
Abstract
Purpose
Self-expandable metal stents (SEMS) have been used to manage large bowel obstruction as a palliative treatment or to initially decompress the colon as a bridge to definitive surgery. Our goal was to review clinical outcomes in patients undergoing placement of a SEMS for colorectal obstruction at a tertiary care hospital.
Methods
A retrospective review was done of patients undergoing placement of a colorectal SEMS at a single centre between August 2005 and March 2011 for obstructing lesions. Outcomes identified included clinical relief of obstruction, successful bridging to surgery or palliation, and stent-related complications.
Results
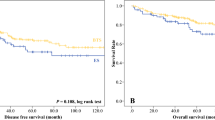
SEMS were placed in a total of 58 patients. The intent of stenting was to bridge to definitive surgery in 11 patients and palliation in 47 patients. Stent placement was clinically successful in relieving obstruction without early complication in 45 (78 %) patients. Of the patients intended to bridge to surgery, 7/11 (64 %) were successfully bridged to surgery. One patient suffered a perforation, two failed to relieve obstruction, and one re-obstructed. Of the patients stented for palliation, 32/47 (68 %) were successfully palliated at a mean follow-up of 7.5 months. Five patients had perforations, six re-obstructed, two had stent migration, and two failed to relieve obstruction. The overall rates for perforation, re-obstruction, and stent migration were 10, 12, and 7 %, respectively.
Conclusion
SEMS placement as a bridge to surgery and for palliation of colorectal obstruction is associated with moderate rates of clinical success but a high rate of perforation.
Similar content being viewed by others

References
Deans GT, Krukowski ZH, Irwin ST. Malignant obstruction of the left colon. Br J Surg. 1994;81(9):1270–6.
Tekkis PP, Kinsman R, Thompson MR, Stamatakis JD. The Association of Coloproctology of Great Britain and Ireland study of large bowel obstruction caused by colorectal cancer. Ann Surg. 2004;240:76–81.
Leitman IM, Sullivan JD, Brams D, DeCosse JJ. Multivariate analysis of morbidity and mortality from the initial surgical management of obstruction carcinoma of the colon. Surg Gynecol Obstet. 1992;174(6):513–118.
Dohmoto M, Rupp KD, Hohlbach G. Endoscopically-implanted prosthesis in rectal carcinoma. Dtsch Med Wochenschr. 1990;115:915.
Spinelli P, Dal Fante M, Mancini A. Self-expanding mesh stent for endoscopic palliation of rectal obstruction tumors: a preliminary report. Surg Endosc. 1992;6:72–4.
Tejero E, Mainar A, Fernandez L, et al. New procedure for the treatment of colorectal neoplastic obstructions. Dis Colon Rectum. 1994;37:1158–9.
Tan CJ, Dasari VM, Gardiner K. Systematic review and meta-analysis of randomized clinical trials of self-expanding metallic stents as a bridge to surgery versus emergency surgery for malignant left-sided large bowel obstruction. Br J Surg. 2012;99:469–76.
Watt AM, Faragher IG, Griffin TT, Rieger NA, Maddern GJ. Self-expanding metallic stents for relieving malignant colorectal obstruction. Ann Surg. 2007;246:24–30.
Sebastian S, Johnston S, Geoghegan T, Torreggiani W, Buckley M. Pooled analysis of the efficacy and safety of self-expanding metal stenting in malignant colorectal obstruction. Am J Gastroenterol. 2004;99:2051–7.
Cheung HY, Chung CC, Tsang WW, Wong JC, Yau KK, Li MK. Endolaparoscopic approach vs conventional open surgery in the treatment of obstruction left-sided colon cancer: a randomized controlled trial. Arch Surg. 2009;144:1127–32.
Ho KS, Quah HM, Lim JF, Tang CL, Eu KW. Endoscopic stenting and elective surgery versus emergency surgery for left-sided malignant colonic obstruction: a prospective randomized trial. Int J Color Dis. 2012;27:355–62.
van Hooft JE, Bemelman WA, Oldenburg B, Marinelli AW, Holzik MF, Grubben MJ, et al. Colonic stenting versus emergency surgery for acute left-sided malignant colonic obstruction: a multicentre randomized trial. Lancet. 2011;12:344–52.
Pirlet IA, Slim K, Kwiatkowski F, Michot F, Millat BL. Emergency preoperative stenting versus surgery for acute left-sided malignant colonic obstruction: a multicentre randomized controlled trial. Surg Endosc. 2011;25:1814–21.
Meisner S, Gonzalez-Huix F, Vandervoort JG, Repici A, Xinopoulos D, Grund KE, Goldburg P, and The Wallflex Colonic Registry Group. Self-expanding metal stenting for palliation of patients with malignant colonic obstruction: Effectiveness and efficacy on 225 patients with 12-month's follow-up. Gastroenterology Research and Practice. doi:10.1155/2012/296347.
Xinopoulos D, Dimitroulopoulos D, Theodosopoulos T, et al. Stenting or stoma creation for patients with inoperable malignant colonic obstructions? Results of a study and cost-effectiveness analysis. Surg Endosc. 2004;18:421–6.
Fiori E, Lamazza A, De Cesare A, et al. Palliative management of malignant rectosigmoidal obstruction. Colostomyvs. Endoscopic stenting. A randomized prospective trial. Anticancer Res. 2004;24:265–8.
van Hooft JE, Fockens P, Marinelli AW, et al. Dutch Colorectal Stent Group. Early closure of a multicenter randomized clinical trial of endoscopic stenting versus surgery for stage IV left-sided colorectal cancer. Endoscopy. 2008;40:184–91.
Pommergaard H, Vilmann P, Jakobsen H, Achiam M. A clinical evaluation of endoscopically placed self-expanding metallic stents in patients with acute large bowel obstruction. Scand J Surg. 2009;98:143–7.
Keswani R, Azar R, Edmundowicz S, et al. Stenting for malignant colonic obstruction: a comparison of efficacy and complications in colonic versus extracolonic malignancy. Gastrointest Endosc. 2009;69:675–80.
Conflict of Interest
The authors declare that no conflicts of interest exist.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Alford, T., Ghosh, S., Wong, C. et al. Clinical Outcomes of Stenting for Colorectal Obstruction at a Tertiary Centre. J Gastrointest Canc 45, 61–65 (2014). https://doi.org/10.1007/s12029-013-9557-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12029-013-9557-8