
Abstract
Background
Sustained severe hyperthermia in patients with high cervical spinal cord injuries may have many etiologies, from infection to autonomic dysregulation. When uncontrolled, it has been seen to have a high morbidity and mortality.
Methods
We present two patients with high cervical spinal cord injury (SCI) who had sustained severe hyperpyrexia, of possible autonomic origin. The temperature stayed above 40°C and was uncontrolled with conventional methods of temperature management.
Results
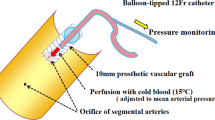
We employed endovascular cooling for therapeutic normothermia which was successful in effective control of temperature in both the patients. The first patient suffered complications from deep vein thrombosis and pulmonary embolism which may be attributed to the presence of the cooling catheter in spite of chemical and mechanical thromboprophylaxis.
Conclusions
The use of endovascular cooling in the management of severe life threatening hyperthermia in patients with cervical SCI may be an useful intervention. There must be a high suspicion for the possibility of deep vein thrombosis in this subgroup, however.


Similar content being viewed by others


References
Mc Kinley W, McNamee S, Meade M, Kandra K, et al. Incidence, etiology, and risk factors for fever following acute spinal cord injury. J Spinal Cord Med. 2006;29:501–6.
Ulger F, Dilek A, Karakaya D, Senel A, et al. Fatal fever of unknown origin in acute cervical spinal cord injury: five cases. J Spinal Cord Med. 2009;32:343–8.
Scott SR, Matthew MJ, Philip MS, William LB, et al. Fatal malignant hyperpyrexia in a cervical spine-injured patient. J Trauma. 2005;58:375–7.
Broessner G, Beer R, Franz G, Lackner P, et al. Severe heat stroke with multiple organ dysfunction—a novel intravascular treatment approach. Crit Care. 2005;9:R498–501.
Polderman KH, Herold I. Therapeutic hypothermia and controlled normothermia in the intensive care unit: practical considerations, side effects, and cooling methods. Crit Care Med. 2009;37:1101–20.
Sugarman B. Fever in recently injured quadriplegic persons. Arch Phys Med Rehabil. 1982;63(12):639–40.
Gaffin SL, Hubbard RW Pathophysiology of heat stroke. In: Pandoff KB, Burr RE (eds) U.S. army textbook of military medicine (TMM): medical aspects of harsh environments. Office of the Surgeon General, Department of the Army.
Marion DW. Controlled normothermia in neurologic intensive care. Crit Care Med. 2004;32:S43–51.
Levi AD, Casella G, Green BA, et al. Clinical outcomes using modest intravascular hypothermia after acute cervical spinal cord injury. Neurosurgery. 2010;66:670–7.
Simosa HF, Petersen DJ, Agarwal SK, et al. Increased risk of deep venous thrombosis with endovascular cooling in patients with traumatic head injury. Am Surg. 2007;73:461–4.
Acknowledgments
The authors acknowledge Ms Helen Jones, senior nurse, Horsley Intensive care unit for her valuable input into the idea and material of the manuscript and Mr Martin Wilby, consultant neurosurgeon.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tripathy, S., Whitehead, C.F. Endovascular Cooling for Severe Hyperthermia in Cervical Spine Injury. Neurocrit Care 15, 525–528 (2011). https://doi.org/10.1007/s12028-011-9529-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-011-9529-4