
Abstract
Background
Morbid obesity may be associated with malnutrition. Because it is important to assess the preoperative nutritional/metabolic status and bone mineral density of these patients, this study was designed aiming to evaluate bone metabolism/mineral density and nutritional profile in morbidly obese women.
Methods
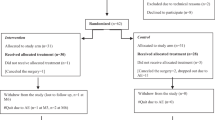
Thirty-three morbidly obese women in preoperative care for obesity surgery were enrolled. Blood samples were drawn to determine nutritional and metabolic status, and dual-energy X-ray absorptiometry (DXA) was performed to evaluate bone mineral density; 24-h recall and food frequency questionnaire (FFQ) were also evaluated.
Results
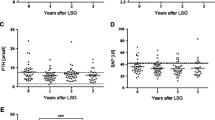
Twenty-seven (81.8%) women were premenopausal and six (18.2%) were postmenopausal. The mean body mass index was 43.2 ± 4.8 kg/m2, and 91% were Caucasian. Insulin-resistant subjects comprised 81.8% of the sample. The median (25–75 percentile) of the total intake of 24-h recall was 3,081 (2,718–3,737) and for FFQ 2,685 (2,284–4,400) calories. FFQ underestimated total energy value intake. The median of calcium was higher when evaluated by the FFQ as compared with the 24-h recall. Protein and lipid intakes were lower if evaluated by the FFQ as compared to the 24-h recall. Vitamin D levels were low in 18 (81.8%) patients. In one premenopausal woman, bone mineral density was low in the lumbar spine (L1–L4), and in one postmenopausal woman it was low in L1–L4, femoral neck and 1/3 proximal radius.
Conclusions
In this study, the nutritional status of morbidly obese women was good, except for markers of bone metabolism, with no detectable differences between pre- and postmenopausal women.
Similar content being viewed by others

References
Rosen C, Klibanski A. Bone, fat, and body composition: evolving concepts in the pathogenesis of osteoporosis. Am J Med. 2009;122:409–14.
Langlois JA, Mussolino ME, Visser M, et al. Weight loss from maximum body weight among middle-aged and older white women and the risk of hip fracture: the NHANES I epidemiologic follow-up study. Osteoporosis Int. 2001;12:763–8.
Coates PS, Fernstrom JD, Fernstrom MH, et al. Gastric bypass surgery for morbid obesity leads to an increase in bone turnover and a decrease in bone mass. J Clin Endocrinol Metab. 2004;89:1061–5.
Bano G, Rodin DA, Pazianas M, et al. Reduced bone mineral density after surgical treatment for obesity. Int J Obes Relat Metab Disord. 1999;23:361–5.
Sjöström L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683–93.
Sjöström L, Narbro K, Sjöström CD, et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357:741–52.
Colossi FG, Casagrande DS, Chatkin R, et al. Need for multivitamin use in the postoperative period of gastric bypass. Obes Surg. 2008;17:1150–8.
Fleischer J, Stein EM, Bessler M, et al. The decline in hip bone density following gastric bypass surgery is associated with extent of weight loss. J Clin Endocrinol Metab. 2008;93:3735–40.
Hamoui N, Kim K, Anthone G, et al. The significance of elevated levels of parathyroid hormone in patients with morbid obesity before and after bariatric surgery. Arch Surg. 2003;138:891–7.
Carlin AM, Rao DS, Meslemani AM, et al. Prevalence of vitamin D depletion among morbidly obese patients seeking gastric bypass surgery. Surg Obes Relat Dis. 2006;2:98–103.
Goldner WS, Stoner JA, Thompson J, et al. Prevalence of vitamin D insufficiency and deficiency in morbidly obese patients: a comparison with non-obese controls. Obes Surg. 2008;18:145–50.
Lacativa PG, Farias MLF. Office practice of osteoporosis evaluation. Arq Bras Endocrinol Metab. 2006;50:674–84.
Miller PD, Zapalowski C, Kulak CAM, et al. Bone densitometry: the best way to detect osteoporosis and to monitor therapy. J Clin Endocrinol Metab. 1999;84:1867–71.
El-Kadre LJ, Rocha PR, Tinoco ACA, et al. Calcium metabolism in pre- and postmenopausal morbidly obese women at baseline and after laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2004;14:1062–6.
Sichieri R. Epidemiologia da Obesidade. Rio de Janeiro. EDUERJ 1998.
Souza RAG, Rangel ACS, Rogério CM, et al. Confiabilidade de um questionário de consumo alimentar em mulheres. Cienc Cuid Saúde. 2007;6:103–9.
Carroll Rj, Pee D, Freedman LS, et al. Statistical design of calibration studies. Am J Clin Nutr. 1997;65:1187S–9S.
Jain MG, Rohan TE, et al. Calibration of the dietary questionnaire for the Canadian study of diet, lifestyle and health cohort. Public Health Nutr. 2003;6:79–86.
Ashraf A, Alvarez J, Saenz K, et al. Threshold for effects of vitamin D deficiency on glucose metabolism in obese female African American adolescents. J Clin Endocrinol Metab. 2009;94:3200–6.
Nishizawa Y, Nakamura T, Ohta H, et al. Guidelines for the use of biochemical markers of bone turnover in osteoporosis (2004). J Bone Metab. 2005;23:97–104.
Lam GS, Asplin JR, Halperin ML. Does a high concentration of calcium in the urine cause an important renal concentrating defect in human subjects? Clin Sci (Lond). 2000;98:313–9.
Hamoui N, Anthone G, Crookes PF. Calcium metabolism in the morbidly obese. Obes Surg. 2004;14:9–12.
Lee JH, O’Keefe JH, Bell D, et al. Vitamin D deficiency: an important, common, and easily treatable cardiovascular risk factor? J Am Coll Cardiol. 2008;52:1949–56.
Brandão CMA, Camargos BM, Zerbini CA, et al. 2008 official positions of the Brazilian society for clinical densitometry—SBDens. Arq Bras Endocrinol Metab. 2009;53:107–12.
Geloneze B, Vasques ACJ, Stabe CFC, et al. HOMA1-IR and HOMA2-IR indexes in identifying insulin resistance and metabolic syndrome—Brazilian Metabolic Syndrome Study (BRAMS). Arq Bras Endocrinol Metab. 2009;53:281–7.
US NATIONAL ACADEMY OF SCIENCES (USA). Dietary Reference Intakes for vitamin C, vitamin E, selenium and carotenoids. Washington DC : National Academy Press, 2000, 506p. (A report on the antioxidants and related compounds. Subcommittees on Upper Reference Intake Levels of Nutrients and Interpretation of Uses of Dietary Reference Intakes and the Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Food and Nutrition Board).
Krebs-Smith SM, Graubard BI, Kahle LL, et al. Low energy reporters vs others: a comparison of reported food intakes. Eur J Clin Nutr. 2000;54:281–7.
Johansson G, Wikman A, Ahrén AM, et al. Underreporting of energy intake in repeated 24-hour recalls related to gender, age, weight status, day of interview, educational level, reported food intake, smoking habits and area of living. Public Health Nutr. 2001;4:919–27.
Hernández-Avila M, Romieu I, Parra S, et al. Validity and reproducibility of a food frequency questionnaire to assess dietary intake of women living in Mexico City. Salud Publica Mex. 1998;40:133–40.
Allard J. Should nutritional status be routinely assessed and corrected before bariatric surgery? Nat Clin Pract Gastroenterol Hepatol. 2007;4:130–1.
Ernst B, Thurnheer M, Schmid SM, et al. Evidence for the necessity to systematically assess micronutrient status prior to bariatric surgery. Obes Surg. 2009;19:66–73.
Flancbaum L, Belsley S, Drake V, et al. Preoperative nutritional status of patients undergoing Roux-en-Y Gastric Bypass for morbid obesity. J Gastrointest Surg. 2006;10:1033–7.
Gemmel K, Santry HP, Prachand VN, et al. Vitamin D deficiency in preoperative bariatric surgery patients. Surg Obes Relat Dis. 2009;5:54–9.
Aasheim ET, Hofsø D, Hjelmesaeth J, et al. Vitamin status in morbidly obese patients: a cross-sectional study. Am J Clin Nutr. 2008;87:362–9.
Wang TJ, Pencina MJ, Booth SL, et al. Vitamin D deficiency and risk of cardiovascular disease. Circulation. 2008;117:503–11.
Hagström E, Hellman P, Larsson TE, et al. Plasma parathyroid hormone and the risk of cardiovascular mortality in the community. Circulation. 2009;119:2765–71.
Silva BC, Camargos BM, Fujii JB, et al. Prevalence of vitamin D deficiency and its correlation with iPTH, biochemical bone turnover markers and bone mineral density, among patients from ambulatories. Arq Bras Endocrinol Metab. 2008;52:482–8.
Avgerimos DV, Leitman MI, Martinez RE, et al. Evaluation of markers for calcium homeostasis in a population of obese adults undergoing gastric bypass operations. J Am Coll Surg. 2007;205:294–7.
Eastell R, Mallinak N, Weiss S, et al. Biological variability of serum and urinary N-Telopeptides of Type I collagen in postmenopausal women. J Bone Miner Res. 2000;15:594–8.
Nakamura K, Saito T, Yoshihara A, et al. Low calcium intake is associated with increased bone reabsorption in postmenopausal Japanese women: Yokogoshi Study. Public Health Nutr. 2009;12:1–5.
Barrett-Connor E, Kritz-Silverstein D. Does hiperinsulinemia preserve bone? Diabetes Care. 1996;19:1388–92.
Gómez JM, Vilarrasa N, Masdevall C, et al. Regulation of bone mineral density in morbidly obese women: a cross-sectional study in two cohorts before and after bypass surgery. Obes Surg. 2009; 19:345–50.
Bacon L, Stern JS, Keim NL, et al. Low bone mass in premenopausal chronic dieting obese women. Eur J Clin Nutr. 2004;58:966–71.
Institute of Medicine, Food and Nutrition Board. Dietary reference intakes (DRIs): recommended intakes for individuals, Vitamins. Washington: National Academy Press; 2001.
Institute of Medicine, Food and Nutrition Board. Dietary reference intakes (DRIs): recommended intakes for individuals, Elements. Washington: National Academic Press; 2001.
Baca EA, Ulibarri VA, Scariano JK, et al. Increased serum levels of N-telopeptides (NTx) of bone collagen in postmenopausal Nigerian women. Calcif Tissue Int. 1999;65:125–8.
Disclosure
There are no external sources of funds supporting this work. There is no financial interest for any of the authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Casagrande, D.S., Repetto, G., Mottin, C.C. et al. Bone Mineral Density and Nutritional Profile in Morbidly Obese Women. OBES SURG 20, 1372–1379 (2010). https://doi.org/10.1007/s11695-010-0121-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-010-0121-3