
Abstract
Religion exerts a powerful influence on many people’s lives. We investigate how self-assessed religiosity affects self-assessed health in Europe. Our sample consists of individuals with a native father and an immigrant mother from another European country. This sample allows for a causal interpretation since we can use the religiosity of the mother’s birth country as an instrument for individual religiosity in the first stage of a 2SLS regression analysis, which is related, in the second stage, to the individual’s health assessment. We find that the more religious are substantially more likely to report bad health. Several robustness tests offer a strong confirmation of the negative relationship between self-assessed religiosity and self-assessed health. Notably, this negative relationship is concentrated among women. The analysis indicates that religious constraints on women’s autonomy can impair their health.
Similar content being viewed by others


Notes
To mention but a few: economic growth (Barro and McCleary 2003; Durlauf et al. 2012), trust (Johansson-Stenman et al. 2009; Berggren and Bjørnskov 2011), the size of the shadow economy (Schneider et al. 2015), criminality (Brauer et al. 2013), tolerance (Berggren et al. 2019), the work ethic (van Hoorn and Maseland 2013) and entrepreneurship (Wiseman and Young 2014).
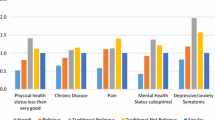
For examples of the diversity of the literature, see, e.g. Ellison and Levin (1998), Idler et al. (2003), Ellison and Hummer (2010), Hill and Cobb (2011) and Zimmer et al. (2019). Baker et al. (2018) identify a complex pattern between religious/secular identity and health outcomes in the United States. They find that “atheists report significantly fewer problems with physical health, mental health and pain than both nonaffiliated theists and some religious individuals” and that “[a]theism is the religious or secular identity with the healthiest outcomes on the basic psychiatric symptoms analyzed” (p. 53). Thus, while many affiliated theists benefit health-wise from their religiosity, atheists likewise seem to benefit from their (secular) identity, and sometimes even more so.
A key concern is reverse causality—e.g., a negative relationship between religiosity and health could reflect sick people seeking religious comfort and consolation (Ferraro and Kelley-Moore 2000).
We use the terms “self-assessed” religiosity and “self-assessed” health, since these are indicators from surveys based on people’s own assessments of how religious and how healthy they are. “Subjective” or “self-rated” are synonyms to “self-assessed”, used in other studies.
Nicholson et al. (2010: 233) point out that “… as this was a cross-sectional study, the potential for reverse causality is a major problem. … [R]everse causality is an important alternative explanation of our findings. These analyses could equally well be argued to show that poor health reduced attendance at religious services.”.
The data from these rounds are stacked. The first round does not include information on parental-birth country.
We also have data for Turkey and Israel, but to keep the sample more homogeneous, we do not include them in the main analysis. We have conducted all tests with them included, and there is no qualitative change in our findings (available upon request).
The individuals in our sample are similar to the general population in the countries in which they were born on observables, including self-reported health (Ljunge 2016).
The importance of the mother in transmitting cultural traits like religiosity has been shown to hold for social trust as well (Ljunge 2014a). Note that we cannot, due to a lack of data, differentiate between mothers who migrated to their present country of residence early and those who did so later in life.
In a robustness test, we code the replies from 1 (“very bad”) to 5 (“very good”) and conduct a linear regression analysis (see the Sect. 4.2).
In a robustness test, we also account for individuals’ overall life satisfaction in several ways, in order to capture cultural differences in attitudes to life, which could contribute to comparability of the subjective-health data.
The EVS/WVS variables are averaged for two reasons: Long-time averages are arguably better measures of persistent levels, and using many waves greatly increases the number of countries available.
We use the dataset compiled by Samanni et al. (2010). Using Gini data from The Standardized World Income Inequality Database yields similar results.
The IQ has been validated by Lynn and Meisenberg (2010) as a measure of cognitive ability.
For more information about this method, see pp. 2–3 of the supplementary material.
The standardized effect is computed as the estimate for religiosity times the standard deviation of religiosity as a fraction of the standard deviation of health.
The significant estimate on the tertiary education of the father is not a robust finding.
The correlation between self-assessed health and the objective health measure life expectancy in the mothers’ birth countries is 0.76, indicating that both measures capture an objective dimension of health.
There are also indications that cognitive skills are transmitted from parents to children (Coneus et al. 2012).
For example, Deaton (2011) remarks that time preference, captured by patience here, could affect both religiosity and health.
In addition, we have investigated whether effects differ depending on whether countries of residence are Catholic or not, and we do not find any statistically significant difference. Hence, it seems as if is religiosity as such, rather than belonging to a particular denomination, that is important.
Russia and Germany are the two largest ancestral groups. Scandinavians could be particularly secular, while Turkish ancestry could be particular since most are Muslims and Europe is overwhelmingly Christian. The Baltics are excluded since most immigrants have Russian ancestry.
There is not much variation in the kind of religion that dominate the mothers’ birth countries: Since they all stem from Europe, almost all are from nations characterized by Christianity. When checking, through sample restrictions, whether Protestant, Catholic or Orthodox Christianity display differential effects, we do not find any evidence that they do—it is the strength of the religious commitment or belief that matters.
This exercise also addresses concerns that people do not reply honestly to surveys about religiosity in very religious countries out of fear. Since our results hold when excluding the most religious countries, we consider it likely that the results are not driven by such behavior.
The result is similar when running the ordinary least squares model of column (3), Table 2, separately for women and men: strongly significant and positive estimate for women and close to zero and insignificant for men. We also tested the same model using the entire sample of the ESS (185,000 women and 159,000 men), and again found a positive estimate for how religiosity is related to bad health for women and a close-to-zero estimate for men. Results are available on request.
Due to the smaller samples when separating the genders, the first-stage results are estimated less precisely, which in turn makes it challenging to perform additional robustness checks in the gender subsamples. The point estimate on religious degree becomes higher for women and so does the standard error, resulting in a wide confidence interval for the true effect. The point estimate for men is close to zero with a standard error like the baseline specification, consistent with a zero true effect.
The theoretical idea, and the results, are also broadly consistent with studies that indicate that individuals with strong religious commitments are less likely than secular individuals to hold egalitarian gender-role attitudes (Diehl et al. 2009) and that more religious societies are less gender equal (Klingorová and Havlíček 2015; Schnabel 2016). Furthermore, it is certainly conceivable that factors that previous studies have shown can explain how religiosity affects health negatively could affect women more strongly than men, but we cannot test them with our data. For example, a negative effect of religiosity on health could result from religious people being less concerned with life on earth, including physical exercise (Feinstein et al. 2010; Kortt and Dollery 2014), being more “fatalistic” and not dealing with negative developments (Azaiza et al. 2010), having been subjected to bad treatment as children, e.g., corporal punishment, genital mutilation, sexual assault or no vaccination (Grogan-Kaylor and Otis 2007; Jegede 2007; Terry 2008; Gershoff 2010; Cappa et al. 2013) or being more mentally strained by internal or external conflicts (Exline 2002; Ellison and Lee 2010; Hill and Cobb 2011).
Still, it bears noting that for generalizability to make sense, one needs to have obtained an interpretable estimate, and we believe we have obtained an estimate that we can interpret as an effect of religiousness on health. This contrasts with much of the literature, as it does not address reverse causality, and for that reason, correlations obtained without an ability to rule out reverse causality cannot readily be generalized in a meaningful way. Hence, it can arguably be claimed that we are in a better position to offer generalizability even with an inclusion of mothers from another European country.
References
Ahrenfeldt, L. J., Möller, S., Andersen-Ranberg, K., Vitved, A. R., Lindahl-Jacobsen, R., & Hvidt, N. C. (2017). Religiousness and health in Europe. European Journal of Epidemiology, 32(10), 921–929.
Algan, Y., & Cahuc, P. (2010). Inherited trust and growth. American Economic Review, 100(5), 2060–2092.
Azaiza, F., Cohen, M., Awad, M., & Daoud, F. (2010). Factors associated with low screening for breast cancer in the Palestinian Authority: relations of availability, environmental barriers and cancer-related fatalism. Cancer, 116(19), 4646–4655.
Baker, J. O., Stroope, S., & Walker, M. H. (2018). Secularity, religiosity and health: physical and mental health differences between atheists, agnostics and nonaffiliated theists compared to religiously affiliated individuals. Social Science Research, 75(September), 44–57.
Barro, R. J., & McCleary, R. M. (2003). Religion and economic growth across countries. American Sociological Review, 68(5), 760–781.
Bengtson, V. L., Putney, N. M., & Harris, S. (2013). Families and faith: How religion is passed down across generations. Oxford: Oxford University Press.
Benjamins, M. R., Hummer, R. A., Eberstein, I. W., & Nam, C. B. (2004). Self-reported health and adult mortality risk: an analysis of cause-specific mortality. Social Science and Medicine, 59(6), 1297–1306.
Benyamini, Y. (2011). Why does self-rated health predict mortality? An update on current knowledge and a research agenda for psychologists. Pyschology and Health, 26(11), 1407–1413.
Berggren, N., & Bjørnskov, C. (2011). Is the importance of religion in daily life related to social trust? Cross-country and cross-state comparisons. Journal of Economic Behavior & Organization, 80(3), 459–480.
Berggren, N., Ljunge, M., & Nilsson, T. (2019). Roots of tolerance among second-generation immigrants. Journal of Institutional Economics, 15(6), 999–1016.
Bergh, A., Nilsson, T., & Waldenström, D. (2011). Sick from inequality?. Cheltenham: Edward Elgar.
Bettendorf, L., & Dijkgraaf, E. (2010). Religion and income: heterogeneity between countries. Journal of Economic Behavior & Organization, 74(1–2), 12–29.
Binder, M., & Coad, A. (2013). “I’m afraid I have bad news for you…”: Estimating the impact of different health impairments on subjective well-being. Social Science and Medicine, 87(June), 155–167.
Bisin, A., & Verdier, T. (2000). “Beyond the melting pot”: cultural transmission, marriage and the evolution of ethnic and religious traits. Quarterly Journal of Economics, 115(3), 955–988 (2000)
Bisin, A., & Verdier, T. (2011). The economics of cultural transmission and socialization. In J. Benhabib, A. Bisin, & M. O. Jackson (Eds.), Handbook of social economics (pp. 339–416). Amsterdam: Elsevier.
Bleakley, H., & Chin, A. (2004). Language skills and earnings: evidence from childhood immigrants. Review of Economics and Statistics, 86(2), 481–496.
Bopp, M., Braun, J., Gutzwiller, F., & Faeh, D. (2012). Health risk or resource? Gradual and independent association between self-rated health and mortality persists over 30 years. PLoS ONE, 7(2), e30795.
Brauer, J. R., Tittle, C. R., & Antonaccio, O. (2013). Does religion suppress, socialize, soothe, or support? Exploring religiosity’s influence on crime. Journal for the Scientific Study of Religion, 52(4), 753–774.
Cappa, C., Moneti, F., Wardlaw, T., & Bissell, S. (2013). Elimination of female genital mutilation/cutting. The Lancet, 382(9898), 1080–1081.
Christian, L. M., Glaser, R., Porter, K., Malarkey, W. B., Beversdorf, D., & Kiecolt-Glaser, J. K. (2011). Poorer self-rated health is associated with elevated inflammatory markers among older adults. Psychoneuroendocrinology, 36(10), 1495–1504.
Coneus, K., Laucht, M., & Reuß, K. (2012). The role of parental investments for cognitive and non-cognitive skill formation – Evidence for the first 11 years of life. Economics & Human Biology, 10(2), 189–209.
Conti, G., Heckman, J., & Urzua, S. (2010). The education-health gradient. American Economic Review, 100(2), 234–238.
Deaton, A. (2008). Income, health and well-being around the world: evidence from the Gallup World Poll. Journal of Economic Perspectives, 22(2), 53–72.
Deaton, A. (2011). Aging, religion and health. In D. A. Wise (Ed.), Explorations in the economics of Ageing (pp. 237–268). Chicago: University of Chicago Press.
DeSalvo, K. B., Bloser, N., Reynolds, K., He, J., & Muntner, P. (2006). Mortality prediction with a single general self-rated health question: a meta-analysis. Journal of General Internal Medicine, 21(3), 267–275.
Diehl, C., Koenig, M., & Ruckdeschel, K. (2009). Religiosity and gender equality: comparing natives and Muslim migrants in Germany. Ethnic and Racial Studies, 32(2), 278–301.
Durlauf, S. N., Kourtellos, A., & Tan, C. M. (2012). Is God in the details? A reexamination of the role of religion in economic growth. Journal of Applied Econometrics, 27(7), 1059–1075.
Dzekedzeke, K., Siziya, S., & Fylkenes, K. (2008). The impact of HIV infection on adult mortality in some communities in Zambia: a cohort study. Tropical Medicine and International Health, 13(2), 152–161.
Ellison, C. G., & Hummer, R. A. (2010). Religion, families and health population-based research in the United States. New Brunswick: Rutgers University Press.
Ellison, C. G., & Lee, J. (2010). Spiritual struggles and psychological distress: is there a dark side of religion? Social Indicators Research, 98(3), 501–517.
Ellison, C. G., & Levin, J. S. (1998). The religion-health connection: evidence, theory and future directions. Health Education & Behavior, 25(6), 700–720.
Exline, J. J. (2002). Stumbling blocks on the religious road: fractured relationships, nagging vices and the inner struggle to believe. Psychological Inquiry, 13(3), 182–189.
Falk, A., Becker, A., Dohmen, T., Enke, B., Huffman, D., & Sunde, U. (2018). Global evidence on economic preferences. Quarterly Journal of Economics, 133(4), 1645–1692.
Feinstein, M., Liu, K., Ning, H., Fitchett, G., & Lloyd-Jones, D. M. (2010). Burden of cardiovascular risk factors, subclinical atherosclerosis and incident cardiovascular events across dimensions of religiosity: the multi-ethnic study of atherosclerosis. Circulation, 121(5), 659–666.
Fernández, R. (2011). Does culture matter? In J. Benhabib, A. Bisin, & M. O. Jackson (Eds.), Handbook of social economics (pp. 481–510). Amsterdam: Elsevier.
Fernández, R., & Fogli, A. (2006). Fertility: the role of culture and family experience. Journal of the European Economic Association, 4(2–3), 552–561.
Ferraro, K. F., & Kelley-Moore, J. A. (2000). Religious consolation among men and women: do health problems spur seeking? Journal for the Scientific Study of Religion, 39(2), 220–234.
Ferrer-i-Carbonell, A., & Frijters, P. (2004). How important is methodology for the estimates of the determinants of happiness? Economic Journal, 114(497), 641–659.
Gallup (2009). What Alabamians and Iranians have in common. https://news.gallup.com/poll/114211/Alabamians-Iranians-Common.aspx. Accessed 2 May 2016.
Gershoff, E. T. (2010). More harm than good: a summary of scientific research on the intended and unintended effects of corporal punishment on children. Law and Contemporary Problems, 73(Spring), 31–56.
Gervais, W. M., & Norenzayan, A. (2012). Analytic thinking promotes religious disbelief. Science, 336(6080), 493–496.
Grogan-Kaylor, A., & Otis, M. D. (2007). The predictors of parental use of corporal punishment. Family Relations, 56(1), 80–91.
Hill, T. D., & Cobb, R. J. (2011). Religious involvement and religious struggles. In A. Blasi (Ed.), Toward a sociological theory of religion and health (pp. 239–260). Leiden: Brill.
Hofstede, G., Hofstede, G. J., & Minkov, M. (2010). Cultures and organizations: Software of the mind. New York: McGraw-Hill.
Huijts, T., & Kraaykamp, G. (2012). Immigrants’ health in Europe: a cross-classified multilevel approach to examine origin country, destination country and community effects. International Migration Review, 46(1), 101–137.
Idler, E., & Kasl, S. (1995). Self-ratings of health: do they also predict change in functional ability? Journals of Gerontology, 50B(6), S344–S353.
Idler, E., Ellison, C., George, L., Krause, N., Ory, M., Pargament, K., et al. (2003). Measuring multiple dimensions of religion and spirituality for health research: conceptual background and findings from the 1998 General Social Survey. Research on Aging, 25(4), 327–365.
Jacob, K., & Kalter, F. (2013). Intergenerational change in religious salience among immigrant families in four European countries. International Migration, 51(3), 38–56.
Jegede, A. S. (2007). What led to the Nigerian boycott of the polio vaccination campaign? PLoS Medicine, 4(3), e73.
Jelinek, G. A. (2017). Determining causation from observational studies: A challenge for modern neuroepidemiology. Frontiers in Neurology, 8, 1–3.
Johansson-Stenman, O., Mahmud, M., & Martinsson, P. (2009). Trust and religion: experimental evidence from Bangladesh. Economica, 76(303), 462–485.
Johnston, D. W., Propper, C., & Shields, M. A. (2009). Comparing subjective and objective measures of health: evidence from hypertension for the income/health gradient. Journal of Health Economics, 28(3), 540–552.
Jürges, H. (2007). True health vs. response styles: exploring cross-country differences in self-reported health. Health Economics, 16(2), 163–178.
Jylhä, M. (2009). What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Social Science and Medicine, 69(3), 307–316.
Kim, D., Subramanian, S. V., & Kawachi, I. (2008). Social capital and physical health: a systematic review of the literature. In I. Kawachi, S. V. Subramanian, S.V. & D. Kim (Eds.), Social capital and health (pp. 139–190). Berlin: Springer.
Klingorová, K., & Havlíček, T. (2015). Religion and gender inequality: the status of women in the societies of world religions. Moravian Geographical Reports, 23(2), 2–11.
Koenig, H. G., King, D. E., & Carson, V. B. (2012). Handbook of religion and health. Oxford: Oxford University Press.
Kortt, M. A., & Dollery, B. (2014). Religion and BMI in Australia. Journal of Religion and Health, 53(1), 217–228.
Ljunge, M. (2014a). Trust issues: Evidence on the intergenerational trust transmission among children of immigrants. Journal of Economic Behavior & Organization, 106(October), 175–196.
Ljunge, M. (2014b). Social capital and health: evidence that ancestral trust promotes health among children of immigrants. Economics and Human Biology, 15(December), 165–186.
Ljunge, M. (2016). Migrants, health, and happiness: evidence that health assessments travel with migrants and predict well-being. Economics and Human Biology, 22(September), 35–46.
Koball, H., Moiduddin, E., Henderson, J., Goesling, B., & Besculides, M. (2010). What do we know about the link between marriage and health? Journal of Family Issues, 31(8), 1019–1040.
Lynn, R., Harvey, J., & Nyborg, H. (2009). Average intelligence predicts atheism rates across 137 nations. Intelligence, 37(1), 11–15.
Lynn, R., & Meisenberg, G. (2010). National IQs calculated and validated for 108 nations. Intelligence, 38(4), 353–360.
McFadden, E., Luben, R., Bingham, S., Wareham, N., Kinmonth, A. L., & Khaw, K.-T. (2009). Does the association between self-rated health and mortality vary by social class? Social Science and Medicine, 68(2), 275–280.
Mackenbach, J. P., Martikainen, P., Looman, C. W. N., Dalstra, J. A. A., Kunst, A. E., & Lahelma, E. (2005). The shape of the relationship between income and self-assessed health: an international study. International Journal of Epidemology, 34(2), 286–293.
Nicholson, A., Rose, R., & Bobak, M. (2010). Associations between different dimensions of religious involvement and self-rated health in diverse European populations. Health Psychology, 29(2), 227–235.
Oman, D. (2018). Elephant in the room: why spirituality and religion matter for public health. In D. Oman (Ed.), Why religion and spirituality matter for public health: Evidence, implications and resources (pp. 1–18). Berlin: Springer.
Oman, D., & Syme, S. L. (2018). Weighing the evidence: What is revealed by 100+ meta-analyses and systematic reviews of religion/spirituality and health? In D. Oman (Ed.), Why religion and spirituality matter for public health: Evidence, implications and resources (pp. 261–281). Berlin: Springer.
Oman, D., & Thoresen, C. E. (2017). Do religion and spirituality influence health? In L. F. Paloutzian & C. L. Park (Eds.), Handbook of the psychology of religion and spirituality (pp. 435–459). New York: Guilford Press.
Pot, A. M., Portrait, F., Visser, G., Puts, M., Broese van Groenou, M. I., & Deeg, D. J. H. (2009). Utilization of acute and long-term care in the last year of life comparison with survivors in a population-based study. BMC Health Services Research, 9, article 139.
Rechel, B., Mladovsky, P., Ingleby, D., Mackenbach, J., & McKee, M. (2013). Migration and health in an increasingly diverse Europe. The Lancet, 381(9873), 1235–1245.
Saad, M., Daher, J. C., & de Medeiros, R. (2019). Spirituality, religiousness and physical health: Scientific evidence. In G. Lucchetti, M. F. Prieto Peres & R. F. Damiano (Eds.), Spirituality, religiousness and health: From research to clinical practice (pp. 87–100). Berlin: Springer.
Samanni, M., Teorell, J., Kumlin, S., & Rothstein, B. (2010). The QoG social policy dataset, version 11Nov10 . https://www.qog.pol.gu.se. Accessed 3 May 2016.
Schierman, S., Bierman, A., & Ellison, C. G. (2013). Religion and mental health. In C. S. Aneshensel, J. C. Phelan, & A. Bierman (Eds.), Handbook of the sociology of mental health (pp. 457–478). Berlin: Springer.
Schnabel, L. (2016). Religion and gender equality worldwide: a country-level analysis. Social Indicators Research, 129(2), 893–907.
Schneider, F., Linsbauer, K., & Heinemann, F. (2015). Religion and the shadow economy. Kyklos, 68(1), 111–141.
Terry, K. J. (2008). Stained glass: the nature and scope of child sexual abuse in the Catholic Church. Criminal Justice and Behavior, 35(5), 549–569.
van de Pol, J., & van Tubergen, F. (2014). Inheritance of religiosity among Muslim immigrants in a secular society. Review of Religious Research, 56(1), 87–106.
van Hoorn, A., & Maseland, R. (2013). Does a Protestant work ethic exist? Evidence from the well-being effect of unemployment. Journal of Economic Behavior & Organization, 91(July), 1–12.
VanderWeele, T. J. (2017a). Religion and health: a synthesis. In M. J. Balboni & J. R. Peteet (Eds.), Spirituality and religion within the culture of medicine (pp. 357–401). Oxford: Oxford University Press.
VanderWeele, T. J. (2017b). Religion and health in Europe: cultures, countries, context. European Journal of Epidemiology, 32(10), 857–861.
VanderWeele, T. J. (2017c). Causal effects of religious service attendance? Social Psychiatry and Psychiatric Epidemiology, 52(11), 1331–1336.
Weil, D. N. (2014). Health and economic growth. In P. Aghion & S. N. Durlauf (Eds.), Handbook of economic growth (Vol. 2B, pp. 623–682). Amsterdam: Elsevier.
Wilkinson, R. G., & Picket, K. (2009). The spirit level: Why more equal societies almost always do better. London: Allen Lane.
Wiseman, T., & Young A. (2014). Religion: productive or unproductive? Journal of Institutional Economics, 10(1), 21–45.
Zimmer, Z., Rojo, F., Ofstedal, M. B., Chiu, C.-T., Saito, Y., & Jagger, C. (2019). Religiosity and health: a global comparative study. SSM – Population Health, 7(April), 100322.
Zuckerman, M., Silberman, J., & Hall, J. A. (2013). The relation between intelligence and religiosity: a meta-analysis and some proposed explanations. Personality and Social Psychology Review, 17(4), 325–354.
Acknowledgements
We are very grateful to Carl Magnus Bjuggren, Pavel Chalupníček, Eelke de Jong, Ilpo Kauppinen, Therese Nilsson and Martin Rode, to seminar participants at Radboud University Nijmegen and the University of Navarra and to conference participants at the Public Choice Society conference in Fort Lauderdale and the European Public Choice Society conference in Freiburg for helpful comments and suggestions on an earlier version of this paper, to Fredrik Andersson for excellent research assistance, and to Johan och Jakob Söderbergs Stiftelse (grants 47/19, FA20-0001), Jan Wallanders och Tom Hedelius stiftelse (grants P19-0180, P2017:0075:1), Riksbankens Jubileumsfond (grant P17-0206:1) and the Czech Science Foundation (GA ČR) (grant 19-03102S) for financial support.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Berggren, N., Ljunge, M. Good Faith and Bad Health: Self-Assessed Religiosity and Self-Assessed Health of Women and Men in Europe. Soc Indic Res 153, 323–344 (2021). https://doi.org/10.1007/s11205-020-02495-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11205-020-02495-5