
Abstract
Background
Darolutamide, an androgen receptor antagonist with a distinct molecular structure, significantly prolonged metastasis-free survival versus placebo in the phase III ARAMIS study in men with nonmetastatic castration-resistant prostate cancer (nmCRPC). In this population, polypharmacy for age-related comorbidities is common and may increase drug–drug interaction (DDI) risks. Preclinical/phase I study data suggest darolutamide has a low DDI potential—other than breast cancer resistance protein/organic anion transporter protein substrates (e.g., statins), no clinically relevant effect on comedications is expected.
Objective
Our objective was to evaluate the effect of commonly administered drugs on the pharmacokinetics of darolutamide and the effect of comedications potentially affected by darolutamide on safety in patients with nmCRPC.
Patients and Methods
Comorbidities and comedication use in the 1509 ARAMIS participants treated with darolutamide 600 mg twice daily or placebo were assessed. A population pharmacokinetic analysis evaluated whether comedications affected the pharmacokinetics of darolutamide in a subset of 388 patients. A subgroup analysis of adverse events (AEs) in statin users versus nonusers was conducted.
Results
Most participants (median age 74 years) had at least one comorbidity (98.4% in both arms) and used at least one comedication (98.7% with darolutamide vs. 98.0% with placebo); these were similar across study arms. Despite frequent use of comedications with DDI potential, no significant effects on darolutamide pharmacokinetics were identified. Comedications included lipid-modifying agents (34.5%), β-blockers (29.7%), antithrombotics (42.8%), and systemic antibiotics (26.9%). AE incidence was similar across study arms in statin users and nonusers. Study limitations include the small sample size for sub-analyses.
Conclusions
These analyses suggest the pharmacokinetic profile of darolutamide is not affected by a number of commonly administered drugs in patients with nmCRPC. Although pharmacokinetic data have indicated that darolutamide has the potential to interact with rosuvastatin, used to assess DDI in these studies, this finding did not seem to translate into increased AEs due to statin use in the ARAMIS trial.
Clinicaltrials.gov identifier: NCT02200614.
Plain Language Summary
Darolutamide is a medicine used to treat men with prostate cancer that has not spread to other parts of the body (nonmetastatic). Often, these patients are taking other medicines for common age-related illnesses. Taking more than one medicine at the same time increases the chances of what is known as drug–drug interactions. Drug–drug interactions can decrease how well the medicines work or may sometimes increase side effects.
AbstractSection Study AimTo test for possible drug–drug interactions in men with prostate cancer who take darolutamide alongside other medicines.
AbstractSection Study ParticipantsMen with nonmetastatic prostate cancer who were being treated with a medicine that lowers testosterone, a chemical in the body that causes prostate cancer tumors to grow. Participants took two darolutamide 300 mg tablets, or an inactive placebo, twice a day.
AbstractSection What Did the Researchers Measure?The researchers documented the number of medicines taken by each participant and the number of other medical conditions that they had. Tests were done to find out whether other medicines affected the way that darolutamide works in the body and whether patients taking darolutamide alongside other medicines experienced more side effects.
AbstractSection ResultsAs would be expected, based on the typical age of patients with prostate cancer, more than 90% of participants in this study used medicines other than darolutamide to manage common age-related illnesses or medical conditions. Taking medicines alongside darolutamide did not impact how darolutamide worked in the body and did not increase the number of side effects experienced by patients. Darolutamide is known to interact with rosuvastatin, a cholesterol-lowering drug. However, in this study, there was no overall increase in side effects among darolutamide-treated patients who took this type of drug compared with in those who did not.
AbstractSection ConclusionIn this study of patients with nonmetastatic prostate cancer, limited drug–drug interactions were seen when taking darolutamide alongside other medicines given to these patients to manage age-related medical conditions.
Similar content being viewed by others

Polypharmacy for age-related comorbidities is common in patients with nonmetastatic castration-resistant prostate cancer, and this increases the risk of drug–drug interactions (DDIs). |
Subanalyses of the phase III ARAMIS trial indicate that darolutamide has low risk of clinically relevant DDIs with comedications commonly used in these patients. |
1 Introduction
A prime goal of treatment for patients with nonmetastatic castration-resistant prostate cancer (nmCRPC) is to delay progression to metastatic disease (mCRPC) since increased tumor burden is associated with worse prognosis [1], although the recent introduction of multiple life-extending therapies for mCRPC (radium-223, abiraterone, enzalutamide, sipuleucel-T, and taxanes) has extended post-progression survival [2]. Along with disease progression, adverse events (AEs) associated with anticancer therapies may have a detrimental impact on patients’ quality of life [3], particularly in patients with nmCRPC, given the mostly asymptomatic nature of their disease. As nmCRPC is generally diagnosed in older men who are often prescribed multiple concomitant medications for comorbid conditions [4,5,6], the risk of AEs or loss of efficacy resulting from drug–drug interactions (DDIs) is also a fundamental component in clinical decision making [7].
The second-generation androgen receptor inhibitors enzalutamide and apalutamide have recently been approved for the treatment of nmCRPC after demonstrating significantly prolonged metastasis-free survival in phase III clinical trials [8, 9]. However, this change in the treatment landscape has also brought decision-making challenges. Apalutamide and enzalutamide are associated with higher incidences of certain AEs (e.g., falls, fatigue, hypertension, rashes, and seizures) than are placebo. They also both have the potential for DDIs when coadministered with medications that are substrates for several metabolizing enzymes and drug transporters [8,9,10,11,12,13,14]. For example, coadministration of either drug may reduce the exposure of medications that are substrates for the cytochrome P450 (CYP) enzymes CYP3A4, CYP2C9, and CYP2C19 [15, 16], resulting in loss of activity of common comedications such as anticoagulants, antihypertensives, opioid analgesics, and proton pump inhibitors (PPIs).
Darolutamide is a novel androgen receptor antagonist with a unique molecular structure recently approved by the US FDA for the treatment of nmCRPC [17, 18]. In the phase III ARAMIS trial (NCT02200614), darolutamide demonstrated significantly prolonged metastasis-free survival compared with placebo (40.4 vs. 18.4 months; hazard ratio for metastasis or death in the darolutamide group 0.41; 95% confidence interval [CI] 0.34–0.50; p < 0.001) in patients with nmCRPC receiving androgen-deprivation therapy and delayed time to pain progression (40.3 vs. 25.4 months; hazard ratio 0.65; 95% CI 0.53–0.79) [19]. The DDI potential of darolutamide has been extensively investigated in preclinical and clinical phase I studies with metabolizing enzymes and drug transporters. Darolutamide was sensitive to induction of CYP3A4, the main enzyme mediating its metabolism. Inhibition of CYP3A4, P-glycoprotein (P-gp) and breast cancer resistance protein (BCRP)—both transporters for which darolutamide is a substrate—by comedications was not considered clinically relevant. No relevant inhibition of any CYP enzymes by darolutamide was observed in vitro, and in vivo studies found weak induction of CYP3A4 only, suggesting darolutamide may have no clinically relevant effect on comedications metabolized by CYP enzymes [20]. Therapeutic levels of darolutamide were found to have no effect on P-gp substrates [20], though exposure of rosuvastatin, a substrate for BCRP, organic anion-transporting peptide (OATP)1B1, and OATP1B3, was moderately increased by darolutamide coadministration [21]. This effect was mainly attributed to inhibition of BCRP; however, a contribution of OATP inhibition is considered likely. Overall, the results of these studies indicated that darolutamide has a favorable DDI profile.
To evaluate the impact of clinically relevant DDIs with darolutamide in the target patient population, we conducted prespecified and post hoc analyses in patients with nmCRPC who participated in the phase III ARAMIS trial [19], including assessments of comorbidities and comedication use, the effects of concomitant medications on the pharmacokinetics of darolutamide, and the impact of coadministering darolutamide with concomitant medications on patient safety. Given that statin use is very common in this population and darolutamide has been observed to increase rosuvastatin exposure [21], we conducted a subanalysis of the impact of using concomitant statins with darolutamide on patient safety.
2 Patients and Methods
2.1 Trial Design
The phase III ARAMIS trial (NCT02200614) protocol and design have been described in detail elsewhere [19]. Briefly, this was a randomized, double-blind, placebo-controlled, phase III clinical trial conducted globally in 409 centers in 36 countries to evaluate the efficacy and safety of darolutamide in patients with nmCRPC. The trial was approved by local institutional review boards and was conducted in compliance with the principles of the Declaration of Helsinki and in accordance with the International Conference on Harmonisation guidelines for Good Clinical Practice. All patients provided written informed consent.
2.2 Treatment
Men were randomized 2:1 to receive darolutamide 600 mg twice daily (given as two 300 mg tablets) or placebo while continuing androgen-deprivation therapy. Patients continued study medications until protocol-defined progression, discontinuation due to AEs, or withdrawal of consent.
2.3 Population Pharmacokinetic Model
An exploratory population pharmacokinetic analysis was performed to evaluate the variability in the pharmacokinetics of darolutamide, its two pharmacologically active diastereomers, (S,R)-darolutamide and (S,S)-darolutamide, and the active metabolite, keto-darolutamide, based on data generated from the phase III ARAMIS study [19]. The population pharmacokinetic model was developed using data from a subset of patients with valid pharmacokinetic samples collected sparsely at several times during the 12-h application interval (detailed in the Electronic Supplementary Material [ESM]—Methods) and information on drug disposition pathways identified preclinically. The bioanalytical methods used for pharmacokinetic sampling are summarized in the ESM—Methods.
All predefined concomitant medications taken by at least one patient during study treatment were included as a covariate in the population pharmacokinetic model (Table 1 in the ESM). The impact of BCRP inhibitors, CYP3A4 inducers/inhibitors, P-gp inducers/inhibitors, PPIs, and/or uridine 5′-diphospho-glucuronosyltransferase (UGT) inducers/inhibitors on the pharmacokinetics of darolutamide was investigated. Comedications with any relevant DDI potential, weak or strong, were included.
2.4 Safety Analyses
At each study visit, data on treatment-emergent AEs (TEAEs), including type, severity, seriousness, and whether they were related to study treatment based on investigator assessment, were recorded. A subgroup analysis was also performed to compare the incidence of TEAEs for patients receiving statins (3-hydroxy-3-methylglutaryl-coenzyme A reductase inhibitors) versus those not receiving statins. This analysis included all TEAEs reported in concomitant statin users versus nonusers regardless of when the event occurred during the study, i.e., without consideration for when darolutamide and the statin were coadministered. A post hoc analysis evaluating TEAE incidence in patients using statins known to be BCRP substrates versus nonusers of BCRP-substrate statins was also performed.
2.5 Statistical Analysis
Patient demographics, comorbidities, and concomitant medications were summarized descriptively for all randomized patients, i.e., the full analysis set. Comedications were categorized according to potential for relevant DDIs (CYP inducers/inhibitors/substrates, UGT substrates, and drug transporter substrates) based on in vitro and phase I clinical studies of darolutamide [21] and established DDI profiles for the currently available androgen-receptor inhibitors, enzalutamide and apalutamide [11,12,13,14].
Pharmacokinetic model development was conducted via nonlinear mixed-effects modelling using NONMEM (version 7.3, ICON Development Solutions plc, Manchester, UK) and R software [22]. Full details of the population pharmacokinetic analysis are given in the ESM—Methods.
Safety evaluations were conducted in all patients who were randomized and received at least one dose of study medication.
3 Results
3.1 Patients
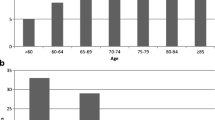
In total, 1509 men were randomized to darolutamide (n = 955) or placebo (n = 554) in addition to androgen-deprivation therapy. One patient randomized to the darolutamide arm did not receive study treatment and was therefore excluded from the safety analyses [19]. Baseline demographic and clinical characteristics were similar in the two treatment groups (Table 1). Median age was 74 years in both groups, and median follow-up time was 17.9 months. Most patients had at least one comorbid condition (98.4% in both treatment arms); the most common comorbidities were hypertension, obesity, anomalies of lipid metabolism, and diabetes (Table 2).
3.2 Concomitant Medication Use
The overwhelming majority of men in the trial were receiving at least one concomitant medication, and rates of comedication use were balanced across the two treatment arms: 98.7% with darolutamide and 98.0% with placebo (Table 3). The most common concomitant medications for comorbid conditions in darolutamide- versus placebo-treated patients were antihypertensives, including drugs affecting the renin–angiotensin system (54.7 vs. 49.8%), β-blockers (29.6 vs. 27.6%), and calcium channel blockers (22.7% in both arms), as well as analgesics (53.8 vs. 50.4%), whereas more than one-third of patients received antithrombotics (42.8 vs. 39.7%) or lipid-modifying agents (34.5 vs. 39.4%). Other cardiovascular agents, diuretics, urological agents, PPIs, systemic antibiotics, and anti-inflammatory/antirheumatic agents were used by at least 20% of patients. These comedications span a range of agents that act as inducers, inhibitors, or substrates of the enzymes predominantly involved in drug metabolism or key drug transporters (e.g., P-gp, BCRP, OATP1B1, OATP1B3) (Table 3).
3.3 Population Pharmacokinetic Analysis
In total, 388 patients (40% of the total who received darolutamide in the phase III trial) were included in the pharmacokinetic subset. Demographics and baseline characteristics were generally similar to those of the overall darolutamide-treated population, although the pharmacokinetic subset contained higher proportions of Japanese patients and patients with mild renal impairment (Table 1).
Evaluation of the population pharmacokinetic analysis showed that none of the comedications included as covariates in the population pharmacokinetic base model met the criteria for a significant covariate effect. These comedications included CYP3A4 inhibitors (21.6%), P-gp inhibitors (20.1%), PPIs (15.2%), BCRP inhibitors (14.9%), UGT1A9 inhibitors (2.8%), and CYP3A4 inducers (0.5%); examples of drugs in these categories are given in Table 3. No patients received P-gp or UGT1A9 inducers. PPIs exerted no effect on darolutamide clearance. It was not possible to specifically assess an effect of CYP3A4 inducers as so few patients received comedications that were CYP3A4 inducers, such as rifampicin or carbamazepine. These data suggest that, although preclinical data indicate darolutamide exposure may be affected by drugs that are strong CYP3A4 and P-gp inducers or inhibitors [23], there was no significant association between the use of concomitant medications and the pharmacokinetic variability of darolutamide in this study.
3.4 Impact on Adverse Event Incidence of Drugs Coadministered with Darolutamide, Including Breast Cancer Resistance Protein Substrates
We also assessed whether the DDIs that have been identified as clinically relevant for darolutamide (notably, sensitivity to strong CYP3A4 inducers and inhibition of BCRP by darolutamide [23]) had a possible impact on the safety of patients in the ARAMIS trial population. As already noted, the common concomitant medications received by patients in ARAMIS were similar between study arms (Table 3). We have previously reported that the incidence of the most common AEs was similar in patients treated with darolutamide and those who received placebo, and permanent discontinuations of the study drug due to AEs occurred in similar proportions of patients in each treatment arm [19].
Concomitant use of statins was similar in the darolutamide and placebo arms (32.1 vs. 36.5%; Table 4). In both treatment arms, the incidence of TEAEs was comparable between patients receiving concomitant statins and those not receiving statins (88.2 vs. 80.9% for darolutamide and 82.2 vs. 73.9% for placebo; Table 4). With respect to the type of AEs reported (based on system organ class and preferred term), no differences among statin users in either treatment arm was observed. No meaningful differences in alanine aminotransferase (ALT) values occurred between concomitant statin users and nonusers: in both treatment arms, mean ALT values were slightly higher among statin users than nonusers at baseline and throughout the treatment period. In a subset of patients using statins that are BCRP substrates (approximately 30% of the overall population; Table 2 in the ESM), predefined AEs known to be associated with statins occurred more frequently with darolutamide than placebo (8.6 vs. 3.5%; Table 5). This difference was due to greater incidences of abnormalities in laboratory parameters. A similar difference was observed in the overall study population, indicating that the difference occurred independently of statin exposure and excluding any relevant impact of darolutamide in statin users. The abnormalities in laboratory parameters were notably increased aspartate aminotransferase levels (1.4% with darolutamide vs. 0.2% with placebo, respectively) and increased blood bilirubin levels (1.3% with darolutamide vs. 0% with placebo).
4 Discussion
The potential for DDIs is an important consideration when selecting an androgen receptor-targeting therapy for patients with nmCRPC. Loss of efficacy with treatments for patients’ comorbidities or sustaining an increased risk of AEs are potential outcomes of DDIs [10, 24]. Extensive investigation in preclinical/phase I studies indicated that darolutamide has a favorable DDI profile. Overall, few DDIs were identified at clinically relevant levels: darolutamide was sensitive to CYP3A4 induction, but no clinically relevant effects on darolutamide were expected from drugs that act as inhibitors of CYP enzymes and drug transporters.
Most importantly, darolutamide had few effects on other drugs used to treat comorbid conditions; increased exposure of rosuvastatin was the only interaction of note [23]. This interaction was mainly attributed to BCRP inhibition, although darolutamide-mediated inhibition of OATP transporters may have contributed to the observed effect. By contrast, enzalutamide is a strong CYP3A4 inducer and a moderate CYP2C9 and CYP2C19 inducer, and apalutamide is a strong inducer of CYP3A4 and CYP2C19 and a weak inducer of CYP2C9, UGT, P-gp, BCRP, and OATP1B1 [11, 14]. Additional monitoring may be required as both drugs may lead to suboptimal bioavailability of comedications with potential loss of efficacy.
The present analyses of the phase III ARAMIS trial demonstrated that almost all patients with nmCRPC receiving androgen-deprivation therapy with androgen receptor inhibitor therapy have comorbid conditions that require the use of concomitant medications. Individual patient data in ARAMIS indicated that many patients were receiving multiple comedications, as others have also reported [10]. As expected in this population (median age 74 years), the most common comorbidities included hypertension and other cardiovascular disorders, obesity, hyperlipidemia, osteoarthritis, and diabetes. Consistent with the comorbidities reported, the most frequently prescribed comedications were antihypertensives and agents for other cardiovascular disorders, along with a need for analgesia, treatments for urological and acid-related gastrointestinal disorders, antidepressants, anxiolytics, and dementia treatments. Our population pharmacokinetic analysis demonstrated that these frequently used concomitant drugs had no significant effect on the pharmacokinetics of darolutamide. Comedications that are potent CYP3A4 inducers were rarely used by the overall ARAMIS population, so the risk of DDIs may also be low in clinical practice.
Only the interaction between darolutamide and the combined BCRP and OATP substrate rosuvastatin has been deemed clinically relevant [23], though our safety subgroup analysis in statin users and nonusers could not clearly attribute any imbalance between the treatment arms to the effect of darolutamide on statins. However, the small sample size may preclude observation of rare AEs such as myopathy or rhabdomyolysis, although these are well-characterized and can readily be monitored. Overall, the incidence of AEs did not appear to be increased significantly by DDIs, as similar AE rates are reported with darolutamide and placebo despite the equally high use of concomitant medications in both treatment arms in the ARAMIS study [19]. This observation includes AEs previously reported more frequently with enzalutamide and apalutamide versus placebo in phase III trials (PROSPER and SPARTAN, respectively) such as falls, hypertension, and central nervous system (CNS)-related AEs [8, 9].
The risk of AEs resulting from DDIs is an important consideration for physicians. Enzalutamide and apalutamide have been identified as substrates, inducers, and/or inhibitors of metabolizing enzymes and inhibitors or inducers of drug transporters [15, 16, 25, 26]. Given that the majority of drugs are metabolized by at least one CYP enzyme [4], enzalutamide and apalutamide have the potential for DDIs with a range of medications that are commonly used by patients with prostate cancer, e.g., gastrointestinal, cardiovascular, and analgesic agents (Table 6) [10, 15, 16, 24,25,26]. Consequently, the FDA labels for enzalutamide and apalutamide suggest avoiding the use of susceptible comedications and warn of the potential loss of efficacy of these comedications, respectively [11, 14]. In a retrospective review of pharmacy records for patients with mCRPC, enzalutamide was associated with a high prevalence of potential DDIs with CNS drugs (e.g., opioid analgesics), which could increase the risk of cognitive adverse effects, falls, and fractures [10]. In addition, enzalutamide reduces plasma concentrations of PPIs, which increases the risk of bleeding events in patients receiving PPIs in combination with aspirin or nonsteroidal anti-inflammatory drug prophylaxis. Overall, 85% of patients with mCRPC who received enzalutamide were at risk for DDIs that would require treatment modification of at least one comedication [10]. In a post hoc analysis of the phase III SPARTAN trial, the risk of falls was increased in patients receiving apalutamide and concomitant α-blockers or antidepressants [27]. Hence, the safety of prescribing androgen receptor inhibitors in the setting of polypharmacy warrants consideration by the treating physician.
Limitations of our study include the small sample size of the safety subanalyses and the population pharmacokinetic analysis and that the population pharmacokinetic analysis did not investigate the effect of darolutamide on the pharmacokinetics of comedications. Strong CYP3A4 and P-gp inducers were identified as having a relevant effect on darolutamide, but such comedications were rarely used in ARAMIS. For example, the strong CYP3A4-inducing anti-epileptic drugs, carbamazepine, phenytoin, and phenobarbital, were used by few patients. However, as patients with severe infections (which may be treated with systemic antibiotics such as rifampicin) and other serious comorbidities (e.g., recent stroke or myocardial infarction, active viral hepatitis, or human immunodeficiency virus) were excluded, the ARAMIS population did not fully represent the real-world population likely to receive darolutamide treatment. Multiple interactions between drugs were possible since many patients received several comedications, but it was not possible to assess the impact of these on patient safety in our analyses. Our identification of potential DDIs is not exhaustive—DDIs may occur with drugs not investigated in preclinical and phase I studies to date, and DDIs may be specific to individual drugs within a drug class. The safety profile of darolutamide will continue to be monitored in post-marketing studies.
5 Conclusions
These analyses of ARAMIS data suggest a limited potential for clinically relevant DDIs between darolutamide and comedications frequently used to treat age-related comorbidities in patients with nmCRPC (Table 6). Interactions noted with the combined BCRP and OATP substrate rosuvastatin did not seem to translate into increased AEs in the ARAMIS trial to date. Determining the risk–benefit balance of androgen receptor-targeted therapies for patients with nmCRPC who receive multiple comedications is important for optimal management. The findings presented here provide additional information for clinical decision making.
Data Sharing
Availability of the data underlying this publication will be determined according to Bayer’s commitment to the EFPIA/PhRMA “Principles for responsible clinical trial data sharing.” This pertains to scope, timepoint, and process of data access. As such, Bayer commits to sharing upon request from qualified scientific and medical researchers patient-level clinical trial data, study-level clinical trial data, and protocols from clinical trials in patients for medicines and indications approved in the United States (US) and European Union (EU) as necessary for conducting legitimate research. This applies to data on new medicines and indications that have been approved by the EU and US regulatory agencies on or after 1 January 2014. Interested researchers can use http://www.clinicalstudydatarequest.com to request access to anonymized patient-level data and supporting documents from clinical studies to conduct further research that can help advance medical science or improve patient care. Information on the Bayer criteria for listing studies and other relevant information is provided in the Study sponsors section of the portal. Data access will be granted to anonymized patient-level data, protocols, and clinical study reports after approval by an independent scientific review panel. Bayer is not involved in the decisions made by the independent review panel. Bayer will take all necessary measures to ensure that patient privacy is safeguarded.
References
National Cancer Institute. Surveillance, epidemiology, and end results program. Cancer stat facts: prostate cancer. 2019. https://seer.cancer.gov/statfacts/html/prost.html. Accessed 16 May 2019.
Francini E, Gray KP, Shaw GK, Evan CP, Hamid AA, Perry CE, et al. Impact of new systemic therapies on overall survival of patients with metastatic castration-resistant prostate cancer in a hospital-based registry. Prostate Cancer Prostatic Dis. 2019;22(3):420–7. https://doi.org/10.1038/s41391-018-0121-2.
Basch E, Autio K, Ryan CJ, Mulders P, Shore N, Kheoh T, et al. Abiraterone acetate plus prednisone versus prednisone alone in chemotherapy-naive men with metastatic castration-resistant prostate cancer: patient-reported outcome results of a randomised phase 3 trial. Lancet Oncol. 2013;14(12):1193–9. https://doi.org/10.1016/S1470-2045(13)70424-8.
Del Re M, Fogli S, Derosa L, Massari F, De Souza P, Crucitta S, et al. The role of drug-drug interactions in prostate cancer treatment: focus on abiraterone acetate/prednisone and enzalutamide. Cancer Treat Rev. 2017;55:71–82. https://doi.org/10.1016/j.ctrv.2017.03.001.
Stepney R, Lichtman SM, Danesi R. Drug-drug interactions in older patients with cancer: a report from the 15th Conference of the International Society of Geriatric Oncology, Prague, Czech Republic, November 2015. Ecancermedicalscience. 2016;10:611. https://doi.org/10.3332/ecancer.2016.611.
Bohnert T, Patel A, Templeton I, Chen Y, Lu C, Lai G, et al. Evaluation of a new molecular entity as a victim of metabolic drug-drug interactions-an industry perspective. Drug Metab Dispos. 2016;44(8):1399–423. https://doi.org/10.1124/dmd.115.069096.
Guthrie B, Makubate B, Hernandez-Santiago V, Dreischulte T. The rising tide of polypharmacy and drug-drug interactions: population database analysis 1995-2010. BMC Med. 2015;13:74. https://doi.org/10.1186/s12916-015-0322-7.
Hussain M, Fizazi K, Saad F, Rathenborg P, Shore N, Ferreira U, et al. Enzalutamide in men with nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2018;378(26):2465–74. https://doi.org/10.1056/NEJMoa1800536.
Smith MR, Saad F, Chowdhury S, Oudard S, Hadaschik BA, Graff JN, et al. Apalutamide treatment and metastasis-free survival in prostate cancer. N Engl J Med. 2018;378(15):1408–18. https://doi.org/10.1056/NEJMoa1715546.
Benoist GE, van Oort IM, Smeenk S, Javad A, Somford DM, Burger DM, et al. Drug-drug interaction potential in men treated with enzalutamide: mind the gap. Br J Clin Pharmacol. 2018;84(1):122–9. https://doi.org/10.1111/bcp.13425.
Astellas Pharma US Inc. Xtandi (enzalutamide) US prescribing information. 2018. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/203415s014lbl.pdf. Accessed 11 June 2019.
European Medicines Agency. Summary of product characteristics: XTANDI. 2019. https://www.ema.europa.eu/en/documents/product-information/xtandi-epar-product-information_en.pdf. Accessed 11 June 2019.
European Medicines Agency. Summary of product characteristics: ERLEADA. 2019. https://www.ema.europa.eu/en/documents/product-information/erleada-epar-product-information_en.pdf. Accessed 11 June 2019.
Janssen Ortho LLC. Erleada (apalutamide) US prescribing information. 2018. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/210951s000lbl.pdf. Accessed 22 July 2019.
European Medicines Agency. Xtandi CHMP assessment report. 2013. http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002639/WC500144998.pdf. Accessed 1 Oct 2018.
European Medicines Agency. Erleada CHMP assessment report. 2018. https://www.ema.europa.eu/en/documents/assessment-report/erleada-epar-public-assessment-report_en.pdf. Accessed 1 Oct 2018.
Fizazi K, Smith MR, Tombal B. Clinical development of darolutamide: a novel androgen receptor antagonist for the treatment of prostate cancer. Clin Genitourin Cancer. 2018;16(5):332–40. https://doi.org/10.1016/j.clgc.2018.07.017.
US Food and Drug Administration. FDA approves darolutamide for non-metastatic castration-resistant prostate cancer. 2019. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-darolutamide-non-metastatic-castration-resistant-prostate-cancer. Accessed 31 July 2019.
Fizazi K, Shore N, Tammela TL, Ulys A, Vjaters E, Polyakov S, et al. Darolutamide in nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2019;380(13):1235–46. https://doi.org/10.1056/NEJMoa1815671.
Zurth C, Graudenz K, Denner K, Vairlein M, Korjamo T, Fricke R, et al. Drug-drug interaction of darolutamide with cytochrome P450 and P-glycoprotein substrates: results from clinical and in vitro studies. San Francisco: ASCO Genitourinary Cancers Symposium; 2019.
Zurth C, Koskinen M, Fricke R, Prien O, Korjamo T, Graudenz K, et al. Drug–drug interaction potential of darolutamide: in vitro and clinical studies. Eur J Drug Metab Pharmacokinet. 2019. https://doi.org/10.1007/s13318-019-00577-5.
R (Version 3.1.1) Development Core Team. R: a language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2008.
Bayer HealthCare Pharmaceuticals Inc. Nubeqa (darolutamide) US prescribing information. 2019. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/212099Orig1s000lbl.pdf. Accessed 31 July 2019.
Benoist GE, van Oort IM, Burger DM, Koch BCP, Mehra N, van Erp NP. The combination of enzalutamide and opioids: a painful pitfall? Eur Urol. 2019;75(2):351–2. https://doi.org/10.1016/j.eururo.2018.09.011.
US Center for Drug Evaluation and Research. NDA/BLA clinical pharmacology and biopharmaceutics review NDA 203415 Xtandi (enzalutamide). 2012. https://www.accessdata.fda.gov/drugsatfda_docs/nda/2012/203415Orig1s000ClinPharmR.pdf. Accessed 26 Sept 2018.
US Center for Drug Evaluation and Research. NDA/BLA multi-disciplinary review and evaluation NDA 210951 Erleada (apalutamide). 2018. https://www.accessdata.fda.gov/drugsatfda_docs/nda/2018/210951Orig1s000MultidisciplineR.pdf. Accessed 26 Sept 2018.
Pollock Y, Smith M, Saad F, Chowdhury S, Oudard S, Hadaschik B, et al. Predictors of falls and fractures in patients (pts) with nonmetastatic castration-resistant prostate cancer (nmCRPC) treated with apalutamide (APA) plus ongoing androgen deprivation therapy (ADT). J Clin Oncol. 2019;37(15_suppl):5025. https://doi.org/10.1200/jco.2019.37.15_suppl.5025.
Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2012;3:1–150.
Hansten PD, Horn JR. Top 100 drug interactions 2018. A guide to patient management. 19th ed. LLP: H&H Publications; 2018.
US Food and Drug Administration. Drug development and drug interactions: table of substrates, inhibitors and inducers. 2017. https://www.fda.gov/drugs/drug-interactions-labeling/drug-development-and-drug-interactions-table-substrates-inhibitors-and-inducers. Accessed 15 Aug 2019.
National Cancer Institute. Common Terminology Criteria for Adverse Events, version 4.03. Bethesda, MD: Cancer Therapy Evaluation Program. 2010. https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm. Accessed 16 Sept 2019.
De Gregori S, De Gregori M, Ranzani GN, Allegri M, Minella C, Regazzi M. Morphine metabolism, transport and brain disposition. Metab Brain Dis. 2012;27(1):1–5. https://doi.org/10.1007/s11011-011-9274-6.
Ge S, Tu Y, Hu M. Challenges and opportunities with predicting in vivo phase II metabolism via glucuronidation from in vitro data. Curr Pharmacol Rep. 2016;2(6):326–38. https://doi.org/10.1007/s40495-016-0076-8.
Acknowledgements
The authors thank the patients, their families, and all investigators involved in this study. The authors wish to acknowledge the contribution of Christian Kappeler and Marie-Aude Le Berre for statistical analysis performed from the ARAMIS study. Medical writing support, including assisting authors with the development of the outline and initial draft and incorporation of comments was provided by Tamsin Williamson, and editorial support, including formatting, proofreading, and submission was provided by Annabel Ola and Beth King all of Scion Medica, London, supported by Bayer AG according to Good Publication Practice guidelines (http://annals.org/aim/article/2424869/good-publication-practice-communicating-company-sponsored-medical-research-gpp3). The study sponsors Bayer AG and Orion Pharma were involved in the study design, collection, analysis and interpretation of data. However, ultimate responsibility for opinions, conclusions, and data interpretation lies with the authors.
Author information
Authors and Affiliations
Contributions
CZ, RF, HG, MK, BP, OP, GB, OP, and IK contributed to the conception and design of the study; NS, CZ, RF, HG, KG, MK, BP, OPr, GB, OP, TLT, IK, FV, MS, and KF contributed to the acquisition of data; NS, RF, HG, BP, GB, OP, TLT, IK, FV, MS, and KF contributed to the analysis and interpretation of the data; NS and KF drafted the manuscript; BP and JM carried out the statistical analysis; all authors provided critical revision of the manuscript for important intellectual content.
Corresponding author
Ethics declarations
Funding
This work was supported by Bayer HealthCare and Orion Pharma.
Conflict of interest
Dr. Shore reports personal fees from Ferring, Bayer, Amgen, Janssen, Dendreon, Tolmar, Astellas, Pfizer, AstraZeneca, Genentech/Roche, Myovant Sciences, Merck, AstraZeneca, Bristol Meyers Squibb, and Nymox outside the submitted work. Drs. Zurth, Fricke, Gieschen, Graudenz, Ploeger, Prien, Borghesi, Petrenciuc, and Kuss report employment by and stock ownership in Bayer. Dr. Koskinen reports employment by and stock ownership in Orion. Dr. Moss reports personal fees from Akari, AstraZeneca, Bayer, Carrick Therapeutics, Debiopharm, Orphazym, Proveca, Richmond Pharmacology, and the University of Leicester outside the submitted work. Dr. Tammela reports personal fees from Janssen, and grants and personal fees from Bayer, Lidds AB, and Astellas, outside the submitted work. Dr. Verholen reports employment by Bayer. Dr. Smith reports personal fees from Amgen, Astellas, Bayer, Clovis, Gilead, Janssen, Lilly, Novartis, and Pfizer, outside the submitted work. Dr. Fizazi reports personal fees from Amgen, Astellas, AstraZeneca, Bayer, Clovis, Curevac, ESSA, Janssen, Orion Pharma, Roche/Genentech, and Sanofi outside the submitted work.
Informed consent
Informed consent was obtained from all individual participants in the study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Shore, N., Zurth, C., Fricke, R. et al. Evaluation of Clinically Relevant Drug–Drug Interactions and Population Pharmacokinetics of Darolutamide in Patients with Nonmetastatic Castration-Resistant Prostate Cancer: Results of Pre-Specified and Post Hoc Analyses of the Phase III ARAMIS Trial. Targ Oncol 14, 527–539 (2019). https://doi.org/10.1007/s11523-019-00674-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11523-019-00674-0