
Abstract
Background
Laparoscopic sleeve gastrectomy (LSG) has become the preferred bariatric procedure in many countries. However, there is one shortcoming of LSG in the long-term follow-up and this is the onset of GERD and erosive esophagitis (EE). Current evidence of the effect of SG on GERD did not consolidate to a consensus. In this study, we objectively evaluate the incidence of EE 1 year post-LSG with upper endoscopy (EGD) and try to identify the significant variables and possible underlying mechanisms of the EE post-LSG.
Methods
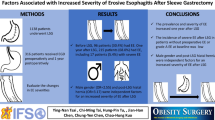
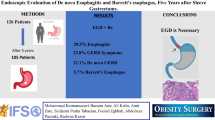
Over a period of 5 years (2011–2016) at Singapore General Hospital, we retrospectively reviewed a prospectively collected database of a cohort of patients whom had LSG by a single surgeon who routinely performed EGD pre-operative and 1 year post-operative to assess EE and hiatal hernia. Patient’s endoscopic findings and demographic and anthropometric data were analyzed.
Results
We identified a total of 97 obese patients who underwent LSG at our hospital by studied surgeon. Sixty-three patients (64.9% of original sample) were finally evaluated in the present study, 40 (59.7%) of whom were female. The mean (range) age of patients was 38.2 (18–66) years, and mean BMI was 36.3 ± 4.1 kg/m2. Median time to follow-up EGD was 13 months (range, 12–15). Following LSG, there was a significant decrease in both BMI (42.1 ± 1.2 vs. 29.9 ± 1.0 kg/m2) and percentage excess weight loss of 56.6 ± 3.6%. The prevalence of EE on endoscopy increased from 9 (14.3%) to 28 (44.4%) patients. Of which 15 (23.8%) were grade A, 11 (17.5%) were grade B, and 2 (3.2%) were grade C. There was no correlation between GERD symptoms with EE; however, our study found a trend suggesting higher prevalence of EE with a sleeve diameter measuring > 2 cm wide (p = 0.069).
Conclusion
Although LSG is effective in treating obesity and its metabolic syndromes, the prevalence of EE increased significantly 1 year after the surgery. Since we do not fully understand the long-term impact of chronic esophagitis in post-sleeve population, we recommend follow-up EGD assessment post-operatively and treat the esophagitis if present.





Similar content being viewed by others

References
WHO Media Centre: Obesity and overweight. Available at: http://www.who.int/mediacentre/factsheets/fs311/en/index.html 2014. Accessed March, 2017
National Institutes of Health (NIH), National Heart, Lung, and Blood Institute (NHLBI) clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. Washington, DC: U.S. DHHS, Public Health Service (PHS) 1998
Allison DB, Fontaine KR, Manson JEet al. VanItallie TB Annual deaths attributable to obesity in the United States. JAMA 1999;282:1530–1538
Schauer PR, Kashyap SR, Wolski K, et al. Bariatric surgery versus intensive medical therapy in obese patients with diabetes. N Engl J Med. 2012;366(17):1567–76.
Angrisani L, Santonicola A, Iovino P, et al. Bariatric surgery and endoluminal procedures: IFSO worldwide survey 2014. Obes Surg. 2017;27(9):2279–89.
Jossart GH, Anthone G, et al. The history of sleeve gastrectomy. Bariatric Times. 2010;7:9–10.
Hess DS, Hess DW. Biliopancreatic diversion with a duodenal switch. Obes Surg. 1998;8:267–82.
Marceau P, Biron Simon, St Georges R, at al. Biliopancreatic diversion with gastrectomy as surgical treatment of morbid obesity. Obes Surg 1991;1:381–387
Kim WW, Gagner M, Kini S, et al. Laparoscopic vs. open biliopancreatic diversion with a duodenal switch: a comparative study. J Gastrointest Surg. 2003;7:552–7.
Daes J, Jimenez ME, Said N, et al. Laparoscopic sleeve gastrectomy: symptoms of gastroesophageal reflux can be reduced by changes in surgical technique. Obes Surg. 2012;22(12):1874–9.
Chiu S, Birch DW, Shi X. Effect of sleeve gastrectomy on gastroesophageal reflux disease: a systematic review. Surg Obes Relat Dis. 2011;7:510–5.
Lundell LR, Dent J, Bennett JR, et al. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification. GUT. 1999;45:172–80.
Himpens J, Dapri G, Cadiere GB. A prospective randomized study between laparoscopic gastric banding and laparoscopic isolated sleeve gastrectomy: results after 1 and 3 years. Obes Surg. 2006;16:1450–6.
Braghetto I, Csendes A, Korn O, et al. Gastroesophageal reflux disease after sleeve gastrectomy. Surg Laparosc Endosc Percutan Tech. 2010;20:148–53.
Lakdawala MA, Bhasker A, Mulchandani D, et al. Comparison between the results of laparoscopic sleeve gastrectomy and laparoscopic Roux-en-Y gastric bypass in the Indian population: a retrospective 1 year study. Obes Surg. 2010;20:1–6.
Carter PR, LeBlanc KA, Hausmann MG, et al. Association between gastroesophageal reflux disease and laparoscopic sleeve gastrectomy. Surg Obes Relat Dis. 2011;7:569–72.
Howard DD, Caban AM, Cendan JC, et al. Gastroesophageal reflux after sleeve gastrectomy in morbidly obese patients. Surg Obes Relat Dis. 2011;7:709–13.
Tai CM, Huang CK, Lee YC, et al. Increase in gastroesophageal reflux disease symptoms and erosive esophagitis 1 year after laparoscopic sleeve gastrectomy among obese adults. Surg Endosc. 2013;27:1260–6.
Genco A, Soricelli E, Casella G, et al. Gastroesophageal reflux disease and Barrett’s esophagus after laparoscopic sleeve gastrectomy: a possible, underestimated long-term complication. Surg Obes Relat Dis. 2017;13(4):568–74.
Shaheen NJ, Richter JE. Barrett’s oesophagus. Lancet 2009;7:373:850–861
Frederik HJ, Lars P, Asbjorn MD, et al. Incidence of adenocarcionoma among patients with Barrett’s esophagus. NEJM. 2011;365:1375–83.
Braghetto I, Csendes A. Prevalence of Barrett’s esophagus in bariatric patients undergoing sleeve gastrectomy. Obes Surg. 2016;26(4):710–4.
Mion F, Tolone S, Garros A, et al. High-resolution impedance manometry after sleeve gastrectomy: increased intragastric pressure and reflux are frequent events. Obes Surg. 2016;26(10):2449–56.
Burgerhart JS, van Rutte PWJ, Edelbroek MAK, et al. Association between postprandial symptoms and gastric emptying after sleeve gastrectomy. Obes Surg. 2015;25:209–14.
Melissas J, Leventi A, Klinaki I, et al. Alterations of global gastrointestinal motility after sleeve gastrectomy. Ann Surg. 2013;258:976–82.
Michalsky D, Dvorak P, Belacek J, et al. Radical resection of the pyloric antrum and its effect on gastric emptying after sleeve gastrectomy. Obes Surg. 2013;23:567–73.
Shah S, Shah P, Todkar J, et al. Prospective controlled study of effect of laparoscopic sleeve gastrectomy on small bowel transit time and gastric emptying half-time in morbidly obese patients with type 2 diabetes mellitus. Surg Obes Relat Dis. 2010;6:152–7.
Braghetto I, Davanzo C, Korn O, et al. Scintigraphic evaluation of gastric emptying in obese patients submitted to sleeve gastrectomy compared to normal subjects. Obes Surg. 2009;19:1515–21.
Bernstine H, Tzioni-Yehoshua R, Groshar D, et al. Gastric emptying is not affected by sleeve gastrectomy—scintigraphic evaluation of gastric emptying after sleeve gastrectomy without removal of the gastric antrum. Obes Surg. 2009;19:293–8.
Melissas J, Koukouraki S, Askoxylakis J, et al. Sleeve gastrectomy–a restrictive procedure? Obes Surg. 2007;17:57–62.
Melissas J, Daskalakis M, Koukouraki S, et al. Sleeve gastrectomy—a “food limiting” operation. Obes Surg. 2008;18:1251–6.
Samuel B, Atiemo K, Cohen P, et al. The effect of sleeve gastrectomy on gastroparesis: a short clinical review. Bariatric Surg Pract Patient Care. 2016;11:84–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest Statement
Author 1, author 2, author 3, author 4, author 5, author 6, author 7 & author 8 have nothing to disclose.
Ethics Approval Statement
For this type of retrospective study, formal consent is not required.
Rights and permissions
About this article

Cite this article
Lim, C.H., Lee, P.C., Lim, E. et al. Correlation Between Symptomatic Gastro-Esophageal Reflux Disease (GERD) and Erosive Esophagitis (EE) Post-vertical Sleeve Gastrectomy (VSG). OBES SURG 29, 207–214 (2019). https://doi.org/10.1007/s11695-018-3509-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-018-3509-0