
Abstract
Objective
To determine the outcomes in children with MIS-C receiving different immunomodulatory treatment.
Methods
In this multicentric, retrospective cohort study, data regarding treatment and outcomes of children meeting the WHO case definition for MIS-C, were collected. The primary composite outcome was the requirement of vasoactive/inotropic support on day 2 or beyond or need of mechanical ventilation on day 2 or beyond after initiation of immunomodulatory treatment or death during hospitalization in the treatment groups. Logistic regression and propensity score matching analyses were used to compare the outcomes in different treatment arms based on the initial immunomodulation, i.e., IVIG alone, IVIG plus steroids, and steroids alone.
Results
The data of 368 children (diagnosed between April 2020 and June 2021) meeting the WHO case definition for MIS-C, were analyzed. Of the 368 subjects, 28 received IVIG alone, 82 received steroids alone, 237 received IVIG and steroids, and 21 did not receive any immunomodulation. One hundred fifty-six (42.39%) children had the primary outcome. On logistic regression analysis, the treatment group was not associated with the primary outcome; only the children with shock at diagnosis had higher odds for the occurrence of the outcome [OR (95% CI): 11.4 (5.19–25.0), p < 0.001]. On propensity score matching analysis, the primary outcome was comparable in steroid (n = 45), and IVIG plus steroid (n = 84) groups (p = 0.515).
Conclusion
While no significant difference was observed in the frequency of occurrence of the primary outcome in different treatment groups, data from adequately powered RCTs are required for definitive recommendations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Multisystem inflammatory syndrome in children temporally associated with SARS-CoV-2 (MIS-C) has emerged as a global child health issue. Various scientific bodies like the CDC, RCPCH, and WHO released their guidance documents in this context during April–May 2020 [1,2,3]. After the early reports from Italy, documenting a spurt in cases presenting with Kawasaki disease–like spectrum, hundreds of publications across the globe including India described similar features [4,5,6]. The novelty of this disease poses many challenges in formulating the treatment guidelines. Given the similarity of MIS-C with Kawasaki disease and the macrophage activation syndrome complicating many rheumatic disorders, intravenous immunoglobulin (IVIG) and steroids formed the sheet anchor for MIS-C management. Early guidance for management of MIS-C from the American College of Rheumatology advocated immunomodulation using IVIG and steroids, and anakinra for refractory cases [7]. However, there is lack of high-quality evidence to guide the choice of initial therapy in MIS-C.
Further, the nature of the disease poses a challenge in conducting randomized controlled trials to generate a high level of evidence. One pragmatic approach is to analyze the available data from observational studies using various statistical techniques such as propensity score matching, as has been done in recent studies [8,9,10]. However, these data are mainly from developed nations. The developing world settings are challenged with multiple factors such as cost constraints with the use of IVIG, non-availability of biologics like anakinra, and the high background rate of infections with overlaping features similar to MIS-C.
In the present work, the data of children with MIS-C from seventeen centers across India were collated and analyzed to compare the outcome in the different treatment arms (IVIG alone, IVIG plus steroids, and steroids alone).
Material and Methods
This retrospective cohort study is an analysis of data collected from different participating centers in India. A formal invitation to participate in the study through email was sent to 21 centers, of which seventeen sites participated in this study. The Institute Ethics Committee approved the study of the coordinating site (IEC-487/02.07.2021). All participating centers also obtained ethical clearance from their respective ethics committees.
A data extraction form was developed and shared with all participating sites and finalized after inputs from all. The information about the demographic profile, clinical features, criteria for diagnosis of MIS-C, laboratory investigations, treatment received (including details of immunomodulatory treatment: IVIG / steroids / IVIG + steroids / biological, vasoactive drugs, and respiratory support) and the outcome was sought. The data from each center were collected by one of the treating physicians at each site. The data were entered in a predesigned form using MS Access or MS Excel, circulated from the coordinating site. Data from one center were received in hard copy, which was later, filled in the Excel sheet. Data from various sites were merged; if any difference in the units of laboratory variables was found, those were modified to standard units for uniformity. The outcomes of interest were calculated from the data provided. The de-identified data of children with MIS-C as per WHO case definition [3], admitted (between April 2020 and June 2021) at participating centers were eligible for inclusion in the study. The subjects for whom the data pertaining to the primary outcome were missing, were excluded from this study.
Based on the immunomodulatory treatment received, the patients were categorized into four groups: IVIG alone; steroids alone; IVIG plus steroids; and one group where patients did not receive immunomodulation.
The primary outcome was the requirement of vasoactive/inotropic support on day 2 or beyond or need of mechanical ventilation on day 2 or beyond after initiation of immunomodulatory treatment or death during hospitalization in the treatment groups. The baseline cardiac outcomes (ejection fraction, coronary dilation/aneurysm) in different treatment groups were also compared. The coronary aneurysms were defined as per coronary size estimations using the standard norms [11].
Data were entered in a Microsoft Access or MS Excel forms by each of the participating centers. Data were collated by the coordinating center and checked for missing data and formatting. RL and NKB screened the data for accuracy and completeness, and the respective sites were contacted in case of any discrepancies. The cleaned dataset was analyzed using Stata software (StataCorp, College Station, TX). Descriptive statistics were used to summarize parameters in the treatment groups. The outcomes in the treatment groups were compared. Logistic regression analysis was performed to adjust for the differences in the baseline features of the subjects for predicting the primary outcome. A propensity score matching analysis was also performed to match the possible confounding factors which might influence the outcome. Given the limited numbers in the IVIG alone arm, outcomes were compared in the two groups: steroid alone vs. IVIG plus steroid. The details of the methods for propensity score matching analysis are provided in Supplementary material S1.
The patients or public were not involved in the design, or conduct, or reporting, or dissemination plans of the present research.
Results
The seventeen participating sites provided data on children diagnosed with MIS-C between April 2020 and June 2021. The data of 368 subjects meeting the WHO case definition for MIS-C were analyzed for the outcome comparisons.
Of the 368 subjects, 28 received IVIG alone, 82 received steroids alone, 237 received IVIG and steroids, while 21 did not receive any immunomodulation. Among children who received steroids in any of the groups, the type of steroid was mentioned in 281 records; 255 (90.4%) received intravenous methylprednisolone, 18 (6.4%) oral prednisolone, while 8 (2.8%) received dexamethasone. Six children received tocilizumab.
Table 1 summarizes the demographic, laboratory, and treatment details of the study population categorized by the immunomodulatory treatment received. The mean (SD) age of the study population was 80.2 (51.1) mo, majority (62.9%) being boys. In addition to fever, which was universal in all subjects, gastrointestinal symptoms, rash, and shock were the other common presenting features reported in 70.3%, 58.3%, and 53.5% of the subjects, respectively. In this cohort, 225 (61.1%) children received vasoactive/inotropic drug support, while 67 (23%) were mechanically ventilated. The median (IQR) duration of hospital stay was 8 (6, 11) d. Patients who received IVIG alone were significantly younger. Those that received both IVIG and steroids had significantly lower platelet counts, and higher CRP and ferritin.
Table 2 summarizes the baseline cardiac parameters. The mean ejection fraction at baseline was significantly lower in the group receiving both IVIG plus steroids than other treatment groups. Seven children had coronary dilation at baseline, while 25 had coronary aneurysms; there was no difference in the observed frequency of these aneurysms among the various treatment arms.
Forty (10.9%) children succumbed during the hospital stay. The primary outcome occurred in 156 (42.4%) children. The primary outcome occurred more often in the group receiving both IVIG plus steroids (p = 0.027) (Table 3).
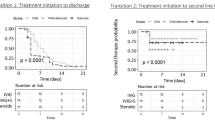
On logistic regression analysis to assess the association between the treatment groups and the outcome adjusting for other factors, the treatment groups did not seem to have an effect on the primary outcome; only children with shock at diagnosis had higher odds for the occurrence of the composite outcome [OR (95% CI): 11.4 (5.19–25.0), p < 0.001] (Table 4). The results were similar when the outcome was compared among the three treatment groups after omitting the ‘no immunomodulatory treatment’ group. There was no difference in the primary outcome in the steroid, and IVIG plus steroid groups (p = 0.1). When the data were analyzed using propensity score analysis comparing the primary outcome in steroid (n = 45) and IVIG plus steroid (n = 84) groups, no difference was observed (p = 0.515) (Supplementary material S1).
Discussion
The present multicentric study from a resource-limited setting in children with MIS-C reports the effect of various therapeutic options (IVIG alone, IVIG plus steroids, and steroids alone) on the outcome. The choice of initial immunomodulation was not associated with the outcome in the present study. Children presenting with shock at diagnosis had higher odds for the occurrence of the primary outcome [OR (95% CI): 11.4 (5.19–25.0), p < 0.001]. The data were analyzed using propensity score analysis to compare the primary outcome in steroid and IVIG plus steroid groups. No discernible difference was observed in the outcomes (p = 0.515). The small number of patients in the IVIG alone group precluded us from making definitive conclusion about efficacy of this intervention.
The present findings are similar to that of the study by McArdle et al., who did not observe any difference in the composite outcome (composite of inotropic support or mechanical ventilation by day 2 or later or death) in multicentric international cohort of 614 children, among IVIG alone, IVIG and steroids, and steroids alone groups [10]. They did not observe any difference in the temporal dynamics of disease severity (inflammatory markers, escalation of immunosuppression) in the groups. Although the sequential severity of illness was not analysed in the present study, the trend seems to be unaffected by the initial immunomodulation, as inferred from the comparable mean duration of inotropic support and mechanical ventilation in the different treatment arms.
On the other hand, Son et al. evaluated 518 children with MIS-C and reported that IVIG plus steroids were associated with a lower risk of cardiac dysfunction than IVIG alone [9]. Similarly, a retrospective study in a French cohort with 181 children also showed a favorable outcome in terms of early defervescence, the requirement of inotropic support, and duration of intensive care stay in the group receiving both IVIG and methylprednisolone as compared to IVIG alone [8]. However, there were differences in the predefined primary outcomes of these studies [10,11,12]; cardiac dysfunction or shock on or after day 2 in the study by Son et al. [9]; the persistence of fever 2 d after the introduction of initial therapy or recrudescence of fever within 7 d in the French cohort [8], compared to the composite outcome (requirement of vasoactive/inotropic support for ≥ 2 d or need of mechanical ventilation ≥ 2 d after initiation of immunomodulatory treatment or death during hospitalization), in the Best Available Treatment Study (BATS) by McArdle et al [10]. In the present study, death was also included as a primary outcome.
No difference in the outcome based on the treatment groups was observed on logistic regression analysis. Further, while using propensity score matching analysis, the outcome was comparable in the group receiving IVIG plus steroids and steroid alone, even though only two groups could be matched and that too in small numbers. This observation is of relevance given the cost and availability of IVIG. Even the recent WHO living guidance for MIS-C without Kawasaki phenotype suggests use of corticosteroids in addition to supportive care rather than either IVIG plus supportive care or supportive care alone [13]. These guidelines must, however, be viewed with the caveat that they are based on observational studies rather than randomized controlled trials.
The mortality observed in the present study subjects is strikingly higher than other large series from developed nations (10.87% vs. 1%–2%). High mortality (27.5%) has also been reported from a single-center study from India, which has not participated in the present study [12].
Although the present study was not aimed to study the predictors of mortality, the authors speculate that the high mortality in the present study settings may be attributed to poor access to tertiary care hospitals, delay in seeking care, and high background infection rates in tropical countries posing a diagnostic challenge for MIS-C. In addition, nonavailability/affordability of biological agents like anakinra and tocilizumab in resource-limited settings might also have contributed to these differences; 22/614 (3.5%) and 107/518 (20.6%) children received a biological agent in the studies by Son et al. and McArdle et al., respectively [9, 10]. In contrast, only 6 subjects received a biological in the present study.
The present study has certain limitations; most of these are due to the retrospective nature of the study. The propensity score analysis was used but the matching could be achieved only for a small proportion in two of the treatment groups. In addition, the factors, which might have influenced the decision to choose the initial immunomodulation, and thus, affected the outcome, were not assessed. The variability in the services/practices at various participating centers, such as use of vasoactive agents, tapering strategies, etc. was not studied; all the participating centers were tertiary care institutions with pediatric intensive care services. Owing to a lack of data, the number of children meeting classification for macrophage activation syndrome and long-term cardiac and coronary results were not studied. Also, the effect of different doses of steroids on the outcome was not analyzed.
Conclusion
No difference was observed in the outcomes in children with MIS-C with different immunomodulation therapies. However, more extensive studies, including adequately sized RCTs are needed to establish the best therapeutic option for managing MIS-C, particularly in resource-limited settings.
Data Availability
On reasonable request.
References
Centers for Disease Control and Prevention. Emergency preparedness and response: Multisystem inflammatory syndrome in children (MIS-C) associated with coronavirus disease 2019 (COVID-19). Health advisory. Available at: https://emergency.cdc.gov/han/2020/han00432.asp. Accessed on 22 May 2021.
Royal College of Paediatrics and Child Health. Guidance: paediatric multisystem inflammatory syndrome temporally associated with COVID-19. Available at: https://www.rcpch.ac.uk/sites/default/files/2020-05/COVID-19-Paediatric-multisystem-%20inflammatory%20syndrome-20200501.pdf. Accessed on 22 May 2021.
World Health Organization. Multisystem inflammatory syndrome in children and adolescents with COVID-19- Scientific Brief. Available at: https://apps.who.int/iris/rest/bitstreams/1277962/retrieve. Accessed on 22 May 2021.
Verdoni L, Mazza A, Gervasoni A, et al. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: an observational cohort study. Lancet. 2020;395:1771–8.
Abrams JY, Oster ME, Godfred-Cato SE, et al. Factors linked to severe outcomes in multisystem inflammatory syndrome in children (MIS-C) in the USA: a retrospective surveillance study. Lancet Child Adolesc Health. 2021;5:323–31.
Jain S, Sen S, Lakshmivenkateshiah S, et al. Multisystem inflammatory syndrome in children with covid-19 in Mumbai, India. Indian Pediatr. 2020;57:1015–9.
Henderson LA, Canna SW, Friedman KG, et al. American college of rheumatology clinical guidance for multisystem inflammatory syndrome in children associated with SARS-CoV-2 and hyperinflammation in pediatric COVID-19: Version 1. Arthritis Rheumatol. 2020;72:1791–805.
Ouldali N, Toubiana J, Antona D, et al. Association of intravenous immunoglobulins plus methylprednisolone vs immunoglobulins alone with course of fever in multisystem inflammatory syndrome in children. JAMA. 2021;325:855–64.
Son MBF, Murray N, Friedman K, et al. Multisystem inflammatory syndrome in children — initial therapy and outcomes. N Engl J Med. 2021;385:23–34.
McArdle AJ, Vito O, Patel H, et al. Treatment of multisystem inflammatory syndrome in children. N Engl J Med. 2021;385:11–22.
McCrindle BW, Li JS, Minich LL, et al. Coronary artery involvement in children with kawasaki disease: risk factors from analysis of serial normalized measurements. Circulation. 2007;116:174–9.
Maheshwari A, Mahto D, Kumar V, et al. Comparison of clinical and laboratory profile of survivors and non-survivors of SARS-CoV-2 related multisystem inflammatory syndrome of childhood in India: an observational study. J Paediatr Child Health. 2022;58:136–40.
World Health Organization. Living guidance for clinical management of COVID-19. WHO. Available at: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-clinical-2021-2. Accessed on 2 Mar 2022.
Acknowledgements
Puspraj Awasthi, Prashant Bobhate, Dhaval Darji, Siyaram Didel, Janani G., Yashashwini K., Naresh Kanna, Tanuja Karande, Bhavi Malik, Shiva Manwatkar, Athira P., Chandrakant Pujari, Tulika Rajawat, Harshitha S., Lokesh Saini, Milap Sharma, Chandrakant Pujari, Aliza Mittal, Mousumi Nandy, Vijay, Varuna Vyas, P. K. Wari.
The MIS-C Study Group (in alphabetical order, equal contribution)
Suresh Kumar Angurana, Department of Pediatrics, Advanced Pediatric Center, Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, India; Shally Awasthi, Department of Pediatrics, King George’s Medical University, Lucknow, Uttar Pradesh, India; Harshita Bamnawat, Department of Pediatrics, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India; Javeed Iqbal Bhat, Department of Pediatrics, Sher-i-Kashmir Institute of Medical Sciences, Srinagar, Jammu & Kashmir, India; Tsultem D. Bhutia, Department of Pediatrics, New STNMMS Hospital, Gangtok, Sikkim, India; Bashir Ahmad Charoo, Department of Pediatrics, Sher-i-Kashmir Institute of Medical Sciences, Srinagar, Jammu & Kashmir, India; Abhijit Choudhary, Department of Pediatrics, All India Institute of Medical Sciences, Nagpur, Maharashtra, India; Bharat Choudhary, Department of Pediatrics, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India; Rashmi Ranjan Das, Department of Pediatrics, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India; Bhagirathi Dwibedi, Department of Pediatrics, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India; Sanajit Ghosh, Department of Pediatrics, Medical College Kolkata, Kolkata, West Bengal, India; Meenakshi Girish, Department of Pediatrics, All India Institute of Medical Sciences, Nagpur, Maharashtra, India; Krishna Mohan Gulla, Department of Pediatrics, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India; Jagdish Prasad Goyal, Department of Pediatrics, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India; Prakriti Gupta, Department of Pediatrics, All India Institute of Medical Sciences, Patna, Bihar, India; Shivanand I, Department of Pediatrics, KIMS, Hubbali, Karnataka, India; Atul Jindal, Department of Pediatrics, All India Institute of Medical Sciences, Raipur, India; Joseph John, Department of Pediatrics, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India; Preetha Joshi, Department of Pediatrics, Kokilaben Dhirubhai Ambani Hospital and Medical Research Institute, Mumbai, India; Ravleen Kaur, Department of Pediatrics, Dr Rajendra Prasad Government Medical College Kangra at Tanda, Himachal Pradesh, India; Daisy Khera, Department of Pediatrics, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India; Amit Kumar, Department of Pediatrics, All India Institute of Medical Sciences, Patna, Bihar, India; Pradeep Kumar, Department of Pediatrics, All India Institute of Medical Sciences, Patna, Bihar, India; Prawin Kumar, Department of Pediatrics, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India; A. V. Lalitha, Department of Pediatric Intensive Care, St. John’s Medical College and Hospital, Bangalore, Karanataka, India; Mahesh Maheshwari, Department of Pediatrics, All India Institute of Medical Sciences, Bhopal, India; Shikha Malik, Department of Pediatrics, All India Institute of Medical Sciences, Bhopal, India; Rakesh Mondal, Department of Pediatrics, Medical College Kolkata, Kolkata, West Bengal, India; Jayashree Muralidharan, Department of Pediatrics, Advanced Pediatric Center, Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, India; Gayatri Pawar, Department of Pediatrics, KIMS, Hubbali, Karnataka, India; Arun Prasad, Department of Pediatrics, Medical College Kolkata, Kolkata, West Bengal, India; Sunil Kumar Rao, Department of Pediatrics, Institute of Medical Sciences, BHU, Varanasi, Uttar Pradesh, India; Vinod H. Ratageri, Department of Pediatrics, KIMS, Hubbali, Karnataka, India; Mihir Sarkar, Department of Pediatrics, Medical College Kolkata, Kolkata, West Bengal, India; Amit Kumar Satpathy, Department of Pediatrics, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India; Jhuma Sankar, Department of Pediatrics, All India Institute of Medical Sciences, New Delhi 110029, India; Seema Sharma, Department of Pediatrics, Dr Rajendra Prasad Government Medical College Kangra at Tanda, Himachal Pradesh, India; Ankur Singh, Department of Pediatrics, Institute of Medical Sciences, BHU, Varanasi, Uttar Pradesh, India; Kuldeep Singh, Department of Pediatrics, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India; Tanu Singhal, Department of Pediatrics, Kokilaben Dhirubhai Ambani Hospital and Medical Research Institute, Mumbai, India; Mangla Sood, Department of Pediatrics, IGMC, Shimla, Himachal Pradesh, India; Samsani Veena Sudeepthi, Department of Pediatrics, All India Institute of Medical Sciences, Raipur, India; Lokesh Tiwari, Department of Pediatrics, All India Institute of Medical Sciences, Patna, Bihar, India; Nishant Verma, Department of Pediatrics, King George’s Medical University, Lucknow, Uttar Pradesh, India; Ruth Yonzon, Department of Pediatrics, New STNMMS Hospital, Gangtok, Sikkim, India.
Funding
None.
Author information
Authors and Affiliations
Consortia
Contributions
NKB and RL contributed to the development and design of the study protocol, reviewed the literature, collated and analyzed the data, and wrote the first draft; MK and RMP were the formal data analysts for the study; SKK led the work of the study team; MIS-C study group did data collation, contributed to the study design; all co-authors critically reviewed the paper and approved the submitted version. The corresponding author attests that all listed authors meet authorship criteria. SKK will act as the guarantor for this paper.
Corresponding author
Ethics declarations
Conflict of Interest
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Narendra Kumar Bagri and M. Khan are joint first authors.
The original online version of this article was revised due to the incorrect order of author in HTML version.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Bagri, N.K., Khan, M., Pandey, R.M. et al. Initial Immunomodulation and Outcome of Children with Multisystem Inflammatory Syndrome Related to COVID-19: A Multisite Study from India. Indian J Pediatr 89, 1236–1242 (2022). https://doi.org/10.1007/s12098-022-04254-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-022-04254-5