
ABSTRACT
BACKGROUND
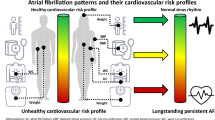
After an initial episode of atrial fibrillation (AF), AF may recur and become permanent. AF progression is associated with higher morbidity and mortality. Understanding the risk factors for permanent AF could help identify people who would benefit most from interventions.
OBJECTIVE
To determine whether body mass index (BMI), diabetes, hypertension, and blood pressure levels are associated with permanent AF among people whose initial AF episode terminated.
DESIGN
Population-based inception cohort study.
PARTICIPANTS
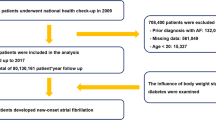
Enrollees in Group Health, an integrated health care system, aged 30–84 with newly diagnosed AF in 2001–2004, whose initial AF terminated within 6 months and who had at least 6 months of subsequent follow-up (N = 1,385).
MAIN MEASURES
Clinical characteristics were determined from medical records. Permanent AF was determined from medical records and ECG and administrative databases. Permanent AF was defined as AF present on two separate occasions 6–36 months apart, without any documented sinus rhythm between the two occasions. Cox proportional hazards models were used to estimate adjusted hazard ratios (HRs).
KEY RESULTS
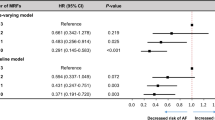
Five-year cumulative incidence of permanent AF was 24 %. Compared with normal BMI (18.5–24.9 kg/m2), BMI levels of 25.0–29.9 (overweight), 30.0–34.9 (obese 1), 35.0–39.9 (obese 2), and ≥ 40.0 kg/m2 (obese 3) were associated with HRs of permanent AF of 1.26 (95 % CI: 0.92, 1.72); 1.35 (0.96, 1.91); 1.50 (0.97, 2.33); and 1.79 (1.13, 2.84), adjusted for age, sex, diabetes, hypertension, blood pressure, coronary heart disease, valvular heart disease, heart failure, and prior stroke. Diabetes, hypertension, and blood pressure were not associated with permanent AF.
CONCLUSIONS
For people whose initial AF episode terminates, benefits of having lower BMI may include a lower risk of permanent AF. Risk of permanent AF was similar for people with and without diabetes or hypertension and across blood pressure levels.
Similar content being viewed by others
REFERENCES
Fuster V, Ryden LE, Cannom DS, et al. ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2006;114:e257–354.
Kerr CR, Humphries KH, Talajic M, et al. Progression to chronic atrial fibrillation after the initial diagnosis of paroxysmal atrial fibrillation: results from the Canadian Registry of Atrial Fibrillation. Am Heart J. 2005;149:489–96.
de Vos CB, Pisters R, Nieuwlaat R, et al. Progression from paroxysmal to persistent atrial fibrillation: clinical correlates and prognosis. J Am Coll Cardiol. 2010;55:725–31.
Steg PG, Alam S, Chaing CE, et al. Symptoms, functional status and quality of life in patients with controlled and uncontrolled atrial fibrillation: data from the RealiseAF cross-sectional international registry. Heart. 2012;98:195–201.
Patton KK, Page RL. New-onset paroxysmal atrial fibrillation: is permanence inevitable? Am Heart J. 2005;149:388–90.
Dublin S, French B, Glazer NL, et al. Risk of new-onset atrial fibrillation in relation to body mass index. Arch Intern Med. 2006;166:2322–8.
Dublin S, Glazer NL, Smith NL, et al. Diabetes mellitus, glycemic control, and risk of atrial fibrillation. J Gen Intern Med. 2010;25:853–8.
Thomas MC, Dublin S, Kaplan RC, et al. Blood pressure control and risk of incident atrial fibrillation. Am J Hypertens. 2008;21:1111–6.
Tsang TS, Barnes ME, Miyasaka Y, et al. Obesity as a risk factor for the progression of paroxysmal to permanent atrial fibrillation: a longitudinal cohort study of 21 years. Eur Heart J. 2008;29:2227–33.
Heckbert SR, Wiggins KL, Glazer NL, et al. Antihypertensive treatment with ACE inhibitors or beta-blockers and risk of incident atrial fibrillation in a general hypertensive population. Am J Hypertens. 2009;22:538–44.
Glazer NL, Dublin S, Smith NL, et al. Newly detected atrial fibrillation and compliance with antithrombotic guidelines. Arch Intern Med. 2007;167:246–52.
Arterburn D, Ichikawa L, Ludman EJ, et al. Validity of clinical body weight measures as substitutes for missing data in a randomized trial. Obes Res Clin Pract. 2008;2:277–81.
Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure probabilities in the presence of competing risks: new representations of old estimators. Stat Med. 1999;18:695–706.
Coviello V, Boggess M. Cumulative incidence estimation in the presence of competing risks. Stata J. 2004;4:103–12.
Prentice RL, Kalbfleisch JD, Peterson AV Jr, Flournoy N, Farewell VT, Breslow NE. The analysis of failure times in the presence of competing risks. Biometrics. 1978;34:541–54.
Zhang X, Zhang S, Li Y, et al. Association of obesity and atrial fibrillation among middle-aged and elderly Chinese. Int J Obes. 2009;33:1318–25.
Guglin M, Maradia K, Chen R, Curtis AB. Relation of obesity to recurrence rate and burden of atrial fibrillation. Am J Cardiol. 2011;107:579–82.
Kistler PM, Sanders P, Morton JB, Vohra JK, Kalman JM, Sparks PB. Effect of body mass index on defibrillation thresholds for internal cardioversion in patients with atrial fibrillation. Am J Cardiol. 2004;94:370–2.
Freynhofer MK, Jarai R, Hochtl T, et al. Predictive value of plasma Nt-proBNP and body mass index for recurrence of atrial fibrillation after cardioversion. Int J Cardiol. 2011;149:257–9.
Cha Y-M, Friedman PA, Asirvatham SJ, et al. Catheter ablation for atrial fibrillation in patients with obesity. Circulation. 2008;117:2583–90.
Chilukuri K, Dalal D, Gadrey S, et al. A prospective study evaluating the role of obesity and obstructive sleep apnea for outcomes after catheter ablation of atrial fibrillation. J Cardiovasc Electrophysiol. 2010;21:521–5.
Jongnarangsin K, Chugh A, Good E, et al. Body mass index, obstructive sleep apnea, and outcomes of catheter ablation of atrial fibrillation. J Cardiovasc Electrophysiol. 2008;19:668–72.
Needleman M, Calkins H. The role of obesity and sleep apnea in atrial fibrillation. Curr Opin Cardiol. 2011;26:40–5.
Wanahita N, Messerli FH, Bangalore S, Gami AS, Somers VK, Steinberg JS. Atrial fibrillation and obesity—results of a meta-analysis. Am Heart J. 2008;155:310–5.
Badheka AO, Rathod A, Kizilbash MA, et al. Influence of obesity on outcomes in atrial fibrillation: yet another obesity paradox. Am J Med. 2010;123:646–51.
Ardestani A, Hoffman HJ, Cooper HA. Obesity and outcomes among patients with established atrial fibrillation. Am J Cardiol. 2010;106:369–73.
Acknowledgements
We thank the study participants, Group Health Research Institute staff, and UW Cardiovascular Health Research Unit staff.
This research was supported by NHLBI grant R01 HL068986 (PI: Heckbert), NHLBI training grant T32 HL007902 (PI: Siscovick; Trainee: Thacker), and NIA grant K23 AG028954 (PI: Dublin).
A preliminary version of this research was presented at the American Heart Association 51st Cardiovascular Disease Epidemiology and Prevention Conference, Atlanta, GA, March 2011.
Conflict of Interest
Dr. Dublin has received a Merck/American Geriatrics Society New Investigator Award. Dr. Psaty is a member of the Data and Safety Monitoring Board (DSMB) for a trial of a device funded by the manufacturer and a member of the steering committee for the Yale Open Data Access Project funded by Medtronic. The other authors declare that they do not have any conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(PDF 132 kb)
Rights and permissions
About this article
Cite this article
Thacker, E.L., McKnight, B., Psaty, B.M. et al. Association of Body Mass Index, Diabetes, Hypertension, and Blood Pressure Levels with Risk of Permanent Atrial Fibrillation. J GEN INTERN MED 28, 247–253 (2013). https://doi.org/10.1007/s11606-012-2220-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-012-2220-4