
Abstract
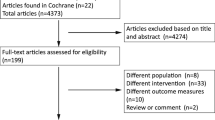
The aim of this study is to compare the efficacy of bromocriptine (BRC) versus cabergoline (CAB) in patients with giant prolactinomas. We searched MEDLINE, EMBASE, CENTRAL and Clinical Trials.gov for studies dated before March 1st, 2016, that used BRC or CAB for the treatment of patients with giant prolactinomas. Specific eligibility criteria were set to identify articles and cases. The selected articles were reviewed, and the data were extracted for analysis. The compared outcomes included tumor shrinkage, tumor response, normalization of prolactin (PRL) level, and visual field defect (VFD) improvement. Gender differences were also considered. Differences between the groups were assessed using Student’s t test and the chi-square test. Two hundred and forty-five records were identified, and 10 articles and 104 cases met the inclusion criteria. Based on our analysis, CAB is significantly better than BRC in normalizing PRL levels in patients, especially males, with giant prolactinomas (69.4% versus 31.7%, p = 0.01). However, there was no significant difference between the two drugs in terms of tumor shrinkage, tumor response and VFD improvement (p > 0.05) in male or female patients. CAB exhibits significantly better efficacy than BRC in the normalization of PRL levels in male patients with giant prolactinomas. Regarding tumor reduction and VFD improvement, both drugs are comparably effective for patients of both genders. This quantitative and systematic review provides preliminary evidence in favor of CAB as a medical therapy for treating giant prolactinomas in male patients, especially those with extremely high PRL levels.

Similar content being viewed by others


References
Acharya SV, Gopal RA, Menon PS, Bandgar TR, Shah NS (2010) Giant prolactinoma and effectiveness of medical management. Endocr Pract 16:42–46
Al-Husaynei AJ, Mahmood IH, Al-Jubori ZS (2008) Comparison of the effects of cabergoline and bromocriptine in women with hyperprolactinemic amenorrhea. Middle East Fertil Soc J 13:33–38
Bahceci M, Sismanoglu A, Ulug U (2010) Comparison of cabergoline and bromocriptine in patients with asymptomatic incidental hyperprolactinemia undergoing ICSI-ET. Gynecol Endocrinol 26:505–508
Bancroft J, O'Carroll R, McNeilly A, Shaw RW (1984) The effects of bromocriptine on the sexual behaviour of hyperprolactinaemic man: a controlled case study. Clin Endocrinol 21:131–137
Blettner M, Sauerbrei W, Schlehofer B, Scheuchenpflug T, Friedenreich C (1999) Traditional reviews, meta-analyses and pooled analyses in epidemiology. Int J Epidemiol 28:1–9
Bonsu KO, Reidpath DD, Kadirvelu A (2016) Lipophilic Statin Versus Rosuvastatin (Hydrophilic) Treatment for Heart Failure: a Meta-Analysis and Adjusted Indirect Comparison of Randomised Trials. Cardiovasc Drugs Ther 30:177–188
Brozek J, Oxman A, Schünemann H (2012) GRADEpro [Computer program], Version 3.2 for Windows. 2008
Capozzi A, Scambia G, Pontecorvi A, Lello S (2015) Hyperprolactinemia: pathophysiology and therapeutic approach. Gynecol Endocrinol 31:506–510
Cho EH, Lee SA, Chung JY, Koh EH, Cho YH, Kim JH, Kim CJ, Kim MS (2009) Efficacy and safety of cabergoline as first line treatment for invasive giant prolactinoma. J Korean Med Sci 24:874–878
Ciccarelli A, Daly AF, Beckers A (2005) The epidemiology of prolactinomas. Pituitary 8:3–6
Colao A, Annunziato L, Lombardi G (1998) Treatment of prolactinomas. Ann Med 30:452–459
Colao A, Chanson P (2009) The prolactinoma. Best Pract Res Clin Endocrinol Metab 23:575–596
Colao A, Di Sarno A, Guerra E, De Leo M, Mentone A, Lombardi G (2006) Drug insight: cabergoline and bromocriptine in the treatment of hyperprolactinemia in men and women. Nat Clin Pract Endocrinol Metab 2:200–210
Colao A, Di Sarno A, Landi ML et al (2000b) Macroprolactinoma shrinkage during cabergoline treatment is greater in naive patients than in patients pretreated with other dopamine agonists: a prospective study in 110 patients. J Clin Endocrinol Metab 85:2247–2252
Colao A, Di Sarno A, Marzullo P et al (2000a) New medical approaches in pituitary adenomas. Horm Res 53:76–87
Colao A, di Sarno A, Pivonello R, di Somma C, Lombardi G (2002) Dopamine receptor agonists for treating prolactinomas. Expert Opin Investig Drugs 11:787–800
Colao A, Pivonello R, Di Somma C, Savastano S, Grasso LF, Lombardi G (2009) Medical therapy of pituitary adenomas: effects on tumor shrinkage. Rev Endocr Metab Disord 10:111–123
Colao A, Savastano S (2011) Medical treatment of prolactinomas. Nat Rev Endocrinol 7:267–278
Corsello S, Ubertini G, Altomare M, Lovicu R, Migneco M, Rota CA, Colosimo C (2003) Giant prolactinomas in men: efficacy of cabergoline treatment. Clin Endocrinol 58:662–670
Cuny T, Barlier A, Feelders R, Weryha G, Hofland LJ, Ferone D, Gatto F (2015) Medical therapies in pituitary adenomas: Current rationale for the use and future perspectives. Ann Endocrinol (Paris) 76:43–58
Davis JR, Sheppard MC, Heath DA (1990) Giant invasive prolactinoma: a case report and review of nine further cases. Q J Med 74:227–238
De Rosa M, Colao A, Di Sarno A et al (1998) Cabergoline treatment rapidly improves gonadal function in hyperprolactinemic males: a comparison with bromocriptine. Eur J Endocrinol 138:286–293
Delgrange E, Raverot G, Bex M et al (2013) Giant prolactinomas in women. Eur J Endocrinol 170:31–38
Di Sarno A, Landi ML, Cappabianca P et al (2001) Resistance to cabergoline as compared with bromocriptine in hyperprolactinemia: prevalence, clinical definition, and therapeutic strategy. J Clin Endocrinol Metab 86:5256–5261
dos Santos Nunes V, El Dib R, Boguszewski CL, Nogueira CR (2011) Cabergoline versus bromocriptine in the treatment of hyperprolactinemia: a systematic review of randomized controlled trials and meta-analysis. Pituitary 14:259–265
Easterbrook PJ, Berlin JA, Gopalan R, Matthews DR (1991) Publication bias in clinical research. Lancet 337:867–872
Eisenhauer EA, Therasse P, Bogaerts J et al (2009) New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 45:228–247
Gillam MP, Molitch ME, Lombardi G, Colao A (2006) Advances in the treatment of prolactinomas. Endocr Rev 27:485–534
Jansen JP, Fleurence R, Devine B et al (2011) Interpreting indirect treatment comparisons and network meta-analysis for health-care decision making: report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: part 1. Value Health 14:417–428
Koppelman MC, Parry BL, Hamilton JA, Alagna SW, Loriaux DL (1987) Effect of bromocriptine on affect and libido in hyperprolactinemia. Am J Psychiatry 144:1037–1041
Lou XH, Wu ZB, Zhang YZ (2013) Bromocriptine-induced Brainstem Angulation in a Patient With Invasive Prolactinoma. J Clin Endocrinol Metab 98:867–868
Lundin P, Pedersen F (1992) Volume of pituitary macroadenomas: assessment by MRI. J Comput Assist Tomogr 16:519–528
Maiter D, Delgrange E (2014) Therapy of endocrine disease: the challenges in managing giant prolactinomas. Eur J Endocrinol 170:R213–R227
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group (2010) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 8:336–341
Molitch ME (2005) Pharmacologic Resistance in Prolactinoma Patients. Pituitary 8:43–52
Moraes AB, Silva CM, Vieira Neto L, Gadelha MR (2013) Giant prolactinomas: the therapeutic approach. Clin Endocrinol 79:447–456
Pascal-Vigneron V, Weryha G, Bosc M, Leclere J (1995) Hyperprolactinemic amenorrhea: treatment with cabergoline versus bromocriptine. Results of a national multicenter randomized double-blind study. Presse Med 24:753–757
Sabuncu T, Arikan E, Tasan E, Hatemi H (2001) Comparison of the effects of cabergoline and bromocriptine on prolactin levels in hyperprolactinemic patients. Intern Med 40:857–861
Saeki N, Nakamura M, Sunami K, Yamaura A (1998) Surgical indication after bromocriptine therapy on giant prolactinomas: effects and limitations of the medical treatment. Endocr J 45:529–537
Shimon I, Benbassat C, Hadani M (2007) Effectiveness of long-term cabergoline treatment for giant prolactinoma: study of 12 men. Eur J Endocrinol 156:225–231
Shrivastava RK, Arginteanu MS, King WA, Post KD (2002) Giant prolactinomas: clinical management and long-term follow up. J Neurosurg 97:299–306
Stroup DF, Berlin JA, Morton SC et al (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 283:2008–2012
Webster J, Piscitelli G, Polli A, Ferrari CI, Ismail I, Scanlon MF (1994) A comparison of cabergoline and bromocriptine in the treatment of hyperprolactinemic amenorrhea. Cabergoline Comparative Study Group. N Engl J Med 331:904–909
Wu ZB, Yu CJ, Su ZP, Zhuge QC, Wu JS, Zheng WM (2006) Bromocriptine treatment of invasive giant prolactinomas involving the cavernous sinus: results of a long-term follow up. J Neurosurg 104:54–61
Yang MS, Hong JW, Lee SK, Lee EJ, Kim SH (2011) Clinical management and outcome of 36 invasive prolactinomas treated with dopamine agonist. J Neuro-Oncol 104:195–204
Acknowledgements
This work was supported by the National Natural Science Foundation of China (81471392 and 81671371) and the Shanghai Municipal Education Commission Gaofeng Clinical Medicine Grant Support (20161407).
Funding
This work was supported by the National Natural Science Foundation of China (81471392 and 81671371) and the Shanghai Municipal Education Commission Gaofeng Clinical Medicine Grant Support (20161407).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest.
Electronic supplementary material
ESM 1
(DOCX 37 kb)
Rights and permissions
About this article

Cite this article
Huang, H.Y., Lin, S.J., Zhao, W.G. et al. Cabergoline versus bromocriptine for the treatment of giant prolactinomas: A quantitative and systematic review. Metab Brain Dis 33, 969–976 (2018). https://doi.org/10.1007/s11011-018-0217-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11011-018-0217-3