
Abstract
Democracy is generally associated with governmental accountability, better public policy choices and public health. However, there is limited evidence about how political regime transition impacts public health. We use two samples of the states around the world to trace the impact of regime transition on public health: the first sample comprises 29 post-communist states, along with 20 consolidated democracies, for the period of 1970–2014; the second sample is a subsample of the same 29 post-communist states but only for the period of transition, 1990–2014. We find that the post-communist states experienced some decline in life expectancy in the first few years of transition (1990–1995). Yet, with a steady increase in the measure of democracy from 1995 onwards, life expectancy significantly improved and infant mortality decreased. Therefore, in the long run, democratization has had a positive impact on both the life expectancy and infant mortality of citizens of the post-communist states.
Similar content being viewed by others


1 Introduction
Studies of the consequences of democracy for society, politics, and economic development have pursued many different avenues.Footnote 1 Scholars have argued that a higher level of democracy is associated with an improvement in a wide range of such social factors as political and social trust, levels of corruption, quality of life, quality of air and environmental policy, education and life satisfaction, among others (Van Erkel & Van Der Meer, 2016; Arpino & Obydenkova, 2020; Obydenkova & Arpino, 2018; Rohrschneider, 2002; Mayne & Hakhverdian, 2017; Brewer, et al., 2004; Libman & Obydenkova, 2014; Obydenkova et al., 2016; Uslaner, 2017, 2018; Armingeon & Guthmann, 2014; Obydenkova & Salahodjaev, 2016, 2017). Within political analysis and international relations, scholars debate the role of democracy in international alliances, membership in international organizations, fulfillment of international agreements and international commitments, as well as an array of values and attitudes (Anderson, 1998; Anderson & Tverdova, 2003; Hobolt, 2012; Libman & Obydenkova, 2013b, 2018a, b; Mungiu-Pippidi, 2015; Newton, 2001). Finally, from an economics perspective, studies on the effects of democracy on various indicators of economic development are countless, including economic modernization, foreign trade, exports, inequality, and the analysis of the nexus of democracy, bureaucracy, territorial (de-)centralization, and even firm innovation (e.g., Brown et al., 2009; Akhmedov & Zhuravskaya, 2004; Keefer, 2007; Nazarov & Obydenkova, 2020; Libman & Obydenkova, 2013a, 2019; Obydenkova & Swenden, 2013; Milanovic, 1999). Yet, despite this fast-growing literature on the effects of democracy on socio-economic and political variables, there are significantly fewer studies on the implications of variation in democracy for public health, and the available findings are somewhat controversial. Our understanding of the implications of democracy for public health is more limited and inconclusive as compared to studies of other effects of democracy (Ghobarah et al., 2004, p. 73).
In fact, the logic linking democracy and public health is somewhat similar to the causal links identified in the above studies on other effects of democracy. As these studies have demonstrated, democracy is generally associated with the highest level of governmental accountability to people, transparency, independent and critical mass media, better public policy choices, better access to education, information, and health services, lower corruption, and a higher quality of life in general. These factors all result in hypothetically improved health policy and public health.Footnote 2 Despite this obvious theoretical links between consolidated democracy and public health, studies on variations in the level of democracy and so-called democracy stock over regime transition are somewhat less conclusive. This does not seem surprising, as the latest wave of regime transition started only in the late 1980s and the early 1990s for 29 post-communist states in Central Europe and Central Asia, and since that time they have consolidated different types of political regime. While most of the European post-communist states became EU members and consolidated democratic regimes, others, especially those in Asia, became autocracies (e.g., Turkmenistan and Kazakhstan) or hybrid regimes. There is still limited evidence about how this latest wave of regime transition has impacted different aspects of public health, and what causal links were involved in this. To address this relatively newly emerged research challenge, we use global evidence through analysis of two samples of the states around the world to trace the impact of regime transition on two main aspects of public health: the first sample comprises 29 post-communist states, along with 20 consolidated democracies, for the period 1970–2014 (thus, accounting for the level of public health before transition started—this is highly important for our cross-decade comparison, something that is often missing in other studies). Unlike other papers focusing either on infant mortality or on life expectancy, our project includes both indicators as this allows for more nuanced comparative analysis.
In addition to consideration of both life expectancy and infant mortality, another aspect we introduce here is taking the 1970s as a departure point for empirical analysis. The focus on public health during communism in the 1970s presents an excellent departure point for our study and allows for a more complete analysis of the changes taking place over these 45 years. To complement this further, the second sample is a subsample of the same 29 post-communist states but only for the period of transition, 1990–2014. This later period reflects the changes that took place throughout the 1990s but it also encompasses the 25 years after 1989—thus reflecting the short-run versus long-run effects of transition on public health. We find that the post-communist states experienced a significant decline in life expectancy and some increase in infant mortality during the period of transition. Overall, we find evidence that in the long run, democratization has a positive impact on both the life expectancy and infant mortality of citizens of the post-communist states.
The paper proceeds as follows. The next section gives an overview of the controversial literature on the democracy– public health nexus, and sets out hypotheses. The third section outlines the empirical model and discusses the data. The fourth section presents the main analysis and findings. The fifth section provides a further detailed discussion of causal mechanisms. Section six concludes.
2 Democracy, Transition, and Public Health
A rich set of studies has explored the effects of democracy on public health, exhibiting somewhat controversial results. Some scholars have argued that democracy is associated with higher governmental accountability to the population, and thus better public policy choices, including in public health policy, freedom of mass media that is critical of governmental choices, electoral cycles that stimulate the government to be attentive to the electorate, better education, lower levels of corruption, that is also influenced a number of a number of external factors and historical legacies both democracy- and autocracy-reinforcing (Franco et al., 2004; Besley & Kudamustu 2006; Wigley & Akkoyunlu-Wigley, 2011, 2017; Gerring et al., 2008; Obydenkova & Libman, 2012, 2015; Alfaro 2012). Departing from these different perspectives, one may expect a positive impact of democracy on citizens’ health. Specifically, in a more democratized society, we conjecture that citizens enjoy a higher level of life expectancy and a lower level of infant mortality. Given that democracy is associated with electoral turnover: government depends on the electoral choices of the population, leading to higher governmental transparency and awareness of the electorate, a better system of education and higher enrollment in secondary education, and lower levels of corruption and clientalism (Akhmedov & Zhuravskaya, 2004; Baum & Lake, 2003). Among other factors, freedom of the mass media is one of the best triggers of a better quality of services (including the quality of medical care and access to it). Thus, governmental choices regarding public health policies have a direct impact on the re-election of executives and the legislature. Yet this is true only within a democratic context. In contrast, in a totalitarian and autocratic context, where electoral results are either faked or have no impact, or simply do not exist, the government is not accountable to the population in its policy choices, including in public health policy.
However, a few studies specifically on infant mortality and life expectancy have challenged these findings. Among others, Ross (2006) asks a more straightforward question: is democracy beneficial for the health of the poorest social layer and for the most economically disadvantaged social class? In case of post-Communist transition, another study stated that “privatization is significantly associated with fertility decline, explaining approximately half of the overall fertility decline across the 52 towns and the 28 countries” (Scheiring et. al. 2020, p. 1). The effect of variation in democracy for public health was also discovered at cross-subnational levels of post-Communist regions. The study argues that more democratic subnational regions “produce better results than the less competitive ones” in terms of public health outcomes (Rosenberg et. al. 2018: 20; also see Danilova et. al. 2016). Looking specifically at two (arguably the most important) indicators—on infant and child mortality—he comes to the conclusion that democracy has no effect at all on the public health of the poorest social layers. While admitting that democracies in general tend to disperse more funding for public health and education, he points out that this funding does not reach the poorest layers of the population, while improving life for the middle and upper-middle classes. In a way, this conclusion makes sense if we recall that democracies make decisions that are favorable for their main electorate: that is, the middle class. When it comes to the poorest social layers, their voting activities are practically non-existent (Bartel et al., 2017), which decreases governmental initiatives to promote (health) public policies that are favorable for the lower class within the electorate. While the findings of Ross (2006) spurred a vivid debate and criticism among scholars (e.g., Martel Garcia 2014), he was not the only one to challenge the democracy–health nexus. Another recent study by Mackenbach et al., (2013a, 2013b) on life expectancy also casts some doubts on the previous consensus in the literature. The study reports the possible short-run negative impact of democracy on life expectancy in European states. The study’s findings could be considered as a statistical anomaly since it seems hard to explain the negative link between democracy and an individual’s health. On the other hand, this study was based on data gathered for the period 1987–2008, capturing radical changes in political regimes across Central European countries that were transitioning from socialism to capitalism. In the early period of transition, the changes in political and economic institutions in the Eastern European countries were accompanied with drastic changes in the standard of living and massive declines in public spending on health care due to the financial crisis associated with radical regime change.
Another factor that has been omitted so far in studies on regime transition is changes in public behavior during the regime transition. The collapse of the political system is associated with more than just economic hardship: it also represents a lost system of values and a lost ideology that had provided the sense and meaning of life for decades and across the generations, especially within the Soviet states. The loss of ideology, along with economic crisis, may trigger higher consumption of alcohol, and an increase in the suicide rate and in participation in risky behavior, among other issues (Balabanova et al., 2012; Rechel & McKee, 2009; Shishkin, 2013; Walberg et al., 1998). Some studies have specifically analyzed the decline in public health during the early 1990s (1990–1994), looking at how and why socio-economic changes led to a decline in life expectancy (Walberg et al., 1998). Some studies have gone beyond purely socio-economic changes, poverty, increased inequality, and unaffordable medical care, and have considered the psychological aspect of regime transition for public health. In addition to the financial crisis in the 1980s and 1990s, and uncertainty, people’s hopes “that their lives would improve were quickly dashed by the bumpy transition to a market economy. Disillusionment led to stress and depression, and depression was a harbinger of death” (Stone, 2000, p. 1732). Depression and disillusionment also went in hand in hand with increases in the consumption of (cheap and often home-cooked) alcohol as the only available and affordable form of drug. One may further conjecture that regime transition and radical social, economic, and political changes altogether triggered not only an increase in alcohol consumption, but also in other forms of health-risky behavior in general (such as an increase in crime and suicide), and contributed to a decline in health in the adult population (Denisova & Shapiro, 2013). Thus, freedom in decision-making and personal expression, the essential outcomes of democratization, may have led to the increased consumption of alcohol and tobacco products that were more available to the public within the context of a market economy, as compared to the previously centralized economy characterized by a high deficit of products and totalitarian control over the production and sale of, for example, alcoholic beverages (Stone, 2000). At the same time, the increased prevalence of mental illness because of depression, associated with the economic-related hardship of transition, and also with the loss of the ideology that had fomented the sense of life of the different generations, may have had an increase in the suicide rate (Denisova & Shapiro, 2013; Stone, 2000). Finally, the prolonged and painful experience of transition may have led to increased engagement in substance abuse or risky sexual behavior, leading to increased unwanted pregnancy among adolescents (Stickley et al., 2014). We refer to this link as a behavioral effect of democratization on public health. In the final analysis, we test the ability of both effects to explain the link between democracy and population health.
Therefore, to complement the existing studies, in this paper we account for two hypothetical causal mechanisms that link regime transition and public health. First, we consider the changes in governmental spending for public health policy. Second, we also consider the changes in public behavior caused by the disruption of the political regime.
3 Conceptual Framework and Empirical Models
-
a.
Conceptual Framework
The Grossman model is a primary theoretical framework in health economics that outlines the way a typical individual makes his/her investment decision with respect to health (Keiding, 2018). The main implication of the model is that optimal health is determined at the point where marginal efficiency of health capital equates with cost of capital (see Fig. 1). In this model, marginal efficiency of health capital is a measure which captures the lifetime return from an investment in health for the given level of health stock. To demonstrate how optimal health is determined, suppose an individual who experiences health depreciation at a variable rate \(\delta\) faces a choice whether to invest part of his disposable income either to improve health with a lifetime return from this investment equaling \(R\), or to lend these resources to someone in the money market with the interest payment of \(r\). If the return on health investment minus health depreciation pays him more than the money market, then the individual decides to invest the part of his disposable income in health. Thus, the decision-making rule can be outlined by the following inequality, \(R\ge r+\delta\), where the right-hand side of the inequality represents the cost of health capital.
Suppose the government partially subsidizes the individual’s investment in health, let us say through various public investment initiatives. The level of subsidization is given by some parameter, θ which can have a value between 0 and 1. The net return on health investment then becomes \((1+\theta )R-\delta\) and the individual will invest in health if the lifetime return, \(R\), is greater than the redefined cost of health capital, \(\frac{r+\delta }{1+\theta }\). Since the optimal health of the individual is the point where the cost of capital equates with the marginal efficiency of capital or lifetime benefit of health investment (see Fig. 1), it depends on the interest rate in the money market, depreciation of health capital, and the level of public investment.
This model can be a good tool for tracking how democratic processes in the post-communist countries impacted the health stock of citizens if we know which parameters are affected by these processes and which directions. Of the three parameters, the democratic process may directly impact the rate of depreciation of health capital, especially during the transition period, \(\delta\). This mechanism can be the so-called behavioral effect. Democratization may also directly affect the level of subsidization of health investment, θ introducing the distributional effect. Based on the empirical literature, there is some evidence that the depreciation rate of health capital increased in the post-communist states because of higher consumption of alcohol and tobacco products, especially during the period of transition. Thus, the negative behavioral effect imposes an increase in the cost of health capital, negatively affecting the population’s health. This response is depicted in the left-hand panel of Fig. 2. At the same time, if democratic institutions force ruling officials to increase public investment in the population’s health, this triggers the positive distributional effect, and population health may improve overall, as shown in the right-hand panel of Fig. 2. Ascertaining which effect actually prevailed in the post-communist countries is the major empirical objective of this study.
-
b.
Empirical Models and Data
Our first research question is whether there were any changes in health outcomes in the period of transition in the post-communist states relative to the consolidated democracies. We address this question by using the conventional difference-in-difference framework as in (1). In Table 1, we list the countries included in the control group (consolidated democracies).Footnote 3
$${Y}_{it}={\theta }_{1}{T}_{1985-1989}+{\theta }_{2}{P}_{1990-1994}+{\theta }_{3}{P}_{1995-1999}+{\theta }_{4}{P}_{2000-2004}+{\theta }_{5}{P}_{2005-2009}+{\theta }_{6}{P}_{2010-2014}+{X}_{it}{\beta }_{1}{+I}_{i}{\beta }_{2}{+G}_{i}{\beta }_{3}+\tau +\mu +{\varepsilon }_{it}$$(1)

Relationship between health and spending for health care and health depreciation

Changes in Health due to changes in spending for health care and health depreciation
In the above model, \({\theta }_{1}-{\theta }_{6}\) measures the differences in population health, \({Y}_{it}\)Footnote 4, in the post-communist states relative to the consolidated democracies in five-year time intervals. \({\theta }_{1}\) measures the difference in the five-year period prior to the start of transition, 1990; while \({\theta }_{2}-{\theta }_{6}\) measures the differences in the subsequent five periods of transition. We anticipate that in the period of transition, population health deteriorated in the post-communist states; thus, \({\theta }_{2}-{\theta }_{5}\) are negative for life expectancy and positive for the infant mortality rate. In the model, we also control for a rich set of factors that may have direct implications for population health before transition and along the transition path. The vector \({X}_{it}\) captures socio-economic differences and includes GDP per capita, its squared term, and average years of education. \({I}_{i}\) includes the institutional differences across countries represented by the percentage of Catholics, an indicator of Christian majority and the ethnic factorization index. \({G}_{i}\) comprises geographic controls, such as how landlocked the country is and distance to the equator and Greenwich. \({\mu }\) and \({\tau }\) are the post-communist and year fixed effects.
Our second research question is whether democracy has a positive impact on population health in the post-communist countries, we answer using the multivariate regression approach. Several studies have used the democracy stock to assess how democracy relates to population health (Wigley & Akkoyunlu-Wigley, 2011; Besley and Kudamatsu 2006). The left-hand side of the Eq. (2) demonstrates that the health outcome in the final year, 2014, is a function of the level of democratization in each year starting from the year of transition. Assuming an additive impact of democracy, \(\sum_{t=1}^{25}{D}_{it}=D{S}_{i}\) is the cumulative stock of democracy for the first 25 years of the transition. The parameter \(\gamma\) is negative for life expectancy and positive for the infant mortality rate and measures a long-run impact of democratization on population health.
To compute the democracy stock, we follow Wigley and Akkoyunlu-Wigley (2011) and Besley and Kudamatsu (2006). There are two major differences in our approach. First, our democracy stock is computed from the start of the transition to capitalism—1990—instead of 1960, the period of decolonization. Second, we use the sub-element of the Polity 2 democracy index, the institutionalized democracy score, ignoring the institutionalized autocracy score. A correlational analysis shows that the Polity 2 index and its sub-element, the institutionalized democracy score, are highly correlated. Since our main interest is to quantify the association with democratization, basing the democracy stock solely on the institutionalized democracy score, and ignoring the autocracy score, should be a more effective measure of to what extent the state’s political system is exposed to widely recognized democratic institutions. Figure 3 demonstrates the existence of a substantial variation in the democracy stock across the post-communist countries in the first 25 years of transition.Footnote 5

Democracy stock in 2014

Post-communist states vs. consolidated democraces, 1970–2014

Democracy stock and population health (post-communist states, 2014)
To understand the possible mechanisms for the relationship between democracy and population health, we use the same empirical approach as in Eq. (2), with the only difference that the dependent variable is either represented by behavioral variables, such as alcohol consumption per capita, smoking prevalence among males, suicide mortality rate per 100,000, and births per 1,000 women aged 15–19, or distributional factors, such as health expenditure per capita, number of physicians, and number of beds per 1,000. A positive association of the democracy stock with any behavioral factor would imply an increased participation in risky activities during the period of transition. A similar association with any distributional factor would imply improved public financing of health care. Such an analysis.
Table 2 provides summary information about the sources used to construct the country-level panels for the countries included in both samples. Table 3 gives the descriptive statistics for the sample used to run the difference-in-difference analysis. The key variables are given separately for the 29 post-communist states and 20 consolidated democracies. Income per capita in the post-communist states is $9,500, which is less than five times that in the consolidated democracies. The citizens of the consolidated democracies are only slightly more educated, 6.89 years vs. 6.6 years, have a higher representation of Catholics, 38 vs. 18%, a higher likelihood of Christian majority, 95 vs 62%, are less likely to live in a landlocked state, 15 vs. 45%, or in a state with a lower likelihood that two randomly selected citizens represent different ethnical groups, 24 vs. 45%. The distance to the equator is comparable between the two types of countries, 5,290 vs. 5,160 km. This descriptive analysis shows that the two groups of countries differ substantially with respect to socio-economic, institutional, and geographic characteristics, and any statistical analysis should be adjusted for these differences, as proposed in models (1) and (2).
Table 3 also demonstrates that the consolidated democracies spend more on health care, $4,953 vs $610, and have slightly more physicians per 1,000 citizens, 3.41 vs. 2.86. However, the post-communist states provide more hospital beds per 1,000 citizens, 5.65 vs. 4.10. These numbers suggest that the consolidated democracies may place a higher emphasis on diagnostics and preventive care, while in the post-communist states a greater emphasis is given to in-patient care.
Table 3 also reveals that the citizens of the post-communist states are more likely to be engaged in risky activities. For example, in the post-communist states there is a substantially higher male smoking rate, 45 vs 30%, suicide mortality rate, 16 vs. 12 deaths per 1,000 citizens, and fertility rate among adolescents, 24 vs. 11 births among 1,000 girls aged 15–19. The only figure that is higher in the consolidated democracies is the consumption of alcohol per capita, 9.2 vs. 8 L per year.
In Figure 4, we visualize the averages with the 95 confidence intervals for population health measures for the post-communist states and the consolidated democracies. In the early 1970s, the citizens of the consolidated democracies lived more than four years longer than their counterparts in the post-communist states. At the time of transition, the gap increased to seven years, and the gap remained the same during the whole period of transition. For example, in 2014, the average citizen of the consolidated democracies lived more than 81 years, while the counterpart citizen of the post-communist states lived only 74 years. With respect to infant mortality, the gap in infant mortality was tremendous, about 35.9 deaths per 1,000 newborns in the early years. This gap declined to 21.8 deaths at the time of transition, and during the transition period, the gap further shrank to 7.4 deaths. The above analysis suggests that the transition may have been detrimental for life expectancy but infant mortality on average may have improved in the post-communist states.
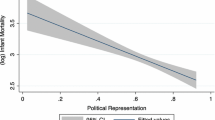
Figure 5, show that the population health measures correlate with the democracy stock. The democratic states experience a longer life expectancy than states with consolidated autocratic regimes. The difference in life expectancy between the newly consolidated democracies and persistently autocratic states is six years. We observe a similar trend for the alternative measure of public health, infant mortality. The consolidated autocratic regimes have almost 20 more deaths per 1,000 births than the newly established consolidated democracies.
4 Analysis and Main Findings
In Figure 6, we report estimates of the first empirical model.Footnote 6 The figure shows that a substantial one-year difference in life expectancy between the two groups existed in the five years before the collapse of the Eastern Bloc. However, the difference reached two years at the time of transition, and peaked at 2.5 years in the period between 1996 and 1999. After 1999, we observe a slight decline in the difference in life expectancy between the two types of state, albeit the improvements were in the post-communist states; but in the final period between 2010 and 2014, the difference in life expectancy was still above that of the pre-transition period. Thus, relative to the consolidated democracies, we observe a substantial deterioration in population health in the post-communist states, although there is a clear sign of improvement in the later period of transition.

Coefficients, \({\theta }_{1}-{\theta }_{6}\), from the difference-in-difference analysis
With respect to infant mortality, the pre-transition difference between the two types of countries is negligible. Similar to life expectancy, in the first 10 years of transition, we observe a substantial deterioration in infant mortality in the post-communist states relative to the consolidated democracies. Although the estimates lack statistical significance, the economic significance of the estimates for the first 10 years of transition is apparent. Infant mortality rose by four deaths per 1,000 births in the post-communist states. The good news is that the difference in infant mortality disappeared along the transition path, and in the last five years of the sample the difference favors the post-communist states, by four deaths per 1,000 births.
Thus, based on these results, we can state that in the period of transition, the post-communist states relative to their counterfactual states experienced a significant drop in life expectancy and an increase in infant mortality. Even though in the later periods of the transition life expectancy improved in the post-communist states, even after more than 20 years of transition, the gap has not been restored to the pre-transition levels. With respect to infant mortality, in the last period, 2010–2014, infant mortality improved in the post-communist states relative to the counterpart states.
In Table 4, we accept the hypothesis that the democracy stock is positively associated with life expectancy in the post-communist states. A one standard deviation increase in the stock (86 points) increases life expectancy by 1.634 years—or, if this estimate is translated into the elasticity term, a 10% increase in the democracy stock increases life expectancy by 0.31%. Enriching the model with the additional controls reduces the magnitude of the main coefficient, although its statistical significance is always within the 10% level. In the final specification, a 10% increase in the democracy stock increases life expectancy by 0.19%.
Table 5 supports the hypothesis that the democracy stock is reversely related to infant mortality. In the most parsimonious specification, a one standard deviation increase in the stock reduces infant mortality by 6.62 deaths per 1,000 births. Translating this into the elasticity term, a 1% increase in the democracy stock reduces infant mortality by 0.94%. The association is almost unit elastic,Footnote 7 and can be classified as a quite sensitive association. Adding other controls substantially reduces the magnitude of this estimate. In the final specification, with the full set of controls, the estimate drops to 3.7 deaths per 1,000 births for a one standard deviation increase in the democracy stock. If we translate this into the elasticity term, a 1% increase in the democracy stock reduces infant mortality by 0.53%.
Following studies on post-communist historical legacies (Pop-Eleches & Tucker, 2017), of the entire set of control variables, the most significant associations with life expectancy are found for the average educational attainment and the percentage of the population represented by Catholics (See Table 4). One additional year of education increases life expectancy by 1.083 years. For example, Mongolia has the lowest educational attainment in 1970, at 3.56 years, with life expectancy at only 69 years in 2014, this is the second lowest life expectancy after Turkmenistan, 67 years, in the same year. If the average educational attainment in Mongolia was 9.56 years, comparable with the Czech Republic, life expectancy could be 76.2 years, close to the life expectancy in the majority of developed nations.
The results also show that a one percentage point increase in the Catholic population increases life expectancy by 0.024 years. Poland and Croatia have the largest representation of Catholics among the post-communist republics, at 87%. This result implies that the Catholic population contributes 2.08 years to the observed difference in life expectancy between these two countries and the countries with no Catholic population.
The association between the landlocked indicator and life expectancy reveals that the landlocked states have lower life expectancy, on average, by slightly more than 2.5 years. This association most likely captures the low life expectancy in the landlocked Central Asian republics, such as Kazakhstan, Kyrgyzstan, Tajikistan, Turkmenistan, and Uzbekistan, rather than in the Eastern European landlocked nations, such as the Czech Republic and the Slovak Republic.
Another important association is between income per capita and life expectancy. A higher living standard increases life expectancy indirectly through higher education, and directly through better nutritional intakes and access to better health care services. The results of our analysis confirm that an increase in the living standard increases life expectancy. This positive association holds until the average income reaches $26,500 per year. Beyond this threshold, a further increase in income per capita depresses the life expectancy.
There are many factors that explain the variations in infant mortality for the post-communist states (See Table 5). A unit increase in the educational attainment reduces the number of deaths among 1,000 newborn children by 2.8 babies. For example, Tajikistan experienced one of the largest likelihoods of infant mortality among the transition societies, 39 deaths per 1,000 births, with average educational attainment in 1970 of 6.6 years. An increase in the educational attainment by two years could reduce this likelihood by more than half a percentage point, or 5.6 infants per 1,000 newborns.
Table 5 also shows that income has a negative association with infant mortality before $10,511 per capita, which is close to the level of the average post-communist state in 2014. There would be a marginal change for the poorest country, Tajikistan, with a substantial increase in the living standard. From a doubled income per capita, Tajikistan would achieve a reduction in infant mortality of only 0.8 deaths for 1,000 newborns.
Table 5 demonstrates that ethnic fractalization, which is the likelihood of two randomly chosen individuals in a society being representatives of two different ethnic groups, has a negative association with infant mortality. A 10-percentage point increase in the given likelihood reduces infant mortality by 1.4 deaths per 1,000 infants. For example, Armenia has one of the most homogenous populations, with only a 12.7% likelihood of ethnic fractalization, and, at the same time, it has above-average infant mortality, at 13 deaths for 1,000 newborns. Based on our results, an increase in ethnic diversity in Armenia by 10 percentage points would reduce infant mortality by 10%.
Table 5 confirms that the landlocked countries experience worse outcomes as regards the infant survival rate in the first years of their life. On average, infant mortality in the landlocked countries is 5.5 deaths per 1,000 newborns more than in the counterpart countries. This result is mainly driven by massive infant mortality in such landlocked countries as Uzbekistan (24.5 deaths per 1,000 newborns), Azerbaijan (29.1 deaths), Tajikistan (39.5 deaths), and Turkmenistan (46.1 deaths). In comparison, in the non-landlocked countries, the infant mortality ranges from 2 to 14.1 deaths per 1,000 newborns, with the lowest in Slovenia and the highest in Moldova.
Table 6 demonstrates that a one-standard-deviation increase in the democracy stock increased health care expenditure per capita by $45. The numbers of beds and physicians per 1,000 individuals were also positively impacted by democratization, although to a lesser extent. This finding explains the improvement of health and democracy simultaneously (for those states that passed through democratization) and supports the distributional effect hypothesis.
Table 7 provides mixed results for the behavioral effect hypothesis. On the one hand, a one-standard-deviation increase in the democracy stock increases the suicide mortality rate by 3.2% points and increases the annual consumption of alcohol by 1.4 L per capita. These results probably refute the behavioral effect hypothesis. On the other hand, the fertility rate among teenagers and young women of ages 15–19 decreases by 1.16 births per 1,000 adolescents, with a similar change in the stock, supporting the hypothesis.
5 Discussion
To understand the results better, we consider two causal mechanisms—distribution effect (reflecting governmental policy choices to spend on public health, to improve medical care and access to it), and, somewhat less studied, the behavioral mechanism (reflecting individual choices with regard to lifestyle, such overconsumption of alcohol, tobacco, pregnancy among teenagers, and suicide rate). While the latter set of factors have been considered in studies in medicine and psychology, they have not been analyzed within political regime transition studies.
Regarding the redistribution effect, we find that consolidated democracy improves the quality of, and access to, health care. This explains the positive association between democracy and population health over time and in the long run. The results reported in Table 6 partially support this hypothesis, suggesting that the introduction of democratic institutions in the post-communist states may have triggered a distribution effect, increasing spending on health care and consequently improving population health. In contrast, for the states with consolidated autocratic regimes, one reason why they may experience inferior outcomes for population health may be a lack of resources devoted to population health.
Previous studies also point out that the populations of non-democracies do not search for medical care even if they need it, mainly because it is not affordable (Balabanova et al., 2012) but also because of low trust to medical personal (along with general lower social and institution trust—trust to people and to services). The later was argued to be one of the pronounced historical legacies of Communism, among many others (Pop-Eleches & Tucker, 2017; Beissinger & Kotkin 2014; Lankina et. al 2016b; Libman & Obydenkova, 2015, 2020) The same group of people exhibit risky behavior, thus reducing their life expectancy. Balabanova et. al (2012), for example, discovered, that people from such transition states as Armenia, Georgia, and Ukraine are significantly less likely to seek medical care, especially those living in rural areas and within age group of 35–49. The post-Soviet non-democratic states contrast with the more successful achievers among the post-communist states in Central Europe (currently the European Union (EU) members and democracies).Footnote 8 Indeed, the impact of the EU has been significant for transformation not only for political processes (associated with promotion of democracy, human rights, protection of environmental among others), but also for socio-cultural behavior and perceptions across and beyond the future member-state (e.g. Pop-Eleches & Tucker, 2017; Lankina et. al 2016b; Obydenkova, 2012; Levitsky and Way 2010). These studies demonstrated transformative power of the EU in terms of value diffusion and democracy promotion across the post-Communist Eurasia. However, the opposite impact of the autocracies-driven external factors can be associated with consolidation of non-democratic values and ideology (Izotov & Obydenkova, 2021) resulting in sustaining lack of transparency and information.Footnote 9
In terms of behavioral effect, an alternative mechanism that may explain the relationship between transition and population health is propensity toward public participation in risky behavior after the initial period of transition. By risky behavior we mean consumption of alcohol and tobacco, suicide, dietary choices, and unwanted pregnancy among teenage women. As discussed in the second section, the relationship between democracy and these behavioral choices may go in different directions. On the one hand, transition from a totalitarian state and control to a market economy makes certain goods more available (e.g., drugs and tobacco become more available to population). Transition is also associated with radical socio-economic and political-ideological changes (e.g., loss of ideology) that may trigger stress and suicide in the short run, and an increase in the consumption of alcohol. The results reported in Table 7 provide mixed support for this hypothesis.
Life expectancy is determined not only by governmental public policy expenditure but also by individuals’ choices and lifestyles, as discussed above (e.g., personal choices in diet, and consumption of alcohol and tobacco, and deciding to commit suicide) and by issues over which the public has no choice (such as pollution, stress, economic poverty, and increased inequality). While we cannot consider all of these factors within one paper, it is still highly important to highlight that life expectancy is only partially explained through the quality of, and access to, medical care, while a significant portion is explained through public behavior and individual choices affecting health. Our results in terms of life expectancy confirm previous findings that this variable “dropped steeply in the 1990s, and several countries have yet to recover the levels noted before the dissolution of the Soviet Union” (Bernd et al., 2013, p. 1145). Moreover, studies looking into specific diseases specify the importance of cardiovascular disease as one of the main challenges in post-communist regions, due to high alcohol consumption and smoking, in addition to other factors (Ibid.).
In contrast, when it comes to infant mortality, the determinates of this are mainly related (if not exclusively) to the quality of, and access to, medical care. To a lesser degree, infant mortality can be related to the individual choices of pregnant women (though this is at odds with studies in psychology and medicine that argue in favor of the predominance of healthy life choices among pregnant women).
Therefore, though life expectancy and infant mortality are determined by both governmental spending and individual choices, their significance varies across these two indicators of health. In contrast to life expectancy, infant mortality is mainly caused by the actual quality of medical care (poor level of doctors or hospitals or hygiene; access to medical care; lack of trust in doctors; insufficient number of hospitals and medical personal, among others). Our finding of a decline in infant mortality over the regime transition signals an improvement in governmental spending on public health. Yet this latter finding is only applicable for cases of democratization (where regime transition involves a gradual increase in the level of democracy). Nevertheless, in cases where the transition resulted in the consolidation of different shades of non-democratic regimes (autocracies or hybrids), infant mortality declined there too.
In the political science literature, there are many alternative measures of democracy available such as Democracy Barometer (developed by the Berlin Social Science Center and Center for Democracy Studies Arau) or Freedom House’s democracy index. Our analysis shows that the correlation between the Polity 2 index and Freedom House’s democracy index for the study period is 0.90. Based on the high correlation, we can assume the high external validity of the measure used in this study and its significant overlap with the alternative measures of democracy.
6 Conclusion
Can it be that for the post-communist states, the relationship between democracy and health is reversed because of an adverse experience of transitioning? Can it be that the true relationship is hidden because of differences in democratization across the post-communist states? While some decline in public expenditure, and—associated with it—some decline in public health, can be expected over the transition period, how long does it remain? The so-called fourth wave of transition took place at least 30 years ago (in the end of the 1980s and the beginning of the 1990s). Since the 1990s, political institutions and regimes have been consolidated over the post-communist space in Eurasia. In contrast to previous studies, this paper aimed to answer these questions by looking at the consequences of already consolidated political regimes for public health, taking into account two very different causal mechanisms (governmental policy versus public behavior) and employing two different measures of health (life expectancy versus infant mortality). Based on the difference-in-difference analysis, we conclude that the post-communist states, relative to their counterfactual states, experienced a significant drop in life expectancy and some increase in infant mortality in the short run during the transition period. Thus, the transition in the short run was accompanied with a deterioration in public health in the period of approximately 1990 to 1995. Yet both aspects of public health improved significantly and radically after the consolidation of democracy. It is highly important for our study to note that life expectancy and child mortality still exhibit a somewhat different trajectory, with the latter almost reaching the level of the consolidated Western democracies. In contrast, life expectancy, reflecting the experience under communism and the psychological pressure triggered by the transition, which resulted in high-risk behavior of the adult population, improved more slowly as compared to child mortality. As discussed, we argue that to have a complete picture of the impact of the transition on public health it is important to consider two “sides of the coin”. Child mortality is mainly explained through quality of health care (access to hospitals; quality and education of medical personal; sufficient number of doctors and beds in hospitals; number of hospitals, etc.)—these factors are highly dependent on governmental spending). Some studies have challenged the assumption that life expectancy, death and massive suicide were caused by alcohol consumption. Bhattacharya et al., (2013), for example, argued that post-Communist transition per se should not be hold responsible for "Russia's 40 percent surge in deaths between 1990 and 1994″. Instead, they suggest that mortality was triggered by the 1980s Michael Gorbachev famous Anti-Alcohol Campaign. For other post-Communist states, the explanation may point to similar poor decisions of centralized political and economic state management that was still in place in the end of the 1980s and very onset of the 1990s. It was also determined by the behavior, style of life conditioned by availability of consumption productions, that is, by their behavior, and by quality of life in general degenerated by communism and/or transition (e.g., e.g., a poor diet and the absence of sport and other recreational activities, an increase in the consumption of alcohol and tobacco, on the one hand; and, on the other hand, psychological factors that were triggered by transition, such as stress, depression, and an increase in suicide rates, to name a few). Needless to say, life expectancy also depends on the access to, and quality of, medical care, but in contrast to child mortality, where medical care is the most important factor, life expectancy is also the result of a number of other factors reflecting the life choices and behavior of adult population. Therefore, accounting for both measures of health allows for a better understanding of the effects of transition and democratization on public health, and the different causal mechanisms involved in this nexus.
Another important finding is that the democracy stock analysis demonstrates that in the long run, democratization has had a positive impact on both life expectancy and infant mortality in the post-communist states. Although there is some evidence of negative behavioral effects, such as an increase in the suicide mortality rate and the consumption of alcohol, there is also evidence of positive behavioral effects, such as a reduction in fertility among teenager women. The strong persistent positive distributional effect in the form of higher health care spending per capita reveals that democracy has a positive impact on a population’s health. This issue as well as psychological implications of regime transition have to stay on the agenda for further investigation. Moreover, it is also possible to conjecture that different types of welfare states and employment regimes established and consolidated by the end of the regime transition may also influence public health (e.g., Eivind Kolberg and Esping-Andersen., 2019; Esping-Andersen 2019). Based on these recent studies, it is possible that reduction in social inequality (associated with social democracy) will be more beneficial for accessibility and quality of medical care (e.g., Esping-Andersen, 2019). In contrast, the liberal type of welfare state would provide only very basic medical public care and could thus be less successful in terms of life expectancy and infant mortality.Footnote 10 However, this should remain on the agenda for future research. The post-communist countries present a very special case-study due to their profound historical legacies of Communism and, associated with this, ideological and behavioral components (Pop-Eleches and Tucker 2016; Beissinger & Kotkin 2014; Lankina et. al. 2016b). In addition to different types of welfare state, political party systems, the nature of market, a number of other explanatory factors listed above could help to develop further a more nuanced approach to the nexus of political regime transition and public health. These issues should stay on the agenda for future studies and research of post-Communist societies and transitional economies.
Notes
The authors of this paper are listed alphabetically, and they contributed equally to this manuscript. Anastassia Obydenkova’s research was supported by the Basic Research Program of the National Research University Higher School of Economics (HSE University) and by the Fung Global Fund, Princeton Institute for International and Regional Studies, Princeton University (USA).
The major requirement to be part of this group is having a nearly perfect democracy in 1990 based on the Polity IV project’s Polity 2 index. The states that satisfy this requirement are mostly located either on the European or North American continents.
The subscript \(i\) represents one of the 49 countries in the sample, and the subscript \(t\) represents one of the 45 years from 1970 to 2014.
At the end of this timeframe, several countries, such as Hungary, Lithuania, Slovenia, the Czech Republic, Mongolia, Poland, and the Slovak Republic, had become newly established consolidated democracies, with the full set of democratic characteristics. Several countries, such as Turkmenistan, Bosnia, Uzbekistan, Kazakhstan, Azerbaijan, Tajikistan, Belarus, and Kyrgyzstan remained either completely undemocratic or with limited exposure to democratic institutions.
In Fig. 6, we depict the coefficients, $${\theta }_{1}-{\theta }_{6}$$, from the difference-in-difference regression (1). In this analysis, each period lasts five years. Thus, a single point in the figure represents the difference in the health outcome at a specific period, along with a 95% confidence interval surrounding this difference. The red line identifies the start of transition.
A 1% change in the independent variable leads to a 1% change in the dependent variable.
Indeed, states’ membership in international organizations such as multilateral development banks, for example, can be potentially a strong contributing factor to changes in international strategies of state-actors and at national level and so far it has received somewhat limited attention (e.g., Ben-Artzi 2016, Obydenkova and Rodrigues Vieira 2020). However, investigation of this issue and its implications for public health is beyond the scope of this paper at this stage but should stay on the agenda for further studies.
The later factors (misinformation and lack of trust to institutions and politicians) are especially relevant within the global health crisis and pandemic. Misinformation of the population potentially could have triggered counter-productive public behavior (e.g., radical decrease in basic safety measured required within the Pandemic).
Japan could be an interesting example, yet, admittedly, outside of the post-Communist region. Japan has one of the highest in the world life expectancy but also one of the highest level in quality of democracy and the welfare state. Potential studies could investigate this nexus at the global level beyond post-Communist Eastern European and Central Asian states, as this study did.
References
Akhmedov, A., & Zhuravskaya, E. (2004). Opportunistic political cycles: Test in a young democracy setting. Quarterly Journal of Economics, 119(4), 1301–1338.
Alesina, A., Devleeschauwer, A., Easterly, W., Kurlat, S., & Wacziarg, R. (2003). Fractionalization. Journal of Economic Growth, 8, 155–194.
Anderson, C. (1998). When in doubt, use proxies: Attitudes toward domestic politics and support for European integration. Comparative Political Studies, 31(5), 569–601.
Anderson, C., & Tverdova, Y. (2003). Corruption, political allegiances, and attitudes toward government in contemporary democracies. American Journal of Political Science, 47(1), 91–109.
Armingeon, K., & Guthmann, K. (2014). Democracy in crisis? The declining support for national democracy in European countries, 2007–2011. European Journal of Political Research, 53(3), 423–442.
Arpino, B., & Obydenkova, A. (2020). Democracy and political trust before and after the great recession 2008: The European Union and the United Nations. Social Indicators Research, 148(2), 395–415. https://doi.org/10.1007/s11205-019-02204-x
Baum, M. A., & Lake, D. A. (2003). The political economy of growth: Democracy and human capital. American Journal of Political Science, 47(2), 333–347.
Balabanova, D., Roberts, B., Richardson, E., Haerpfer, C., & McKee, M. (2012). Health care reform in the former Soviet Union: Beyond the transition. Health Services Research, 47(2), 840–864.
Balestra, C., Boarini, R., & Tosetto, E. (2018). What matters most to people? Evidence from the OECD better life index users’ responses. Social Indicators Research, 136, 907–930.
Ben-Artzi, R. (2016). Regional development banks in comparison: Banking strategies versus development goals. Cambridge University Press.
Bhattacharya, J., Gathmann, C., & Miller, G. (2013). The gorbachev anti-alcohol campaign and Russia’s mortality crisis. American Economic Journal: Applied Economics, 5(2), 232–260.
Barro, R., & Lee, J. W. (2013). A new data set of educational attainment in the world, 1950–2010. Journal of Development Economics, 104, 184–198.
Bartel, J., Birch, S., & Skirmuntt, M. (2017). The local roots of the participation gap: Inequality and voter turnout. Electoral Studies, 48, 30–44. https://doi.org/10.1016/j.electstud.2017.05.004
Beissinger, M., & Kotkin, S. eds. (2014). Historical legacies of communism in Russia and Eastern Europe. Cambridge University Press.
Besley, T., & Kudamastu, M. (2006). Health and democracy. American Economic Review, 96(2), 313–318.
Brewer, P. R. Kimberly Gross, Sean Aday and Lars Willnat (2004). International trust and public opinion about world affairs. American Journal of Political Science, 48(1), 93–109.
Brown, J. D., Earle, J. S., & Gehlbach, S. G. (2009). Helping hand or grabbing hand? State bureaucracy and privatization effectiveness. American Political Science Review, 103(2), 264–283.
Denisova, I. & Shapiro, J. (2013). Recent demographic developments in the russian federation. In: Alexeev M. and Weber, S., (Eds.) The Oxford handbook of the Russian Economy. Oxford University Press.
Danilova, I., Shkolnikov, V. M., Jdanov, D. A., Meslé, F., & Vallin, J. (2016). Identifying Potential differences in cause-of-death coding practices across Russian Regions. Population Health Metrics, 14(8), 1–20.
Durand, M. (2015). The OECD better life initiative: How’s life? And the measurement of well-Being. The Review of Income and Wealth, 61(1), 4–17.
Eivind Kolberg, J., & Gøsta, E. A. (2019). Welfare states and employment regimes. In: Jon Eivind, K. (Ed.) The Study of welfare state regimes. Routledge, pp. 3–36.
Esping-Andersen, G. (2019). 1. Single-party dominance in Sweden: The Saga of Social Democracy. In: Pempel T. J. (Ed.) Uncommon Democracies. Cornell University Press, pp. 33-57. https://doi.org/10.7591/9781501746161-004.
Esping-Andersen, G. (2018). 4. The three political economies of the welfare state.In: O’Connor, J. S., Olsen, G. M., (Eds.) Power Resource Theory and the Welfare State. University of Toronto Press, 2018, pp. 123–153. https://doi.org/10.3138/9781442678675-008.
Franco, A., Alvarez-Dardet, C., & Ruiz, M. (2004). Effect of democracy on health: Ecological study. BMJ, 329, 1421–1423.
Gerring, J., Thacker, S., & Alfaro, R. (2012). Democracy and human development. The Journal of Politics, 74(1), 1–17.
Ghobarah, H. A., Huth, P., & Russett, B. (2004). Comparative public health: The political economy of human misery and well-being. International Studies Quarterly, 48(1), 73–94.
Hobolt, S. (2012). Citizen satisfaction with democracy in the European Union. Journal of Common Market Studies, 50(s1), 88–105.
Izotov, V. S., & Obydenkova, A. V. (2021). Geopolitical games in Eurasian regionalism: Ideational interactions and regional international organisations. Post-Communist Economies, 33(2–3), 150–174. https://doi.org/10.1080/14631377.2020.1793584
Keefer, P. (2007). Clientelism, credibility, and the policy choices of young democracies. American Journal of Political Science, 51(4), 804–821.
Keiding, H. (2018). Theoretical health economic. World Scientific Publishing Co. Pte. Ltd.
Lankina, T., Libman, A. & Obydenkova, A. (2016a). Authoritarian and democratic diffusion in post-Soviet regions. Comparative Political Studies 49: 12, 1599–629. https://doi.org/10.1177/0010414016628270.
Lankina, T., Libman, A., & Obydenkova, A. (2016b). Appropriation and subversion: Pre-communist literacy, communist party saturation, post-Soviet democratic outcomes. World Politics, 68(2), 229–274. https://doi.org/10.1017/S0043887115000428.
Levitsky, S., & Way, L. (2010). Competitive Authoritarianism: Hybrid Regimes after the Cold War. Cambridge University Press.
Libman, A., & Obydenkova, A. (2013a). Communism or communists? Soviet legacies and corruption in transition economies. Economic Letters, 119(1), 101–103. https://doi.org/10.1016/j.econlet.2013.02.003.
Libman, A., & Obydenkova A. (2013b). Informal governance and participation in non-democratic international organizations. Review of International Organizations, 8, 221–243 (2013). https://doi.org/10.1007/s11558-012-9160-y.
Libman, A., & Obydenkova, A. V. (2020). Proletarian Internationalism in Action? Communist Legacies and Attitudes towards Migrants in Russia. Problems of Post-Communism, 67(4–5), 402–416. https://doi.org/10.1080/10758216.2019.1640068.
Libman, A., & Obydenkova, A. (2014). The Governance of commons in a large nondemocratic state: The case of forestry in the Russian federation. Publius: The Journal of Federalism, 44(2), 298–323. https://doi.org/10.1093/publius/pjt065.
Libman, A., & Obydenkova, A. (2019). Inequality and historical legacies: Evidence from post-communist regions. Post-Communist Economies, 31(6), 699–724. https://doi.org/10.1080/14631377.2019.1607440.
Libman, A., & Obydenkova, A. (2015) CPSU legacies and regional democracy in contemporary Russia, special issue: Governance, Trust and Democracy, Political Studies, 63(“S1”), 173–190. https://doi.org/10.1111/1467-9248.12133.
Libman, A., & Obydenkova, A. V., (2018a). Understanding authoritarian regionalism. Journal of Democracy, Volume 29 (Issue 4), pp. 151–165. https://www.journalofdemocracy.org/article/understanding-authoritarian-regionalism.
Libman, A., and Obydenkova, A. V., (2018b). Regional international organizations as a strategy of autocracy: The Eurasian economic union and Russian foreign policy. International Affairs, 94 (5), 1037–1058. https://doi.org/10.1093/ia/iiy147.
Mackenbach, J., Hu, Y., & Looman, C. (2013a). Democratization and life expectancy in Europe, 1960–2008. Social Science and Medicine, 93, 166–175.
Mackenbach, J. P., Hu, Y., & Looman, C. W. N. (2013b). Democratization and life expectancy in Europe, 1960–2008. Social Science & Medicine, 93(18), 166–175.
Martel García, F. (2014). Democracy Is Good for the Poor: A Procedural Replication of Ross. Research and Politics, Nov. 2014. https://doi.org/10.1177/2053168014559094.
Mayne, Q., & Hakhverdian, A. (2017). Ideological congruence and citizen satisfaction: Evidence from 25 advanced democracies. Comparative Political Studies, 50(6), 822–849.
Milanovic, B. (1999). Explaining the increase in inequality during transition. Economics of Transition, 7(2), 299–341.
Mizobuchi, H. (2014). Measuring world better life frontier: A composite indicator for OECD better life index. Social Indicators Research, 118, 987–1007.
Mungiu-Pippidi, A. (2015). The quest for good governance: How societies develop control of corruption. Cambridge University Press.
Nazarov, Z., & Obydenkova, A. V. (2020). Democratization and firm innovation: Evidence from European and Central Asian post-communist states. Post-Communist Economies, 32(7), 833–859. Online first: https://doi.org/10.1080/14631377.2020.1745565.
Obydenkova, A. (2008). Regime transition in the regions of Russia: The freedom of mass media: Transnational impact on sub‐national democratization? European Journal of Political Research, 47(2), 221–246. https://doi.org/10.1111/j.1475-6765.2007.00727.x.
Obydenkova, A.(2012). Democratization at the grassroots: the European Union's External Impact. Democratization, 19(2), 230–257. https://doi.org/10.1080/13510347.2011.576851.
Obydenkova, A., & Arpino, B. (2018). Corruption and trust in the European Union and National Institutions: Changes over the great recession across European States. Journal of Common Market Studies, 56(3), 594–611. https://doi.org/10.1111/jcms.12646.
Obydenkova, A., & Libman, A. (2012). The impact of external factors on regime transition: Lessons from the Russian Regions. Post-Soviet Affairs, 28(3), 346–401. https://doi.org/10.2747/1060-586X.28.3.346.
Obydenkova, A., & Libman, A. (2015). The survival of post-communist corruption in contemporary Russia: The influence of historical legacies. Post-Soviet Affairs, 31(4), 304–338. https://doi.org/10.1080/1060586X.2014.931683.
Obydenkova, A., Nazarov, Z., & Salohodjaev, R. (2016). The process of deforestation in the weak democracies and the role of intelligence. Environmental Research, 148, 484–490. https://doi.org/10.1016/j.envres.2016.03.039.
Obydenkova, A. V., & Salahodjaev, R. (2016). Intelligence, democracy, and international environmental commitment. Environmental Research, 147, 82–88. https://doi.org/10.1016/j.envres.2016.01.042.
Obydenkova, A. V., & Salahodjaev, R. (2017). Climate change policies: The role of democracy and social cognitive capital. Environmental Research, 157, 182–189. https://doi.org/10.1016/j.envres.2017.05.009.
Obydenkova, A., & Swenden, W. (2013). Autocracy-sustaining versus democratic federalism: Explaining the divergent trajectories of territorial politics in Russia and Western Europe. Territory, Politics, Governance, 1(1), 86–112. https://doi.org/10.1080/21622671.2013.763733.
Obydenkova, A. V., & Rodrigues Vieria, V. G. (2020). The limits of collective financial Statecraft: Regional development banks and voting alignment with the united states at the united nations general assembly. International Studies Quarterly, 64(1), 13–25. https://doi.org/10.1093/isq/sqz080.
Newton, K. (2001). Trust, social capital, and democracy. International Political Science Review, 22(2), 201–214.
Pop-Eleches, G., & Tucker, J. (2017). Communism’s shadow: historical legacies and contemporary political attitudes. Princeton University Press.
Rechel, B., & McKee, M. (2009). Health reform in central and eastern Europe and the former Soviet Union. The Lancet., 374(9696), 1186–1195. https://doi.org/10.1016/S0140-6736(09)61334-9.
Rohrschneider, R. (2002). The democracy deficit and mass support for an EU-Wide government. American Journal of Political Science, 46(2), 463–475.
Ross, M. (2006). Is democracy good for the poor? American Journal of Political Science, 50(4), 860–874.
Rosenberg, D., Kozlov, V., & Libman, A. (2018). Political regimes, income and health: Evidence from sub-national comparative method. Social Science Research, 72, 20–37. https://doi.org/10.1016/j.ssresearch.2018.02.001.
Shandra, J. M., Nobles, J., London, B., & Williamson, J. B. (2004). Dependency, democracy, and infant mortality: A quantitative, cross-national analysis of less developed countries. Social Science & Medicine, 59(2), 321–333.
Scheiring, Gabor, Bryant P. H. Hui, Darja Irdam, Aytalina Azarova, Eva Fodor, David Stuckler, Gosta Esping-Andersen, and Lawrence King (2020) “Privatization and the postsocialist fertility decline” Political Economy Research Institute (PERI) WP Working papers series N 533, pp. 1–74. University of Massachusetts: Amherest.
Shishkin S. (2013) Russia’s Health Care System: Difficult Path of Reform. In: Alexeev M., & Weber, S., (Ed.) Oxford Handbook of the Russian Economy. Oxford University Press.
Stickley, A., Koyanagi, A., Koposov, R., Schwab-Stone, M., Ruchkin V. (2014). Loneliness and Health Risk behaviors among Russian and U.S. adolescents: A cross-sectional study, BMC Public Health, 14.
Stone, R. (2000). Stress: Invisible Hand in Eastern Europe’s Death Rates. Science, 288(5472), 1732–1733. https://doi.org/10.1126/science.288.5472.1732.
Uslaner, Eric M. (2017) The historical roots of corruption: Mass education, economic inequality, and state capacity. Cambridge University Press.
Uslaner, E. M. (Ed.). (2018). The Oxford handbook of social and political trust. Oxford University Press.
Van Erkel, P., & Van Der Meer, T. (2016). Macroeconomic performance, political trust and the great recession: A multilevel analysis of the effects of within-country fluctuations in the corruption and trust in the EU and National Institutions Macroeconomic Performance on Political Trust in 15 EU Countries, 1999–2011. European Journal of Political Research, 55, 177–197.
Walberg, P., McKee, M., Shkolnikov, V., Chenet, L., & Leon, D. A. (1998). Economic change, crime, and mortality crisis in Russia: Regional analysis. British Medical Journal, 317(7154), 312–318.
Wigley, S., & Akkoyunlu-Wigley, A. (2011). The Impact of Regime Type on Health: Does Redistribution Explain Everything? World Politics, 63(4), 647–677.
Wigley, S., & Akkoyunlu-Wigley, A. (2017). The Impact of Democracy and Media Freedom on Under-5 Mortality, 1961–2011. Social Science and Medicine, 190, 237–246.
Acknowledgements
The paper was presented in a number of guest-speaker events at New York University, Columbia University of New York, Universidad Autonoma de Barcelona, and at the Davis Center at Harvard University (Cambridge, US). The authors are very grateful to Ada Ferrer-i-Carbonell, Joshua Tucker, Elise Giuliano, Alexandra Vacroux and Rawi Abdelal for their feedbacks on this project. The authors are grateful to two anonymous reviewers of this paper for their excellent comments. Anastassia Obydenkova thanks the Basic Research Program of the National Research University Higher School of Economics (HSE University) and Fung Global Fund, Princeton Institute for International and Regional Studies, Princeton University, for supporting her research. The authors of this paper are listed alphabetically and they contributed equally to this project.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix

Rights and permissions
About this article

Cite this article
Nazarov, Z., Obydenkova, A. Public Health, Democracy, and Transition: Global Evidence and Post-Communism. Soc Indic Res 160, 261–285 (2022). https://doi.org/10.1007/s11205-021-02770-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11205-021-02770-z