
Abstract
Objectives
This study aimed at examining the effect of the nutrition education program on adolescents’ knowledge, attitudes and behaviour in relation to nutrition in rural China.
Methods
A cluster-randomised intervention trial design was employed. Two middle schools were randomly selected and assigned to the school conducting nutrition education (NE school), or to the Control school, in Mi Yun County, Beijing. From each school 65 seventh-grade students were randomly selected to participate in the study. Nutrition-related knowledge, attitudes and behaviour were measured at pre- and post-intervention surveys with the same instrument. The nutrition education lasted for 6 months.
Results
After the intervention, more students in NE school knew the main function of dairy products and vegetables, which micronutrient is rich in dairy products and beans, and in meat, and the symptom of food poisoning, than those in Control school. The rate of students who thought nutrition is very important to health, and foods with an expired date should be thrown away in NE school was higher than that in Control school (93.8 vs. 80.3 and 92.3 vs. 78.7 %, respectively). The rate of students who ate vegetables and breakfast everyday in NE school was higher than that in Control school (96.9 vs. 80.3, and 89.2 vs. 75.4 %, respectively). (p < 0.05).
Conclusions
This nutrition education programme is effective in improving adolescents’ knowledge, attitudes, and behaviour in relation to nutrition; therefore, the nutrition education with interactive and innovative intervention components is strongly recommended for future nutrition promotion programmes for adolescents.
Similar content being viewed by others


Introduction
Overweight and obesity are, globally, the fifth leading risks for mortality. At least 2.8 million adults die each year as a result of being overweight or obese. In addition, 44 % of the diabetes burden, 23 % of the ischaemic heart disease burden, and between 7 and 41 % of certain cancer burdens are attributable to overweight and obesity [1]. While many nutrition-related chronic diseases such as cardiovascular disease (CVD), non-insulin-dependent diabetes mellitus (NIDDM) and certain types of cancer may only appear in adult life, they are associated with dietary and lifestyle risk factors developed during childhood and adolescence, many of which are associated with obesity. Studies suggest that obesity tracks into adulthood if it is present in adolescence [2]. Further, studies also indicate that adolescents are a nutritionally vulnerable group for a number of reasons, including their high nutrition requirements for growth, their eating patterns and lifestyles, their risk-taking behaviours and their susceptibility to environmental influences [3, 4]. Therefore, the promotion of nutrition from adolescence plays a vital long-term role in maintaining lifelong health.
China, the largest developing country in the world, currently faces a variety of health challenges, one of these being that nutrition problems in adolescence pose a significant and growing challenge in many parts of the country [5]. For example, the Chinese Center for Disease Control and Prevention reported that around 120 million youth under 18 years were obese in China. Also, the Obesity Review released by International Obesity Research Association reported that in China, the obesity rate of children was 12 %; worse, among the teenagers under 17 years, 1/3 of them had demonstrated at least one risk factor for cardiovascular diseases [6]. Also, recent statistics released by the Chinese Capital Institute of Pediatrics showed that among youth under 18 years in Beijing, 20 % were overweight or obese and that the obesity rate had increased five- to sevenfold over the past 20 years [7]. China is the most populous country in the world, with 1.37 billion people (2010), of whom about 200 million are adolescents, accounting for about 14.8 % of the total population [8]. Hence, adolescents’ nutrition and health in China form an indispensable and essential part for the sustainable development of adolescents themselves and the country as a whole, and accordingly should receive special attention.
Furthermore, the National Survey on Nutrition among Children Aged 0–6 Years (2012) reported that the rate of underweight and stunning among children in rural areas was three to four times higher than that in urban areas. Worse, the obesity rate of children in urban and rural areas was 8.5 and 6.5 %, respectively, with a more significant increase among children in rural areas [9]. The above data indicated that both under- and over-nutrition problems in adolescents are serious especially in rural areas of China, and should be a priority in future nutrition promotion initiatives. However, there is very limited published research focusing on improving adolescents’ nutrition in rural areas of China. Fortunately, previous studies have demonstrated that effective nutrition education gives individuals an easier access to nutrition information and facilitates them to develop healthy attitudes and behaviours [10]. In view of this, the purpose of this study was to examine whether this nutrition education programme is effective to improve adolescents’ knowledge, attitudes and behaviour in relation to nutrition in rural areas of China. If it is, there is a strong argument to use this strategy to promote nutrition among adolescents in rural areas of China. Our hypothesis is that a systematic nutrition education program is effective in improving adolescents’ knowledge, attitudes and behaviour in relation to nutrition in rural areas of China.
Materials and methods
This study received ethical clearance approval both from Griffith University (Australia) Human Research Ethics Committee (Reference No: PBH/14/12/HREC) and Peking University (China) Institutional Review Board (Ethics Review Approval No: IRB00001052-12024). Each participant was provided with full information about the study. Informed written consent was obtained both from students and their guardians.
Study design
First, we obtained permission and cooperation from the Education Committee of the Mi Yun County authorities to allow us to conduct the research. And then a cluster-randomised intervention trial design was employed to examine the effect of this nutrition education programme on students’ knowledge, attitudes and behaviour in relation to nutrition. Two schools were randomly selected from 15 middle schools in rural areas of Mi Yun County, Beijing, to participate in the survey. These two schools were then randomly assigned to either the school with the nutrition education intervention (NE school) or to the school without our nutrition education intervention (Control school). Knowledge, attitudes and behaviours in relation to nutrition were measured at baseline/pre-intervention survey and at post-intervention survey using the same instrument. The pre-intervention survey was conducted in July 2012, the nutrition education was implemented from September 2012 to May 2013 (altogether 6 months, excluding Winter Holidays) and the post-intervention survey was conducted in June 2013.
Sample
The participants were seventh grade students in rural middle schools in Mi Yun County, Beijing. Middle schools in China contain three grades, from grade seven to grade nine. Because the grade eight students would upgrade to grade nine after the baseline survey, and because students needed to prepare for the entry examination for high schools during this year, we considered that the extensive academic pressure would preclude them from participating in the intervention with enthusiasm and energy, we excluded this group from our study. The grade nine students would graduate from middle schools and go to different high schools (from grade ten to grade twelve) after the baseline survey, so bearing in mind the difficulty of tracing them we also excluded this group from our study.
The calculation formula for comparing the rate between two separate samples was used to calculate the sample size:
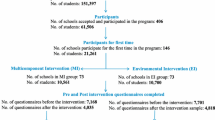
where n 1 and n 2 are the sample size in each group, p 1 and p 2 are the estimate rate of each group, u α and u β are the u value as α is the significant level and β is the possibility of making the second type of error [11]. In our study, we used the awareness rate of nutrition knowledge as the indicator; we estimated the mean awareness rate of each nutrition knowledge item in NE school and in Control school as 80 and 50 %, respectively, after intervention, so p 1 = 0.8 and p 2 = 0.5. We set α = 0.05, β = 0.1, u 0.05/2 = 1.96, u 0.1 = 1.282, and accordingly n 1 = n 2 = 50.7. Each school required a minimum number of 51 students as subjects. To satisfy these requirements and to allow for dropouts, we asked 65 students in each school to complete the pre-and post-intervention questionnaires. In all, 126 students completed both the pre- and post-intervention questionnaires, with a response rate of 96.9 %.
Instrument
The instrument for the study was a 27-item, self-administered, structured questionnaire, designed in Chinese. The questionnaire was divided into four main sections to assess respondents’ demographic characteristics and their knowledge, attitudes and behaviour in relation to nutrition. Section A (personal information) and section C (food frequency consumption) were derived from the questionnaire used in the 2004 China Adolescent Behavioral Risk Factor Survey, designed by the Institute of Child and Adolescent Health, Peking University. Section C examined respondents’ food frequency consumption aimed at investigating weekly frequency of consumption of fresh fruit, vegetables, dairy products, breakfast, dessert, fried food and soft drinks. This questionnaire had been pre-tested on a small sample before its wide use in China [12]. Section B (nutrition knowledge) was derived from two English questionnaires, which comprised ten nutrition knowledge items, each with five response categories structured in different ways. The nutrition knowledge items included the main function of necessary nutrients; which food was richer in certain nutrients; and the symptoms and causes of food poisoning. The mean Cronbach’s alpha scores was 0.73 [13] and 0.57, with a test–retest reliability of 0.80 [14]. It was translated by a Chinese, who had a Bachelor Degree of Arts, majored in English and then engaged in research focusing on nutrition promotion. So she is proficient both in Chinese and English and familiar with the terms on nutrition. Section D (attitudes towards nutrition) was designed by relevant experts; it investigated students’ attitudes towards nutrition, healthy dietary habits and food with an expired consumption date, and the mean Cronbach’s alpha score of this section was 0.665.
Each questionnaire took about 20 min to complete. Standardization of the questionnaire was also ensured by carrying out a pilot study on 70 students in a school randomly selected from the same rural areas (Mi Yun County) as the main study. Following the pilot study, minor adjustments, such as deleting unnecessary options in the questions and simplifying the language, were made to the questionnaire, prior to commencement of the study. The questionnaire was completed in the classroom. The investigator, who was in charge of collecting the questionnaires, was a Chinese national fluent in Mandarin, who had received prior training about skills of conducting a survey.
Interventions
The NE school undertook a nutrition education, which included three components: conducting in-class nutrition curriculum, organizing peer support activities and distributing knowledge brochures. The Control school did not receive the above nutrition education. The core component of the intervention in the NE school was determined according to the 2011 Chinese Residents Dietary Guidelines [15], which include the definition and importance of a balanced diet, the functions of the nutrients, nutrient deficiencies and their effects, how to supplement necessary nutrients reasonably, good hygienic practices and food safety.
To be specific, we held an in-class nutrition curriculum for students once every week (altogether 26 sessions). To make it feasible and efficient, we incorporated this 15 min in-class nutrition curriculum into a regular 40-min class. Fifteen minutes per week does not take a long time, and it does not affect students’ normal learning, so the school authorities were willing to approve and to cooperate in this. On the other hand, the in-class nutrition curriculum was a part of regular class, so we did not need to find an extra suitable place for it. All students attended, and accordingly it lowered the running cost and guaranteed a high attendance rate. In addition, we asked a teacher who already taught the target students in the school to help us to give the in-class nutrition curriculum, to make students feel comfortable with the learning environment and absorb the information given. To guarantee the quality of this in-class nutrition curriculum, we gave teachers training on nutrition knowledge and teaching skills and arranged an oral examination on training outcomes prior to the intervention.
In addition, taking into account the feasibility and appropriateness, we organised peer support activity for students once every month (altogether 6 times), which we considered the maximum load for motivated participation as each peer support activity took about 30 min. To avoid wasting students’ time during the peer support activity, and to boost efficiency, we provided the form and topic of each peer support activity to students a week earlier to allow them to prepare by, for example, gathering relevant information, making presentation cards, or rehearsing the debate. During the process of the peer support activity, students could seek help or guidance from a teacher if they wanted, but the teacher was not allowed to interfere or change the way students behaved. This approach guaranteed that students were able to conduct their own peer support activity independently for maximum effect and obtain necessary instructions to disseminate correct information at the same time. Further, we also encouraged students in the same group to share their experience and help each other in daily life, not only during the peer support activity, to strengthen their bond and connection with each other.
Restricted by limited funds and limited human resources, this study selected a nutrition-related knowledge brochure as the main promotional material. We distributed a three-page nutrition knowledge brochure to students twice: the first in September 2012 and the second in December 2012.
Statistical analysis
Using Epidata 3.02 software, data were coded and entered onto a computer, and then logical error detection and verification were carried out to exclude missing data and abnormal values. We conducted all of the statistical analysis procedures using the Statistical Package for Social Science version 20.0 (SPSS 20.0). We used an alpha level of 0.05 to determine the statistical significance of the data. The data collected from the pre- and post-intervention surveys were paired and compared.
First, students’ socio-demographic characteristics were described. We used mean and standard deviation to summarise students’ ages; frequency was calculated to describe the students’ gender and nationality. Analysis of variance was used to identify whether there was a statistical difference in the students’ age between two schools, and the Chi square test was used to identify whether there was a statistical difference in the students’ gender and nationality between two schools before the interventions. Then, frequency was calculated to compute students’ awareness rate of each of the ten nutrition knowledge items, the expected attitudes towards nutrition, healthy dietary habits, and food with an expired date and the adoption rate of each of the seven healthy eating behaviours in pre- and post-intervention surveys. Chi square test was used to identify whether there was a significant difference in students’ awareness rate of nutrition knowledge items, their attitudes towards nutrition and their adoption rate of healthy eating behaviours over the previous 7 days between two schools before and after interventions. When conducting Chi-square test, if the number of cells that contained actual counts less than 5 was more than 20 % of the total number of the cells, then we would combine some cells into one cell. If all the expected counts were more than 5 in a table, we would display the results from Pearson Chi-square analysis. If the expected counts were between 1 and 5 in a table, we would display the results from continuity correction analysis.
Results
Sample characteristics
The total number of students who completed the survey was 126, with 65 from the NE school and 61 from the Control school, with 61 males (48.4 %) and 65 females (51.6 %). The mean age for the respondents was 12.8 ± 0.4 years, with ages ranging from 12 to 14 years; 88.1 % of the respondents were Han nationality, and 11.9 % were minorities. There was no statistically significant difference in student’s age, gender and nationality between the NE school and the Control school.
Nutrition knowledge
Table 1 displays the awareness rate of the ten knowledge items among students in the NE school and in the Control school at the pre- and post-intervention survey. It shows that there were no significant differences in the following five items: ‘the main function of dairy products is to build strong teeth and bones’, ‘the main function of vegetables is to protect against infections’, ‘dairy products and beans are richer in Calcium’, ‘meat is richer in protein’, and ‘the symptoms of food poisoning depend on the types of causative germ’, between the NE school and the Control school before intervention, however, there were significant differences in students' awareness rate of these five knowledge items between the NE school and Control school after the intervention (P < 0.05). These results indicated that students' awareness of these five knowledge items improved significantly after the intervention in the NE school.
Attitudes towards healthy dietary intake and nutrition
Table 2 shows that there were no significant differences in students' attitudes towards the importance of nutrition to health and how to deal with the food with an expired date between the NE school and the Control school before the intervention. However, there were significant differences in students' attitudes towards these two items between the NE school and the Control school after the intervention (P < 0.05). These results indicated that the intervention had a positive influence on students' attitudes towards the importance of nutrition to health, and towards the correct way to deal with the food with an expired date.
Eating behaviour
Table 3 shows that for the behaviour of ‘eating vegetables every day’ and ‘eating breakfast every day’, there was no significant difference among students between the NE school and the Control school before intervention; however, there was a significant difference between the NE school and the Control school after intervention (P < 0.05), which indicated that the intervention had increased the rate of eating vegetables and breakfast everyday among students.
Discussion
The purpose of this study was to assess whether this school-based nutrition education programme is effective to improve adolescents’ knowledge, attitudes and behaviour in relation to nutrition in rural areas of China. The results showed that some of adolescents’ knowledge, attitudes and behaviour in relation to nutrition improved significantly after this 6-month nutrition education, which demonstrates that this nutrition education program is effective to promote adolescents’ nutrition in rural areas of China. These findings are consistent with the results of previous studies, which showed that school-based nutrition interventions can play a major role in dietary change among adolescents because the amount of time young people spend at school and the large percentage of food they consume there, parental influence on diet decreases and the food provided in schools and the influence of peers become more important [16–18]. Also, nutrition education has been widely integrated into the formal curriculum for many years. After recognising the importance of helping students to acquire accurate and age-related knowledge and to develop their healthy dietary habits and behaviours, nutrition education has incorporated more interactive and participative components to improve students' nutrition [19, 20]. In view of these, our study tried to design and conduct more adolescent-oriented nutrition education intervention in this school-based nutrition program.
Contemporary curriculum is beginning to share time in classrooms with more active learning that emphasises the audiences’ interests, experiences, problem solving, discussion, presentation and other learning-by-doing activities. At the same time, students continue to need information, facts, concepts and context—to engage meaningfully in these activities [21]. Our programme tried to increase interactivity as a part of the in-class nutrition curriculum because many studies have demonstrated that teaching students using interactive class pedagogy can improve their retention of knowledge [22, 23]. For example, in our study, students were allowed to ask questions at any time during the class hours and the teacher would give them an immediate feedback. Besides, during the class hour, the teacher asked students to discuss a nutrition issue within a group and provided them with an opportunity to communicate and learn from each other. Such interactivity is relatively uncommon in Chinese schools where a didactic pedagogy is more typical [24–26]. Our strategies, which included incorporating a nutrition curriculum into a regular class, giving lessons by a trained teacher with whom students are familiar and increasing the interactivity of the class, are undoubtedly crucial factors contributing to the positive impact of this nutrition education program on students’ nutrition. Such learning strategies provide an effective example of curriculum development that can be used in future nutrition programs.
We selected peer support activity as a key intervention component because previous studies have demonstrated that peer support is an effective intervention for a variety of populations, with beneficial effects across a wide spectrum of health outcomes. For example, peer support has been found to be effective in increasing breast-feeding duration; improving self-efficacy and well-being in individuals with heart disease; improving fitness, strength, and sport competence for breast cancer survivors; enhancing mental health; and increasing chronic disease management and health-related quality of life [27–30]. Additionally, peer support is especially vital and influential to adolescents, as they spend increased time with peers, enhancing the potential for the norms and behaviours of peers to influence them [31, 32]. While it is true that peers influence each other across the whole life span, the effects of peer influence, however, are stronger during adolescence than other stages of life [33, 34]. Moreover, we gave the students adequate time to prepare before the peer support activity to establish their peer connections; enough autonomy and necessary guidance during the peer support activity to deepen the peer relations; and ongoing encouragement after the peer support activity to maintain peer bonds. These are also the reasons why our intervention can be effective. In a word, peer support has a clear potential to improve adolescents’ nutrition and the strategies used in our study, namely building, strengthening and keeping peer connection and bonds to guarantee the effect of the peer support activities were found to be effective and feasible and could be profitably employed and advocated in future nutrition programmes. Moreover, the long-term and sustainable effect of peer support for adolescent groups should be explored as peers can influence an individual throughout his or her whole life.
Finally, the promotional material used is significant. The material takes many forms and its diversity ranges from mass media TV messages to written texts in materials such as advertisements, information leaflets and more comprehensive brochures [35]. Due to the limitation of funds, this study only selected a nutrition knowledge brochure as the main promotional material. However, future promotional materials should be planned, designed and developed in accordance with the characteristics of adolescents, as style and taste in such promotional materials may quickly become outdated. Trends change among this group more quickly than any other segment in our society [36]. Particular attention to the most current graphic trends and communication styles is critical in achieving and holding the interest of young people. So promotional materials need to be constantly updated, including more photographs, and employ bright colors and more unique shapes [37]. Most of all, the materials need to speak the target population’s language and relate to their circumstances and social context [38]. Also, with the advent of new technologies, such as social media, researchers should include new elements of technology in the development of promotional materials. For example, a study has found that the effectiveness of the multimedia textbook was greater than that of the traditional printed textbook. Multimedia textbooks are similar to conventional books but differ in function in that they contain video and audio clips and animation that allow the reader to interact dynamically with the content [39, 40]. In summary, to make promotional materials effective for adolescents, high-quality promotional materials which are oriented to adolescents, speak adolescents’ language and include new technology elements should be designed and developed in future research.
Conclusion
This study has found that a well-designed nutrition education programme is effective in improving adolescents’ knowledge, attitudes and behaviour in relation to nutrition, in rural areas of China. The traditional education components—in-class nutrition curriculum and promotional materials delivery, which have generally been acknowledged as being insufficient to generate positive behaviour change, also played an important role in supporting and enhancing the effectiveness of our intervention because we had integrated various participative and interactive elements into them. In addition, our intervention also incorporated other components, such as peer support activity, to generate more positive and significant change not only on adolescents’ knowledge, but also on their attitudes and behaviours and eventual health outcome. Therefore, our nutrition education programme combined with a variety of interactive, participative and innovative intervention components is strongly recommended for future nutrition promotion programs.
References
http://www.who.int/mediacentre/factsheets/fs311/en/. Accessed 23 Nov 2014.
World Health Organization. Nutrition in adolescence: issues and challenges for the health sector: issues in adolescent health and development. Geneva: WHO Press; 2005.
Perry-Hunnicuft G, Newman IM. Adolescent dieting practices and nutrition knowledge. Health Values. 1993;17:35–40.
Forthing MC. Current eating patterns of adolescents in the United States. Nutr Today. 1991;26:35–9.
Wang D, Shi Y, Chang C, Stewart D, Ji Y, Wang Y, Harris N. Knowledge, attitudes and behaviour regarding nutrition and dietary intake of seventh-grade students in rural areas of Mi Yun County, Beijing, China. Environ Health Prev Med. 2014;19:179–86.
http://news.xinhuanet.com/health/2012-08/31/c_123654322.htm. Accessed 31 Jan 2015.
http://news.xinhuanet.com/edu/2011-03/29/c_121244536.htm. Accessed 31 Oct 2014.
Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int. 2000;15:259–67.
Sun ZQ. Medical statistics. Beijing: People’s Medical Publishing House; 2005.
Ji CY. The report of health-related and health risk behaviours among Chinese adolescents in 2005. Beijing: Peking University Medical Press; 2007.
Oldewage-Theron WH, Egal AA. Nutrition knowledge and nutritional status of primary school children in QwaQwa. S Afr J Clin Nutr. 2010;23:149–54.
Turconi G, Celsa M, Rezzani C, Biino G, Sartirana MA, Roggi C. Reliability of a dietary questionnaire on food habits, eating behaviour and nutritional knowledge of adolescents. Eur J Clin Nutr. 2003;57:753–63.
China’s Minister of Health. Chinese residents dietary guidelines (2011). Tibet: The Tibet People’s Publishing House; 2011.
Wang D, Stewart D. The implementation and effectiveness of school-based nutrition promotion programmes using a health promoting schools approach: a systematic review. Public Health Nutr. 2013;16:1082–100.
Wang D, Stewart D, Yuan Y, Chang C. Do health-promoting schools improve nutrition in China? Health Promot Int. 2013;. doi:10.1093/heapro/dat047.
Louise R, Oddrun S. Filling the black box of implementation for health-promoting schools. Health Educ. 2011;111:347–62.
Wang D, Stewart D, Chang C, Ji Y, Shi Y. Effect of interventions to improve adolescents’ nutrition knowledge in China. Health Educ. 2014;114:322–30.
Mohammadi NK, Rowling L, Nutbeam D. Acknowledging educational perspectives on HPSs. Health Educ. 2008;110:240–51.
Bransford JD, Brown AL, Cocking RR. How people learn: brain, mind, experience and school. Washington, DC: National Academy Press; 1990.
Gass S, Varonis E. Input, interaction, and second language production. Stud Second Lang Acquis. 1994;16:283–302.
Morell T. Interactive lecture discourse for university EFL students. Engl Specif Purp. 2004;23:325–38.
Bransford JD, Brown AL, Cocking RR. How people learn: brain, mind, experience and school. Washington, DC: National Academy Press; 1990.
Baram-Tsabari A, Yarden A. Characterizing children’s spontaneous in science and technology. Int J Sci Educ. 2005;27:803–26.
Hagay G, Baram-Tsabari A. A shadow curriculum: incorporating students interest into the formal biology curriculum. Res Sci Edu. 2011;41:611–34.
Dennis CL, Hodnett E, Gallop R. The effect of peer support on breast-feeding duration among primiparous women: a randomized controlled trial. Can Med Assoc J. 2002;166:21–8.
Hibbard MR, Cantor J, Charatz H. Peer support in the community: initial findings of a mentoring program for individuals with traumatic brain injury and their families. J Head Trauma Rehabil. 2002;17:112–31.
Ley A, Robert G, Willis D. How to support peer support: evaluating the first steps in a healthcare community. J Public Ment Health. 2010;9:16–25.
Gottlieb BH, Wachala ED. Cancer support groups: a critical review of empirical studies. Psychooncology. 2007;16:379–400.
Smith AL. Peer relationships in physical activity contexts: a road less travelled in youth sport and exercise psychology research. Psychol Sport Exerc. 2003;4:25–39.
Morris BA, Chambers SK, Campbell M. Motorcycles and breast cancer: the influence of peer support and challenge on distress and posttraumatic growth. Support Care Cancer. 2012;20:1849–58.
Campbell H, Phaneuf MR, Deane K. Cancer peer support programs—do they work? Patient Educ Couns. 2004;55:3–15.
Fitzgerald A, Fitzgerald N, Aherne C. Do peers matter? A review of peer and/or friends’ influence on physical activity among American adolescents. J Adolesc. 2012;35:941–58.
Kools M, Ruiter RAC, van de Wiel MWJ, Margaretha WJ, Kok G. Increasing readers comprehension of health education brochures: a qualitative study into how professional writers make texts coherent. Health Educ Behav. 2004;31:720–40.
Armstrong JJ, Lumsden DB. Impact of universities promotional materials on college choice. J Mark High Educ. 1999;9:83–91.
Kools M, van de Wiel MWJ, Ruiter RAC. The effect of graphic organizers on subjective and objective comprehension of a health education text. Health Educ Behav. 2006;33:360–72.
Kools M, van de Wiel MWJ, Ruiter RAC. Pictures and text in instructions for medical devices: effects on recall and actual performance. Patient Educ Couns. 2006;64:104–11.
Wofford MM, Spickard AW, Wofford JL. The computer-based lecture. Innov Educ Clin Pract. 2001;16:464–7.
Santer DM, Michaelsen VE, Erkonen WE. A comparison of educational interventions. Arch Pediatr Adolesc Med. 1995;149:297–302.
Acknowledgments
This study was funded by the Grant for Higher Research Degree students in School of Public Health, Griffith University (AUS$3000). Griffith University had no role in the design, analysis or writing of this article.
Conflict of interest
The authors declare no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Wang, D., Stewart, D., Chang, C. et al. Effect of a school-based nutrition education program on adolescents’ nutrition-related knowledge, attitudes and behaviour in rural areas of China. Environ Health Prev Med 20, 271–278 (2015). https://doi.org/10.1007/s12199-015-0456-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12199-015-0456-4