
Abstract
Introduction
This study was conducted to prospectively evaluate the diagnostic value of detailed neurological evaluation, transcranial Doppler sonography (TCD) and Perfusion-CT (PCT) to predict delayed vasospasm (DV) and delayed cerebral infarction (DCI) within the following 3 days in patients with aneurysmal subarachnoid hemorrhage (SAH).
Methods
A total of 61 patients with aneurysmal SAH were included in the study. All patients were amenable for neurological evaluation throughout the critical phase to develop secondary ischemia after SAH. The neurological status was assessed three times a day according to a detailed examination protocol. Mean flow velocities (MFV) in intracranial vessel trunks were measured daily by TCD. Native CT and PCT were routinely acquired at 3-day intervals and, in addition, whenever it was thought to be of diagnostic relevance. The predictive values of abnormal PCT and accelerations in TCD (MFV > 140 cm/s) to detect angiographic DV and DCI within the following 2 days were calculated and compared to the predictive value of delayed ischemic neurological deficits (DIND).
Results
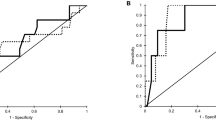
The accuracy of TCD and PCT to predict DV or DCI was 0.65 and 0.63, respectively. In comparison, DIND predicted DV or DCI with an accuracy of 0.96. Pathological PCT findings had a higher sensitivity (0.93) and negative predictive value (0.98) than TCD (0.81 and 0.96).
Conclusion
Neurological assessment at close intervals is the most accurate parameter to detect DV and DCI in the following 3 days. However, DIND may not be reversible. The routine acquisition of PCT in addition to daily TCD examinations seems reasonable, particularly in patients who are not amenable to a detailed neurological examination since it has a higher sensitivity and negative predictive value than TCD and leaves a lower number of undetected cases of vasospasm and infarction.
Similar content being viewed by others


References
Rosengart AJ, Schultheiss KE, Tolentino J, Macdonald RL. Prognostic factors for outcome in patients with aneurysmal subarachnoid hemorrhage. Stroke. 2007;38(8):2315–21.
Dreier JP, Woitzik J, Fabricius M, et al. Delayed ischaemic neurological deficits after subarachnoid haemorrhage are associated with clusters of spreading depolarizations. Brain. 2006;129(Pt 12):3224–37.
Jones TH, Morawetz RB, Crowell RM, et al. Thresholds of focal cerebral ischemia in awake monkeys. J Neurosurg. 1981;54(6):773–82.
Beck J, Raabe A, Lanfermann H, et al. Effects of balloon angioplasty on perfusion- and diffusion-weighted magnetic resonance imaging results and outcome in patients with cerebral vasospasm. J Neurosurg. 2006;105(2):220–7.
Westermaier T, Stetter C, Vince GH, et al. Prophylactic intravenous magnesium sulfate for treatment of aneurysmal subarachnoid hemorrhage: a randomized, placebo-controlled, clinical study. Crit Care Med. 2010;38(5):1284–90.
Kunze E, Pham M, Raslan F, et al. Value of perfusion CT, transcranial doppler sonography, and neurological examination to detect delayed vasospasm after aneurysmal subarachnoid hemorrhage. Radiol Res Pract. 2012;2012:231206. doi:10.1155/2012/231206.
Pham M, Johnson A, Bartsch AJ, et al. CT perfusion predicts secondary cerebral infarction after aneurysmal subarachnoid hemorrhage. Neurology. 2007;69(8):762–5.
Wintermark M, Dillon WP, Smith WS, et al. Visual grading system for vasospasm based on perfusion CT imaging: comparisons with conventional angiography and quantitative perfusion CT. Cerebrovasc Dis. 2008;26(2):163–70.
von Kummer R, Bourquain H, Bastianello S, et al. Early prediction of irreversible brain damage after ischemic stroke at CT. Radiology. 2001;219(1):95–100.
Macdonald RL, Kassell NF, Mayer S, et al. Clazosentan to overcome neurological ischemia and infarction occurring after subarachnoid hemorrhage (CONSCIOUS-1): randomized, double-blind, placebo-controlled phase 2 dose-finding trial. Stroke. 2008;39(11):3015–21.
Ma J, Huang S, Ma L, Liu Y, Li H, You C. Endothelin-receptor antagonists for aneurysmal subarachnoid hemorrhage: an updated meta-analysis of randomized controlled trials. Crit Care. 2012;16(5):R198.
Chaichana KL, Pradilla G, Huang J, Tamargo RJ. Role of inflammation (leukocyte–endothelial cell interactions) in vasospasm after subarachnoid hemorrhage. World Neurosurg. 2010;73(1):22–41.
Zetterling M, Hallberg L, Hillered L, Karlsson T, Enblad P, Ronne EE. Brain energy metabolism in patients with spontaneous subarachnoid hemorrhage and global cerebral edema. Neurosurgery. 2010;66(6):1102–10.
Bosche B, Graf R, Ernestus RI, et al. Recurrent spreading depolarizations after subarachnoid hemorrhage decreases oxygen availability in human cerebral cortex. Ann Neurol. 2010;67(5):607–17.
Stein SC, Levine JM, Nagpal S, LeRoux PD. Vasospasm as the sole cause of cerebral ischemia: how strong is the evidence? Neurosurg Focus. 2006;21(3):2.
Crowley RW, Medel R, Dumont AS, et al. Angiographic vasospasm is strongly correlated with cerebral infarction after subarachnoid hemorrhage. Stroke. 2011;42(4):919–23.
Chaudhary SR, Ko N, Dillon WP, et al. Prospective evaluation of multidetector-row CT angiography for the diagnosis of vasospasm following subarachnoid hemorrhage: a comparison with digital subtraction angiography. Cerebrovasc Dis. 2008;25(1–2):144–50.
Yao GE, Li Q, Jiang XJ, et al. Vasospasm after subarachnoid hemorrhage: a 3D rotational angiography study. Acta Neurochir Suppl. 2011;110(Pt 2):221–5.
Lindegaard KF, Nornes H, Bakke SJ, Sorteberg W, Nakstad P. Cerebral vasospasm after subarachnoid haemorrhage investigated by means of transcranial Doppler ultrasound. Acta Neurochir Suppl (Wien). 1988;42:81–4.
Kassell NF, Sasaki T, Colohan AR, Nazar G. Cerebral vasospasm following aneurysmal subarachnoid hemorrhage. Stroke. 1985;16(4):562–72.
Dorsch NW. Cerebral arterial spasm: a clinical review. Br J Neurosurg. 1995;9(3):403–12.
van den Bergh WM, Algra A, van Kooten F, et al. Magnesium sulfate in aneurysmal subarachnoid hemorrhage: a randomized controlled trial. Stroke. 2005;36(5):1011–5.
Frontera JA, Fernandez A, Schmidt JM, et al. Defining vasospasm after subarachnoid hemorrhage: what is the most clinically relevant definition? Stroke. 2009;40(6):1963–8.
Aralasmak A, Akyuz M, Ozkaynak C, Sindel T, Tuncer R. CT angiography and perfusion imaging in patients with subarachnoid hemorrhage: correlation of vasospasm to perfusion abnormality. Neuroradiology. 2009;51(2):85–93.
Carrera E, Schmidt JM, Oddo M, et al. Transcranial Doppler for predicting delayed cerebral ischemia after subarachnoid hemorrhage. Neurosurgery. 2009;65(2):316–23.
Hickmann AK, Langner S, Kirsch M et al. The value of perfusion computed tomography in predicting clinically relevant vasospasm in patients with aneurysmal subarachnoid hemorrhage. Neurosurg Rev. 2012.
Lee JY, Lee MS, Whang K, Lee JM, Kim SH, Lee SS. Accuracy of transcranial Doppler sonography for predicting cerebral infarction in aneurysmal subarachnoid hemorrhage. J Clin Ultrasound. 2006;34(8):380–4.
Conflict of interest
Thomas Westermaier received lecture fees from Johnson & Johnson. All other authors have no personal, financial, institutional or academic conflict of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Westermaier, T., Pham, M., Stetter, C. et al. Value of Transcranial Doppler, Perfusion-CT and Neurological Evaluation to Forecast Secondary Ischemia after Aneurysmal SAH. Neurocrit Care 20, 406–412 (2014). https://doi.org/10.1007/s12028-013-9896-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-013-9896-0