameshift mutation in NOD2 associated with susceptibility to Crohn’s disease. Nature 411:603–606
Ogura Y, Inohara N, Benito A, Chen FF, Yamaoka S, Nunez G (2001b) Nod2, a Nod1/Apaf-1 family member that is restricted to monocytes and activates NF-kappaB. J Biol Chem 276:4812–4818
Paffenbarger RS Jr, Blair SN, Lee IM, Hyde RT (1993) Measurement of physical activity to assess health effects in free-living populations. Med Sci Sports Exerc 25:60–70
Pan DA, Lillioja S, Kriketos AD, Milner MR, Baur LA, Bogardus C, Jenkins AB, Storlien LH (1997) Skeletal muscle triglyceride levels are inversely related to insulin action. Diabetes 46:983–988
Parker DR, Weiss ST, Troisi R, Cassano PA, Vokonas PS, Landsberg L (1993) Relationship of dietary saturated fatty acids and body habitus to serum insulin concentrations: the Normative Aging Study. Am J Clin Nutr 58:129–136
Peeters MW, Thomis MA, Loos RJ, Derom CA, Fegard R, Vlietinck RF, Beunen GP (2008) Clustering of metabolic risk factors in young adults: genes and environment. Atherosclerosis 200:168–176
Pradhan A (2007) Obesity, metabolic syndrome, and type 2 diabetes: inflammatory basis of glucose metabolic disorders. Nutr Rev 65:S152–S156
Radin MS, Sinha S, Bhatt BA, Dedousis N, O’Doherty RM (2008) Inhibition or deletion of the lipopolysaccharide receptor Toll-like receptor-4 confers partial protection against lipid-induced insulin resistance in rodent skeletal muscle. Diabetologia 51:336–346
Rosenstiel P, Fantini M, Brautigam K et al (2003) TNF-alpha and IFN-gamma regulate the expression of the NOD2 (CARD15) gene in human intestinal epithelial cells. Gastroenterology 124:1001–1009
Shi H, Kokoeva MV, Inouye K, Tzameli I, Yin H, Flier JS (2006) TLR4 links innate immunity and fatty acid-induced insulin resistance. J Clin Invest 116:3015–3025
Song Y, Mason J, TInker L, Howard BV, Kuller LH, Nathan L, Rifai N, Liu N (2007) Insulin sensitivity and insulin secretion determined by homeostasis model assessment and risk of diabetes in a multiethnic cohort of women. Diab Care 30:1747–1752
Tada H, Aiba S, Shibata K, Ohteki T, Takada H (2005) Synergistic effect of Nod1 and Nod2 agonists with toll-like receptor agonists on human dendritic cells to generate interleukin-12 and T helper type 1 cells. Infect Immun 73:7967–7976
Takahashi Y, Isuzugawa K, Murase Y, Imai M, Yamamoto S, Iizuka M, Akira S, Bahr GM, Momotani E, Hori M, Ozaki H, Imakawa K (2006) Up-regulation of NOD1 and NOD2 through TLR4 and TNF-alpha in LPS-treated murine macrophages. J Vet Med Sci 68:471–478
Tierney AC, McMonagle J, Shaw DI, Gulseth HL, Helal O, Saris WH, Paniagua JA, Golabek-Leszczyñska I, Defoort C, Williams CM, Karsltröm B, Vessby B, Dembinska-Kiec A, López-Miranda J, Blaak EE, Drevon CA, Gibney MJ, Lovegove JA, Roche HM (2011) Effects of dietary fat modification on insulin sensitivity and on other risk factors of the metabolic syndrome–LIPGENE: a European randomized dietary intervention study. Int J Obes (Lond) 35(6):800–809
Tsukumo DM, Carvalho-Filho MA, Carvalheira JB, Prada PO, Hirabara SM, Schenka AA, Araujo EP, Vassallo J, Curi R, Velloso LA, Saad MJ (2007) Loss-of-function mutation in Toll-like receptor 4 prevents diet-induced obesity and insulin resistance. Diabetes 56:1986–1998
Weidinger S, Klopp N, Rummler L, Wagenpfeil S, Novak N, Baurecht HJ, Groer W, Darsow U, Heinrich J, Gauger A, Schafer T, Jakob T, Behrendt H, Wichmann HE, Ring J, Illig T (2005) Association of NOD1 polymorphisms with atopic eczema and related phenotypes. J Allergy Clin Immunol 116:177–184
Wellen KE, Hotamisligil GS (2005) Inflammation, stress, and diabetes. J Clin Invest 115:1111–1119
Willet W (1998) Nutritional epidemiology, 2nd edn. Oxford University Press, New York
Zhao L, Kwon MJ, Huang S, Lee JY, Fukase K, Inohara N, Hwang DH (2007) Differential modulation of Nods signaling pathways by fatty acids in human colonic epithelial HCT116 cells. J Biol Chem 282:11618–11628
Acknowledgments
AE-S holds a Canada Research Chair in Nutrigenomics. MK and AB received support from the Public Health Agency of Canada.
Conflict of interest
The authors do not have any conflicts of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cuda, C., Badawi, A., Karmali, M. et al. Effects of polymorphisms in nucleotide-binding oligomerization domains 1 and 2 on biomarkers of the metabolic syndrome and type II diabetes. Genes Nutr 7, 427–435 (2012). https://doi.org/10.1007/s12263-012-0287-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12263-012-0287-5