
Abstract
Purpose
The authors sought to evaluate whether the reacquisition of images 3 h after administration of radiotracer improves the sensitivity of fluorine-18 fluorodeoxyglucose positron emission tomography computed tomography ([18F]-FDG PET/CT) in patients with suspicious breast lesions.
Materials and methods
Forty-eight patients with 59 breast lesions underwent an [18F]-FDG PET/CT study in the prone position with a dual-time-point acquisition performed in the early phase 1 h after FDG administration (PET-1) and in the delayed phase 3 h after FDG administration (PET-2). Both examinations were evaluated qualitatively and semiquantitatively with calculation of the mean percentage variation of the standard uptake values (Δ% SUVmax) between PET-1 and PET-2. All lesions with an SUVmax ≥2.5 at PET-1 or a reduction in SUV between PET-1 and PET-2 were considered benign. The definitive histopathological diagnosis was available for all patients included in the study.
Results
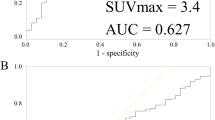
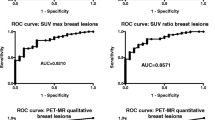
The dual-time-point acquisition of [18F]-FDG PET/CT displayed an accuracy of 85% for lesions with an SUVmax ≥2.5 and/or positive Δ% SUVmax, with sensitivity and specificity values of 81% and 100% compared with 69%, 63% (both p<0.001) and 100% (p=n.s.), respectively, for the single-time-point acquisition. Malignant lesions showed an increase in FDG uptake between PET-1 and PET-2, with a Δ% SUVmax of 10±7 (p<0.04). In contrast, benign lesions showed a decrease in SUV between PET-1 and PET-2, with aΔ% SUVmax of −21±7 (p<0.001).
Conclusions
The delayed repeat acquisition of PET images improves the accuracy of [18F]-FDG PET/CT in patients with suspicious breast lesions with respect to the single-time-point acquisition. In addition, malignant breast lesions displayed an increase in FDG uptake over time, whereas benign lesions showed a reduction. These variations in FDG uptake between PET-1 and PET-2 are a reliable parameter that can be used for differentiating between benign and malignant breast lesions.
Riassunto
Obiettivo
Scopo di questo studio è stato quello di valutare se in pazienti con sospetto di neoplasia mammaria, la riacquisizione di immagini, 3 ore dopo la somministrazione del radiofarmaco, comporta un miglioramento della sensibilità dell’esame di tomografia ad emissione di positroni con 18F-fluorodesossiglucosio (18F-FDG PET-CT).
Materiali e metodi
Quarantotto pazienti con 59 lesioni mammarie sono state sottoposte a studio 18F-FDG PETCT, in posizione prona, con doppia acquisizione in fase precoce eseguita 1 ora dopo la somministrazione di FDG (PET-1) ed in fase tardiva a distanza di 3 ore (PET-2). Entrambi gli esami sono stati valutati qualitativamente e semi-quantitativamente attraverso il calcolo della variazione media percentuale dei valori di captazione standard (Δ% SUVmax) tra PET-1 e PET-2. Tutte le lesioni che mostravano un SUVmax≥2,5 alla PET-1 o un incremento nei valori di SUV, tra PET-1 e PET-2, sono state considerate maligne. Viceversa, le lesioni che mostravano un SUVmax<2,5 alla PET-1 o una diminuzione dei valori di SUV tra PET-1 e PET-2, sono state considerate benigne. La diagnosi finale istopatologica è stata disponibile per tutte le pazienti incluse in questo studio.
Risultati
La doppia acquisizione della 18F-FDG PET-CT, ha mostrato un’accuratezza diagnostica dell’85%, per le lesioni con un SUVmax≥2,5 e/o con Δ% SUVmax positivo, con valori di sensibilità e specificità dell’81% e del 100% contro 69%, 63% (entrambi, p<0,001) e 100% (p=non stimabile) della singola acquisizione. Le lesioni maligne hanno mostrato, un aumento della captazione di FDG tra PET-1 e PET-2, con un Δ% SUVmax di 10±7 (p<0,04). Viceversa, le lesioni benigne hanno mostrato una diminuzione nei valori di SUV tra PET-1 e PET-2 con Δ% SUVmax di −21±7 (p<0,001).
Conclusioni
La riacquisizione tardiva delle immagini PET migliora l’accuratezza diagnostica della 18F-FDG PET-CT nelle pazienti con sospetta neoplasia mammaria, rispetto alla tecnica eseguita con singola acquisizione. Inoltre, le lesioni mammarie maligne mostrano un incremento della captazione di FDG nel corso del tempo, viceversa, le lesioni benigne mostrano una diminuzione della captazione di FDG. Queste variazioni di captazione di FDG tra PET-1 e PET-2, rappresentano un parametro affidabile, che può essere utilizzato nella differenziazione tra lesioni benigne e maligne della mammella.
Similar content being viewed by others

References/Bibliografia
Jemal A, Siegel R, Ward E et al (2007) Cancer statistics. CA Cancer J Clin 57:43–66
Schirrmeister H, Kuhn T, Guhlmann A et al (2001) Fluorine-18-2-deoxy-2-fluoro-D-glucose PET in the preoperative staging of breast cancer: comparison with the standard staging procedures. Eur J Nucl Med 28:351–358
Eubank WB, Mankoff DA (2005) Evolving role of positron emission tomography in breast cancer imaging. Semin Nucl Med 35:84–99
Matthies A, Hicheson M, Cuchiara A, Alavi A (2002) Dual time point 18F-FDG PET for the evaluation of pulmonary nodules. J Nucl Med 43:871–875
Kumar R, Loving VA, Chauhan A et al (2005) Potential of dual-time-point imaging to improve breast cancer diagnosis with 18F-FDG PET. J Nucl Med 46:1819–1824
Mavi A, Urhan M, Yu JQ et al (2006) Dual Time point 18F-FDG-PET imaging detects breast cancers with high sensitivity and correlates well with histologic subtypes. J Nucl Med 47:1440–1446
American College of Radiology (1995) Breast imaging reporting and data system (BI-RADS). American College of Radiology, Reston
Kennedy BJ (ed) (1992) Manual for the staging of cancer. Lippincott, Philadelphia
Buck A, Schirrmeister H, Kuhn T et al (2002) FDG uptake in breast cancer correlation with biological and clinical prognostic parameters. Eur J Nucl Med Imaging 29:1317–1323
Lowe VJ, Fletcher JW, Gobar L et al (1998) Prospective investigation of positron emission tomography in lung nodules. J Clin Oncol 16:1075–1084
Dewan NA, Gupta NC, Redepenning LS et al (1993) Diagnostic efficacy of FDG-PET imaging in solitary pulmonary nodules. Potential role in evaluation and management. Chest 104:997–1002
Zhuang H, Pourdehnad M, Lambright ES et al (2001) Dual time point FDG PET imaging for differentiating malignant form inflammatory processes. J Nucl Med 42:1412–1417
Hustinx R, Smith RJ, Benard F et al (1999) Dual time point fluorine-18 fluorodeoxyglucose positron emission tomography: a potential method to differentiate malignancy from inflammation and normal tissue in the head and neck. Eur J Nucl Med 26:1345–1348
Koyama K, Okamura T, Kawabe J et al (2002) The usefulness of FDG-PET images obtained 2 hours after intravenous injection in liver tumor. Ann Nucl Med 16:169–176
Torizuka T, Tamaki N, Inokuma T et al (1995) In vivo assessment of glucose metabolism in hepatocellular carcinoma with FDG PET. J Nucl Med 36:1811–1817
Nishiyama Y, Yamamoto Y, Monden T et al (2005) Evaluation of delayed additional FDG-PET imaging in patients with pancreatic tumour. Nucl Med Comm 26:895–901
Avril N, Rosè CA, Schelling M et al (2000) Breast imaging with positron emission tomography and fluorine-18 fluorodeoxyglucose: use and limitations. J Clin Oncol 18:3495–3502
Kumar R, Chauhan A, Zhuang H et al (2006) Standardized uptake values of normal breast tissue with 2-deoxy-2-[F-18]fluoro-D-glucose positron emission tomography: variations with age, breast density, and menopausal status. Mol Imaging Biol 8:355–362
Hellwig D, Graeter TP, Ukena D et al (2007) 18F-FDG PET for mediastinal staging of lung cancer: which SUV threshold makes sense ? J Nucl Med 48:1761–1766
Murthy K, Aznar M, Thompson CJ et al (2000) Results of preliminary clinical trials of the positron emission mammography system PEM-I: a dedicated breast imaging system producing glucose metabolic images using FDG. J Nucl Med 41:1851–1858
Tafra L (2007) Positron emission tomography (PET) and mammography (PEM) for breast cancer: importance to surgeons. Ann Surg Oncol 14:3–13
Weinberg IN, Beylin D, Zavarzin V et al (2005) Positron emission mammography: high-resolution biochemical breast imaging. Technol Cancer Res Treat 4:55–60
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Caprio, M., Cangiano, A., Imbriaco, M. et al. Dual-time-point [18F]-FDG PET/CT in the diagnostic evaluation of suspicious breast lesions. Radiol med 115, 215–224 (2010). https://doi.org/10.1007/s11547-009-0491-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-009-0491-6