
Abstract
There are two salient facts about health care in low and middle-income countries; (1) the private sector plays an important role and (2) the care provided is often of poor quality. Despite these facts we know little about what drives quality of care in the private sector and why patients seek care from poor quality providers. We use two field studies in India that provide insight into this issue. First, we use a discrete choice experiment to show that patients strongly value technical quality. Second, we use standardized patients to show that better quality providers are not able to charge higher prices. Instead providers are able to charge higher prices for elements of quality that the patient can observe, which are less important for health outcomes. Future research should explore whether accessible information on technical quality of local providers can shift demand to higher quality providers and improve health outcomes.

Source Survey carried out by authors

Source Data comes from standardized patient reports conducted by Mohanan et al. (2015)
Similar content being viewed by others


Notes
This reduces the need for the “stability assumption” outlined by Hainmueller et al. (2013).
This reduces the need for the “no profile-order effects” outlined by Hainmueller et al. (2013).
References
Alkire, B. C., Peters, A. W., Shrime, M. G., & Meara, J. G. (2018). The economic consequences of mortality amenable to high-quality health care in low-and middle-income countries. Health Affairs, 37(6), 988–996.
Andaleeb, S. S., Siddiqui, N., & Khandakar, S. (2007). Patient satisfaction with health services in Bangladesh. Health Policy and Planning, 22(4), 263–273.
Arrow, K. J. (1963). Uncertainty and the welfare economics of medical care. Am Economic Review, 53(5), 941–973.
Banerjee, A., Deaton, A., & Duflo, E. (2004). Health, health care, and economic development: Wealth, health, and health services in rural Rajasthan. American Economic Review, 94(2), 326.
Basu, S., Andrews, J., Kishore, S., Panjabi, R., & Stuckler, D. (2012). Comparative performance of private and public healthcare systems in Low-and middle-income countries: A systematic review. PLoS Medicine, 9(6), e1001244.
Berendes, S., Heywood, P., Oliver, S., & Garner, P. (2011). Quality of private and public ambulatory health care in low and middle income countries: Systematic review of comparative studies. PLoS Medicine, 8(4), e1000433.
Das, J., Chowdhury, A., Hussam, R., & Banerjee, A. V. (2016a). The impact of training informal health care providers in India: A randomized controlled trial. Science, 354(6308), 7384.
Das, J., Hammer, J., & Leonard, K. (2008). The quality of medical advice in low-income countries. The Journal of Economic Perspectives, 22, 93–114.
Das, J., Holla, A., Das, V., Mohanan, M., Tabak, D., & Chan, B. (2012). In Urban and rural India, a standardized patient study showed low levels of provider training and huge quality gaps. Health Affairs, 31(12), 2774–2784.
Das, J., Holla, A., Mohpal, A., & Muralidharan, K. (2016b). Quality and accountability in health care delivery: audit-study evidence from primary care in India. American Economic Review, 106(12), 3765–3799.
Das, J. K., Salam, R. A., & Bhutta, Z. A. (2014). Global Burden of Childhood Diarrhea and Interventions. Current Opinion in Infectious Diseases, 27(5), 451–458.
Das, J., Woskie, L., Rajbhandari, R., Abbasi, K., & Jha, A. (2018). Rethinking assumptions about delivery of healthcare: Implications for universal health coverage. BMJ, 361, k1716.
DHS. (2016). India demographic and health survey 2016. I. M. o. H. a. F. Welfare
Dupas, P., & Miguel, E. (2017). Impacts and determinants of health levels in low-income countries. Handbook of Economic Field Experiments, 2, 3–93.
Fung, C. H., Lim, Y. W., Mattke, S., Damberg, C., & Shekelle, P. G. (2008). Systematic review: The evidence that publishing patient care performance data improves quality of care. Annals of Internal Medicine, 148(2), 111–123.
Grépin, K. A. (2016). Private sector an important but not dominant provider of key health services in low-and middle-income countries. Health Affairs, 35(7), 1214–1221.
Hanson, K., McPake, B., Nakamba, P., & Archard, L. (2005). Preferences for hospital quality in Zambia: results from a discrete choice experiment. Health Economics, 14(7), 687–701.
Jin, G. Z., & Leslie, P. (2005). The case in support of restaurant hygiene grade cards. Choices, 20(2), 97–102.
Kassegne, S., Kays, M. B., & Nzohabonayo, J. (2011). Evaluation of a social marketing intervention promoting oral rehydration salts in Burundi. BMC Public Health, 11(1), 155.
Kim, S. S., Kaplowitz, S., & Johnston, M. V. (2004). The effects of physician empathy on patient satisfaction and compliance. Evaluation and the Health Professions, 27(3), 237–251.
Kitapci, O., Akdogan, C., & Dortyol, I. T. (2014). The impact of service quality dimensions on patient satisfaction, repurchase intentions and word-of-mouth communication in the Public Healthcare Industry. Procedia-Social and Behavioral Sciences, 148, 161–169.
Kleinman, L., Mcintosh, E., Ryan, M., Schmier, J., Crawley, J., Locke, G. R., & Lissovoy, G. D. (2002). Willingness to pay for complete symptom relief of gastroesophageal reflux disease. Archives of Internal Medicine, 162(12), 1361–1366.
Kremer, M., & Glennerster, R. (2011). Improving health in developing Countries. Handbook of Health Economics, 2, 201–315.
Kruk, M. E., Gage, A. D., Arsenault, C., Jordan, K., Leslie, H. H., Wan, S. R. D., Adeyi, O., Barker, P., Daelmans, B., & Doubova, S. V. (2018). High-quality health systems in the sustainable development goals Era: Time for a revolution. The Lancet Global Health, 6(11), e1196–e1252.
Lagarde, M., & Palmer, N. (2008). The impact of user fees on health service utilization in low-and middle-income Countries: How strong is the evidence? Bulletin of the World Health Organization, 86, 839–848.
Leatherman, S., Berwick, D., Iles, D., Lewin, L. S., Davidoff, F., Nolan, T., & Bisognano, M. (2003). The business case for quality: Case studies and an analysis. Health Affairs, 22(2), 17–30.
Lenters, L. M., Das, J. K., & Bhutta, Z. A. (2013). Systematic review of strategies to increase use of oral rehydration solution at the household level. BMC Public Health, 13(3), S28.
Meeker, D., Linder, J. A., Fox, C. R., Friedberg, M. W., Persell, S. D., Goldstein, N. J., Knight, T. K., Hay, J. W., & Doctor, J. N. (2016). Effect of behavioral interventions on inappropriate antibiotic prescribing among primary care practices: A randomized clinical trial. JAMA, 315(6), 562–570.
Mohanan, M., Babiarz, K. S., Goldhaber-Fiebert, J. D., Miller, G., & Vera-Hernández, M. (2016). Effect of a large-scale social franchising and telemedicine program on childhood diarrhea and pneumonia outcomes in India. Health Affairs, 35(10), 1800–1809.
Mohanan, M., Giardili, S., Das, V., Rabin, T. L., Raj, S. S., Schwartz, J. I., Seth, A., Goldhaber-Fiebert, J. D., Miller, G., & Vera-Hernández, M. (2017). Evaluation of a social franchising and telemedicine programme and the care provided for childhood diarrhoea and pneumonia, Bihar, India. Bulletin of the World Health Organization, 95(5), 343.
Mohanan, M., Marcos, V. H., Das, V., Giardili, S., Goldhaber-Fiebert, J. D., Rabin, T. L., Raj, S. S., Schwartz, J. I., & Seth, A. (2015). The know-do gap in quality of health care for childhood diarrhea and pneumonia in rural India. JAMA Pediatrics, 169(4), 349–357.
Murti, A., Deshpande, A., & Srivastava, N. (2013). Service quality, customer (patient) satisfaction and behavioural intention in health care services: Exploring the Indian perspective. Journal of Health Management, 15(1), 29–44.
National Academies of Sciences. (2018). Crossing the global quality chasm: Improving health care Worldwide. T. N. A. Press.
National Academies of Sciences. (2019). Engineering and medicine. Improving Health Care Worldwide. National Academies Press.
Rao, K Vaninadha, VK Mishra and RD Retherford. 1998. Knowledge and use of oral rehydration therapy for childhood diarrhoea in India: Effects of exposure to mass media.
Rethans, J. J., Gorter, S., Bokken, L., & Morrison, L. (2007). Unannounced standardised patients in real practice: A systematic literature review. Medical Education, 41(6), 537–549.
Rethans, J.-J., Sturmans, F., Drop, R., & Van der Vleuten, C. (1991). Assessment of the performance of general practitioners by the use of standardized (simulated) patients. British Journal of General Practice, 41(344), 97–99.
Robinson, J. C., Whaley, C., & Brown, T. T. (2016). Association of reference pricing for diagnostic laboratory testing with changes in patient choices, prices, and total spending for diagnostic tests. JAMA Internal Medicine, 176(9), 1353–1359.
Sood, N., & Wagner, Z. (2014). Private sector provision of oral rehydration therapy for child diarrhea in sub-saharan Africa. The American Journal of Tropical Medicine and Hygiene, 90(5), 939–944.
Sood, N., Wagner, Z., Huckfeldt, P., & Haviland, A. M. (2013). Price shopping in consumer-directed health plans. Forum for Health Economics and Policy., 25, 35–53.
Srivastava, A., Avan, B. I., Rajbangshi, P., & Bhattacharyya, S. (2015). Determinants of women’s satisfaction with maternal health care: A review of literature from developing countries. BMC Pregnancy and Childbirth, 15(1), 97.
Tang, Y., Liu, C., & Zhang, X. (2016). Public reporting as a prescriptions quality improvement measure in primary care settings in china: Variations in effects associated with diagnoses. Scientific Reports, 6, 39361.
USAID/UNICEF/WHO. (2005). Diarrhoea Treatment guidelines: including new recommendations for the use of ors and zinc supplementation for clinic-based healthcare workers. Arlington: USAID Micronutrient Program.
Wagner, Z., Asiimwe, J. B., Dow, W. H., & Levine, D. I. (2019). The role of price and convenience in use of oral rehydration salts to treat child diarrhea: A cluster randomized trial in Uganda. PLoS Medicine, 16(1), e1002734.
Wagner, Z., Shah, M., & Sood, N. (2014a). Barriers to use of oral rehydration salts for child diarrhea in the private sector: Evidence from India. Journal of Tropical Pediatrics, 61(1), 37–43.
Wagner, Z., Szilagyi, P. G., & Sood, N. (2014b). Comparative performance of public and private sector delivery of Bcg vaccination: evidence from Sub-Saharan Africa. Vaccine, 32(35), 4522–4528.
Whaley, C., Chafen, J. S., Pinkard, S., Kellerman, G., Bravata, D., Kocher, R., & Sood, N. (2014). Association between availability of health service prices and payments for these services. JAMA, 312(16), 1670–1676.
World Health Organization. (2018). Delivering quality health services: A global imperative for universal health coverage.
World Health Organization Department of Child Adolescent Health World Health Organization and UNICEF. (2005). Handbook IMCI: Integrated management of childhood illness. World Health Organization.
Yang, L., Liu, C., Wang, L., Yin, Xi., & Zhang, X. (2014). Public reporting improves antibiotic prescribing for upper respiratory tract infections in primary care: A matched-pair cluster-randomized trial in China. Health Research Policy and Systems, 12(1), 61.
Zanolini, A., Sikombe, K., Sikazwe, I., Eshun-Wilson, I., Somwe, P., Moore, C. B., Topp, S. M., Czaicki, N., Beres, L. K., & Mwamba, C. P. (2018). Understanding preferences for Hiv care and treatment in Zambia: Evidence from a discrete choice experiment among patients who have been lost to follow-up. PLoS Medicine, 15(8), e1002636.
Zhang, X., Haviland, A., Mehrotra, A., Huckfeldt, P., Wagner, Z., & Sood, N. (2018). Does enrollment in high-deductible health plans encourage price shopping? Health Services Research, 53, 2718–2734.
Acknowledgements
We would like to thank Rebecca Dizon-Ross, Jishnu Das, and participants at ASHEcon 2019 and AEA 2020 conferences for helpful comments. We would also like to thank Sneha Nimmagadda for excellent field work management. Data is available upon reasonable request. Replication data and code will be made available upon publication. This work was partly funded by the National Institute of Diabetes and Digestive and Kidney Diseases (Grant Number: R01DK126049; PI Wagner).
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix 1 Supplementary analysis and extra data
See Figs.

Source Survey carried out by authors
Patient preferences for provider characteristics (estimated using logit). Data comes from a discrete choice experiment. Each point represents the marginal effect from a single logit model with choice-set fixed-effects. The top attribute level within each attribute category represents the reference to which the other attribute levels are compared.
3,

Distribution of Doctor Prices. This figure presents the distribution of prices charged for a consultation related to child diarrhea or pneumonia as reported by standardized patients. The prices do not include medication, tests, or any other fees that may have been incurred
4,

5,

Association between quality and prices (truncated at 95th percentile). Each point represents the coefficient from a linear regression with doctor fee (truncated at the 95th percentile) as the dependent variable and the quality metric indicated on the y-axis as the explanatory variable, while controlling for provider characteristics (age, sex, years of experience, training, and whether the facility has electricity). Confidence intervals were estimated using robust standard errors. Panel C pools diarrhea and pneumonia cases. There were no providers that gave the correct treatment for diarrhea
6,

Association between quality and prices (Generalized Linear Model with log link). Each point represents the coefficient from a linear regression with doctor fee (truncated at the 95th percentile) as the dependent variable and the quality metric indicated on the y-axis as the explanatory variable, while controlling for provider characteristics (age, sex, years of experience, training, and whether the facility has electricity). Confidence intervals were estimated using robust standard errors. Panel C pools diarrhea and pneumonia cases. There were no providers that gave the correct treatment for diarrhea
7,

Association between quality and prices (excluding zero prices). Each point represents the coefficient from a linear regression with doctor fee (truncated at the 95th percentile) as the dependent variable and the quality metric indicated on the y-axis as the explanatory variable, while controlling for provider characteristics (age, sex, years of experience, training, and whether the facility has electricity). Confidence intervals were estimated using robust standard errors. Panel C pools diarrhea and pneumonia cases. There were no providers that gave the correct treatment for diarrhea
8,

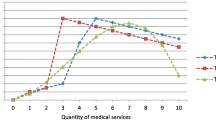
Source Data comes from standardized patient reports conducted by Mohanan et al. (2015)
Returns to good patient assessment at different levels of technical quality (diarrhea and pneumonia combined). Each set of points associated with a technical quality outcome (combination of red and blue dots) is estimated from the same regression using an interaction between the measure of patient assessment (global assessment index, liked doctor, would return to doctor) and measure of technical quality (correct treatment, correct diagnosis, ORS). The red dots are the coefficient on the patient assessment measure and the blue dots are the sum of the coefficient on the interaction term and the coefficient on the patient assessment measure. Therefore, the red points represent the additional price that doctors with poor technical quality are able to charge for having a positive patient assessment, and the blue points represent the additional price that doctors with good technical quality are able to charge for having a positive patient assessment (Color figure online).
9,

Sensitivity of results to authors’ covariate selection. Each range plots the upper and lower ends of the coefficient (A) or p-value (B) distribution from 64 regressions that included all possible combinations of covariates. Dashed line on Panel A is at zero. Dashed line in Panel B is at p-value of 0.05 and dotted line is at p-value of 0.10
10,

Heterogeneity in DCE result by poverty indicators. Data comes from a discrete choice experiment. Each point represents the coefficient from a linear probability model with choice-set fixed-effects. Panel A plots coefficients from two regressions, one that includes only households that reported being below the poverty line (57% of households), a common poverty measure in Indi, and one that includes only households that reported being above the poverty line (43% of households). Panel B also plots coefficients from two regressions, one that includes only caretakers with no education (28% of caretakers) and one that includes only caretakers with at least some education (72% of caretakers). The top attribute level within each attribute category represents the reference to which the other attribute levels are compared
11 and Tables
4,
5,
6,
7,
8,
9,
10,
11,
12,
13, and
14.
Appendix 2 additional information on standardized patient methods
Validity and benefits of SP method
The SP method is an established and valid method for practitioner performance measurement because it presents a well-defined incognito case in a clinically accurate and consistent manner to all practitioners. (Das et al., 2012; Rethans et al., 1991, 2007). This method has several benefits. First, it ensures illness and patient characteristics are identical across providers, which limits concerns about differential patient sorting across clinics, as might be the case when observing real patient-provider interactions. Second, because we know the actual illness being presented and the optimal care associated with the case, we can objectively score the quality of care provided. Third, we are able to observe prices charged for completed transactions, which is more accurate than prices self-reported by providers. Finally, there are no concerns about Hawthorne effects because providers are unaware that the visit is being studied.
Global assessment index
SPs rated the provider on several characteristics associated with the visit on 1–4 scales: (1) Did the provider create an environment in which you could convey your symptoms and concerns easily? (2) Did the provider appear to be knowledgeable about your illness? (3) Did the provider address your worries seriously? (4) Did the provider explain anything about your illness?
Provider sampling
Among 360 clusters in the study area for the Bihar Evaluation of Social Franchising and Telemedicine (BEST) (Mohanan, et al., 2015), 80 were selected at random. Study clusters were defined as sets of villages surrounding a central village that met eligibility criteria for a telemedicine center—the primary criteria being the availability of Internet connectivity and potential franchisees, with infrastructure such as dedicated space. The BEST team generated a list of all health care practitioners visited in the past 6 months—regardless of medical qualifications—from interviews with 64 randomly selected households with children younger than 5 years per cluster. The 5 most frequently visited primary health care practitioners in each cluster were included in the study.
Roles for standardized patients
Diarrhea case
Sangeeta said to her husband Santosh “get some medicines for Sonu, he has loose-motions, if we take him now, he’ll soil his clothes”. Sonu is suffering from loose-motions since the night before last. Yesterday night he went to pass stool 8–9 times and he has been crying too. Now that he has fallen asleep Sangeeta is thinking about getting all household work done quickly.
Santosh his wife and child stay together with his parents in a nearby village. Santosh is a 25 year old cheerful person, he has been educated till class 8. He works as a helper on a vehicle and rears cattle and earns about 2500–3000 rupees per month. He spends most of his time outside for work; he is at home from last 4 days. Sangeeta keeps the house clean but she feels that the neighborhood is not clean. They drink water from a handpump and they keep the drinking water covered but they don’t boil it.
Their son Sonu is 2 years old and all his teeth have come out. He is active all day; he is growing fine and is talkative. Sonu plays in the mud but does not eat mud; he has been vaccinated when he was an infant. Sangeeta has not seen any worms in his stool. He is not suffering from any other illness. He stopped breastfeeding just 6 months back and eats whatever is cooked in the house, though he likes to eat biscuits.
Sonu has been suffering from loose-motions since the night before last, the stool id not foamy or greasy, it does not smell foul. Sonu is crying a lot, it seems as if he has recurring pain in his stomach. There has been no vomit.
There has been no change in the food habits of Sonu, Sangeeta is feeding Sonu porridge and milk from a bottle, she cleans the bottle with warm water after feeding Sonu from it. Sonu is drinking lots of water. Santosh does not feel that his child is weak, irritated or tired. Sonu’s body is not warm on touching.
For the last two days, the child has had a diarrhea, and he has been suffering from pain in the stomach occasionally bot not all the time, and the stomach is not swollen. The diarrhea is watery, yellow, does not have mucous (chiknahat, balgam or jhag) or blood in it (the doctor may ask these questions to rule out dysentery from viral diarrhea). In addition it is not particularly foul smelling and is not, what is called `explosive diarrhea’ (the doctor may ask this to rule out giardia or other infestations). The father does not think that the child has any fever; he has not given any medicines to the child; he has given the child water to drink, but not with any salt or sugar in it.
Pneumonia case
Rita, told her husband Baliram to go and get medicine for their son Munna, as he could not sleep well last night because he was having difficulty breathing. He has fever and cough since last 5 days, which is not getting better and since last night is also having difficulty breathing.
Baliram Yadav is a 24 years old who has studied upto 8th standard. He lives with his family in a two room pucca house in the village and his family comprises of his wife, son and his parents. He works as a helper with a truck driver and from it earns rupees 4000 a month. Due to his work he stays away from home most of the time but is home since last four days.
Rita is a housewife and most of her time is spent cooking food on chulha and rearing cattle. The house she lives in does not have a toilet thus she and her family uses a nearby pit toilet in the village. She keeps her house neat and clean but feels her neighborhood is dirty. She draws drinking water for the family from a handpump and stores it in an earthen pot, which she covers but does not boil the water.
Munna their son, is 2 years old and during his birth weigh 2.4 kg. He has all his milk teeth and generally keeps well. But he has not got all the immmunisation vaccine shots. Munna does not suffer from any allergies and neither does he get any epilepsy attack.
Baliram and Rita are worried about Munna and thus when Munna had fever they consulted a village doctor who gave them some Desi medicine for it. They do not know the name of the medicine the provider gave but munna’s condition did not improve upon taking the medicine. He has got weak and is not playing much and keeps lying down most of the time. He is sleeping more than usual and is lazy. He eats normal food cooked at home and was weaned away from breastfeeding a year ago. But he loves eating biscuits. And recently he has not eaten any cold thing. Baliram has heard of a good doctor in a nearby village whose treatment is very good and thus he has come to this doctor to get medicine for Munna.
The child has been suffering from high fever for 5 days and is burning to touch. He has continuous cough which is similar in day and night. There was no blood in the cough but there was vomiting after coughing since yesterday. The child is spitting out only mucous and saliva but no phlegm. He has been breathing rapidly and his nostrils appear to be flaring when he breathes. Also, the skin between his ribs and stomach and also the neck muscles seems to be straining when he breathes. He makes a harsh sound since he started having difficulty breathing. The father tried to keep the child warm by covering him with the blanket last night when he started having this breathing difficulty. He does not have a running or blocked nose. He does not have any stomach ache but had loose motions a couple of times in the last two days. He has chest pain and also complained of head ache but no ear pain. There was been a decrease in frequency of urination and the child does not have any tears while crying. Also, the colour of the fingernails of the child has become more dark than normal.
Appendix 3 Discrete choice experiment
Sampling for DCE
See Fig.

Example choice set from discrete choice experiment. This is an example choice set but appears identical to what respondents viewed. The doctor on the left (doctor B) cost 100 rupees, has a 5 star quality rating, is 30 min away, and has an Ayurvedic degree. The doctor on the right (doctor A) cost 200 rupees, has a 3 star quality rating, is 60 min away, and has an MBBS/MD degree
12 and Table
15.
We used the 2011 Indian census to construct a sample frame of Patna, a smaller urban center in Bihar State. A geographically representative sampling strategy was used for this study. The urban wards of the city were divided into five geographical regions and 10 random starting points were selected in each region with 50 total starting points. Every 4th household from the starting point was visited until 20 interviews from each starting point were completed. Several households contacted were ineligible for the survey or refused to consent to participate in the interview. Respondents were adults over 18 years of age who were decision makers or caregivers for a child under 10 years of age in the household. Overall, 500 interviews were completed. 48.5% of households contacted were eligible for the survey and completed the interview. 16.2% of households contacted refused to be interviewed. 35.3% of households contacted were ineligible for the interview.
Instructions for DCE as seen by respondents |
Introduction to DCE |
We are interested in how people make decisions about health care and we hope that you can help us with this issue. There is no “correct” response to any of our questions and we just ask that you respond with your opinion. We will ask you to imagine what you would do if your child becomes ill. We will describe two types of doctors, and you should choose which one you would be most likely to go to for care for your child. These doctors will have different characteristics we are interested in learning about. Your responses are very important and they will directly inform decision making about health care in India. Therefore, please imagine that you are really going to make the decisions we are asking you to and answer truthfully. The doctors are different from each other in terms of the following four characteristics. Enumerator: demonstrate by hand signals that you are comparing two doctors |
Doctor fees/price |
The doctors will be charging different amount of fees for their service. Please assume that this amount is just for the doctor fees and any other charges for lab test, medicines etc. are the same for all doctors. There are four amounts of fees—Rs. 0 (Free service), Rs. 100, Rs. 200 and Rs. 300 |
Doctor fees: 0 rupees |
Doctor fees: 100 rupees |
Doctor fees: 200 rupees |
Doctor fees: 300 rupees |
Quality rating by patient or government (Randomly select either patient or government rating) |
Patient quality rating for the clinic |
Previous 50 patients have provided a quality rating based on their experience with these doctors, which is reflected using a star system from 1 to 5 stars; 5 stars represents excellent quality and 1 star represents very poor quality. Three stars looks this: and means the doctor is not “very poor quality” or “excellent quality” but somewhere in the middle |
Please remember that some of the previous patients may have rated the doctor five star and some even one start but we are showing you an average rating |
Government quality rating for the clinic |
Assume that the State Health Department visited all of the health facilities in your area and provided a single quality rating based on the quality of the doctor (e.g., prescribe the correct treatment, appropriate diagnosis, run all the correct tests, properly disinfect equipment, etc.). The quality rating is reflected using a star system |
5 stars () represents perfect quality and 1 star () represents very poor quality. Three stars looks this: |
and means the doctor is not “very poor quality” or “perfect quality” but somewhere in the middle |
Rating: 5 stars |
Rating: 3 stars |
Rating: 1 star |
Distance/time to arrive to facility |
We will ask about doctors that are at different distances from your home. Please assume that you will use same mode of transportation to visit each doctor. For example, if we indicate that a doctor is 30 min away and you prefer to use the bus to arrive at a doctor’s office, assume this means 30 min on bus. This time can be between 10 and 60 min |
Time: 10 min |
Time: 20 min |
Time: 30 min |
Time: 60 min |
Qualifications of the doctor |
We will ask you about doctors that have different degree as follows, |
(1) Allopathy (English medicine) degree (e.g. MBBS or MD degree) |
(2) Homeopathy degree (e.g. BHMS, MD, Homeopath) |
(3) Ayurvedic degree (e.g. BAMS and MD, Ayurved) |
(4) Traditional healers without any formal medical degree |
Degree: MBBS/ MD |
Degree: Homeopathic (BHMS) |
Degree: Ayurvedic (BAMS) |
Degree: No degree |
Diarrhea vignette |
I will ask you to choose between two different doctors based on the characteristics we use to describe them. Assume that all other characteristics between doctors are the same. For example, assume that the amount of the people in the waiting area, the number of seats, etc., is the same for all providers. Please choose which of the two doctors you would be most likely to visit. Even if you would prefer no doctor at all over the options given, please select which of the two doctors you would most prefer. After you make your choice, we will ask whether you would prefer to visit the chosen doctor or to not visit any doctor at all. It is very important that you think about what you would actually do in a real situation. If you need me to repeat the information about one or both of the doctors, please let me know. Feel free to ask questions |
Imagine that “child name" has been having diarrhea for the last 2 days. Each of these days he/she had 6 watery stools, fevers and he/she is now very weak and not eating or drinking very well. Now imagine that you have to choose between two different doctors from whom to seek care for your child. Let’s try a practice round. It is important that you take this exercise seriously and choose the doctor that you expect you would actually choose in real life if your child had diarrhea |
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wagner, Z., Banerjee, S., Mohanan, M. et al. Does the market reward quality? Evidence from India. Int J Health Econ Manag. 23, 467–505 (2023). https://doi.org/10.1007/s10754-022-09341-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10754-022-09341-w