
Abstract
Background
Studies devoted to intensive glucose control suggested that the intensive insulin therapy (IIT) approach could effectively reduce complications associated with critical illness. A program of IIT with the goal of achieving a blood glucose of 80–120 mg/dL was, therefore, adopted in this study. To explore the impact of this approach in patients admitted to a neurocritical care unit, we compared the short-term outcomes of patients treated before and after our policy change.
Methods
Retrospectively extracted data from the electronic medical records of 1913 patients admitted between Feb 1, 2005 and Aug 30, 2006 were included in the standard insulin therapy group (SIT targeted to maintain blood glucose levels less than 150 mg/dL) and 1796 patients admitted between Sept 1, 2006 and March 30, 2008 were included in the IIT group (IIT-targeted to maintain blood glucose levels between 80 and 120 mg/dL).
Results
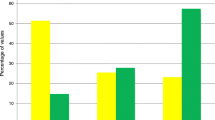
Mean glucose levels were lower in the IIT compared to SIT (136.9 mg/dL, SD 47.6 vs. 143.8 mg/dL, SD 46.4); however, this strategy was also associated with an increased incidence of hypoglycemia (OR: 1.8, and 95% CI: 1.5–2.3). The likelihood of mortality increased proportionally as the severity of hypoglycemia worsened (any blood glucose value <70 mg/dL, OR: 3.26, and 95% CI: 2.52–4.22, any blood glucose <40, OR: 3.65, and 95% CI: 2.21–6.02, any blood glucose <20, OR: 6.25, and 95% CI: 2.41–16.23).
Conclusion
IIT was not only able to reduce overall mean glucose levels, but also resulted in significantly more episodes of hypoglycemia, increased mortality, and increased length of stay. The relationship between hypoglycemia and mortality indicates that efforts to control glucose levels should also aggressively avoid induction of hypoglycemia.

Similar content being viewed by others
References
Van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, Vlasselaers D, Ferdinande P, Lauwers P, Bouillon R. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345(19):1359–67.
Van den Berghe G, Wilmer A, Hermans G, Meersseman W, Wouters PJ, Milants I, Van Wijngaerden E, Bobbaers H, Bouillon R. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006;354(5):449–61.
Krinsley JS. Effect of an intensive glucose management protocol on the mortality of critically ill adult patients. Mayo Clin Proc. 2004;79(8):992–1000.
Bilotta F, Caramia R, Paoloni FP, Delfini R, Rosa G. Safety and efficacy of intensive insulin therapy in critical neurosurgical patients. Anesthesiology. 2009;110(3):611–9.
Krinsley JS. Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically ill patients. Mayo Clin Proc. 2003;78(12):1471–8.
Finfer S, Chittock DR, Su SY, Blair D, Foster D, Dhingra V, Bellomo R, Cook D, Dodek P, Henderson WR, et al. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283–97.
Oz G, Seaquist ER, Kumar A, Criego AB, Benedict LE, Rao JP, Henry PG, Van De Moortele PF, Gruetter R. Human brain glycogen content and metabolism: implications on its role in brain energy metabolism. Am J Physiol. 2007;292(3):E946–51.
Rao J, Oz G, Seaquist ER. Regulation of cerebral glucose metabolism. Minerva endocrinologica. 2006;31(2):149–58.
Ouyang YB, He QP, Li PA, Janelidze S, Wang GX, Siesjo BK. Is neuronal injury caused by hypoglycemic coma of the necrotic or apoptotic type? Neurochem Res. 2000;25(5):661–7.
Dorhout Mees SM, van Dijk GW, Algra A, Kempink DR, Rinkel GJ. Glucose levels and outcome after subarachnoid hemorrhage. Neurology. 2003;61(8):1132–3.
Schlenk F, Sarrafzadeh AS. Is continuous insulin treatment safe in aneurysmal subarachnoid hemorrhage? Vasc Health Risk Manag. 2008;4(4):885–91.
Ho CL, Ang CB, Lee KK, Ng IH. Effects of glycaemic control on cerebral neurochemistry in primary intracerebral haemorrhage. J Clin Neurosci. 2008;15(4):428–33.
Vespa P, Boonyaputthikul R, McArthur D, Miller C, Etchepare M, Bergsneider M, Glenn T, Martin N, Hovda D. Intensive insulin therapy reduces microdialysis glucose values without altering glucose utilization or improving the lactate/pyruvate ratio after traumatic brain injury. Crit Care Medicine. 2006;34(3):850–6.
Oksanen T, Skrifvars M, Varpula T, Kuitunen A, Pettila V, Nurmi J, Castren M. Strict versus moderate glucose control after resuscitation from ventricular fibrilation. Intensive Care Med. 2007;33:2093–100.
Falciglia M, Freyberg R, Almenoff P, D’Alessio D, Render M. Hyperglycemia-related mortality in critically ill patients varies with admission diagnosis. Crit Care Med. 2009;37:3001–9.
Griesdale D, Tremblay B-H, McEwen J, Chittock D. Glucose control and mortality in patients with severe traumatic brain injury. Neurocrit Care. 2009;11:311–6.
Curkendall SM, Natoli JL, Alexander CM, Nathanson BH, Haidar T, Dubois RW. Inpatient diabetic hypoglycemia: economic and clinical impact. Endocr Pract. 2009;6:1–48.
Kreutziger J, Wenzel V, Kurz A, Constantinescu MA. Admission blood glucose is an independent predictive factor for hospital mortality in polytraumatised patients. Intensive Care Med. 2009;35(7):1234–9.
Salim A, Hadjizacharia P, Dubose J, Brown C, Inaba K, Chan LS, Margulies D. Persistent hyperglycemia in severe traumatic brain injury: an independent predictor of outcome. Am Surg. 2009;75(1):25–9.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Graffagnino, C., Gurram, A.R., Kolls, B. et al. Intensive Insulin Therapy in the Neurocritical Care Setting is Associated with Poor Clinical Outcomes. Neurocrit Care 13, 307–312 (2010). https://doi.org/10.1007/s12028-010-9469-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-010-9469-4