
Abstract
Purpose
To compare characteristics of patients with possible statin intolerance identified using different claims-based algorithms versus patients with high adherence to statins.
Methods
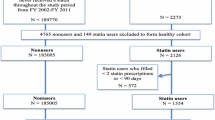
We analyzed 134,863 Medicare beneficiaries initiating statins between 2007 and 2011. Statin intolerance and discontinuation, and high adherence to statins, defined by proportion of days covered ≥80 %, were assessed during the 365 days following statin initiation. Definition 1 of statin intolerance included statin down-titration or discontinuation with ezetimibe initiation, having a claim for a rhabdomyolysis or antihyperlipidemic event followed by statin down-titration or discontinuation, or switching between ≥3 types of statins. Definition 2 included beneficiaries who met Definition 1 and those who down-titrated statin intensity. We also analyzed beneficiaries who met Definition 2 of statin intolerance or discontinued statins.
Results
The prevalence of statin intolerance was 1.0 % (n = 1320) and 5.2 % (n = 6985) using Definitions 1 and 2, respectively. Overall, 45,266 (33.6 %) beneficiaries had statin intolerance by Definition 2 or discontinued statins and 55,990 (41.5 %) beneficiaries had high adherence to statins. Compared with beneficiaries with high adherence to statins, those with statin intolerance and who had statin intolerance or discontinued statins were more likely to be female versus male, and black, Hispanic or Asian versus white. The multivariable adjusted odds ratio for statin intolerance by Definitions 1 and 2 comparing patients initiating high versus low/moderate intensity statins were 2.82 (95%CI: 2.42–3.29), and 8.58 (8.07–9.12), respectively, and for statin intolerance or statin discontinuation was 2.35 (2.25–2.45).
Conclusions
Definitions of statin intolerance presented herein can be applied to analyses using administrative claims data.


Similar content being viewed by others


References
Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–78.
Taylor F, Ward K, Moore TH et al. Statins for the primary prevention of cardiovascular disease. Cochrane Database Syst Rev 2011:CD004816.
Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. Circulation. 2014;129:S1–45.
Third Report of the National Cholesterol Education Program (NCEP. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143–421.
Mann D, Reynolds K, Smith D, Muntner P. Trends in statin use and low-density lipoprotein cholesterol levels among US adults: impact of the 2001 National Cholesterol Education Program guidelines. Ann Pharmacother. 2008;42:1208–15.
Muntner P, Levitan EB, Brown TM, et al. Trends in the prevalence, awareness, treatment and control of high low density lipoprotein-cholesterol among United States adults from 1999 to 2000 through 2009-2010. Am J Cardiol. 2013;112:664–70.
Zhang H, Plutzky J, Skentzos S, et al. Discontinuation of statins in routine care settings: a cohort study. Ann Intern Med. 2013;158:526–34.
Cohen JD, Brinton EA, Ito MK, Jacobson TA. Understanding statin use in America and gaps in patient education (USAGE): an internet-based survey of 10,138 current and former statin users. J Clin Lipidol. 2012;6:208–15.
Parker BA, Capizzi JA, Grimaldi AS, et al. Effect of statins on skeletal muscle function. Circulation. 2013;127:96–103.
Bruckert E, Hayem G, Dejager S, Yau C, Begaud B. Mild to moderate muscular symptoms with high-dosage statin therapy in hyperlipidemic patients--the PRIMO study. Cardiovasc Drugs Ther. 2005;19:403–14.
Wei MY, Ito MK, Cohen JD, Brinton EA, Jacobson TA. Predictors of statin adherence, switching, and discontinuation in the USAGE survey: understanding the use of statins in America and gaps in patient education. J Clin Lipidol. 2013;7:472–83.
Banach M, Rizzo M, Toth PP, et al. Statin intolerance - an attempt at a unified definition. Position paper from an international lipid expert panel. Arch Med Sci. 2015;11:1–23.
Guyton JR, Bays HE, Grundy SM, Jacobson TA, The National Lipid Association Statin Intolerance Panel. An assessment by the statin intolerance panel: 2014 update. J Clin Lipidol. 2014;8:S72–81.
Romano PS, Roos LL, Jollis JG. Presentation adapting a clinical comorbidity index for use with ICD-9-CM administrative data: differing perspectives. J Clin Epidemiol. 1993;46:1075–9.
Gu Q, Burt VL, Dillon CF, Yoon S. Trends in antihypertensive medication use and blood pressure control among United States adults with hypertension: the National Health and Nutrition Examination Survey, 2001 to 2010. Circulation. 2012;126:2105–14.
Muntner P, Yun H, Sharma P, et al. Ability of low antihypertensive medication adherence to predict statin discontinuation and low statin adherence in patients initiating treatment after a coronary event. Am J Cardiol. 2014;114:826–31.
Choudhry NK, Shrank WH, Levin RL, et al. Measuring concurrent adherence to multiple related medications. Am J Manag Care. 2009;15:457–64.
Arca M, Pigna G. Treating statin-intolerant patients. Diabetes Metab Syndr Obes. 2011;4:155–66.
Bitzur R, Cohen H, Kamari Y, Harats D. Intolerance to statins: mechanisms and management. Diabetes Care. 2013;36(Suppl 2):S325–30.
Fitchett DH, Hegele RA, Verma S. Cardiology patient page. Statin intolerance Circulation. 2015;131:e389–91.
Rosenson RS, Baker SK, Jacobson TA, Kopecky SL, Parker BA, The National Lipid Association's Muscle Safety Expert P. An assessment by the statin muscle safety task force: 2014 update. J Clin Lipidol. 2014;8:S58–71.
Jamal SM, Eisenberg MJ, Christopoulos S. Rhabdomyolysis associated with hydroxymethylglutaryl-coenzyme a reductase inhibitors. Am Heart J. 2004;147:956–65.
Law M, Rudnicka AR. Statin safety: a systematic review. Am J Cardiol. 2006;97:52C–60C.
Ganga HV, Slim HB, Thompson PD. A systematic review of statin-induced muscle problems in clinical trials. Am Heart J. 2014;168:6–15.
Armitage J, Bowman L, Wallendszus K, et al. Intensive lowering of LDL cholesterol with 80 mg versus 20 mg simvastatin daily in 12,064 survivors of myocardial infarction: a double-blind randomised trial. Lancet. 2010;376:1658–69.
de Lemos JA, Blazing MA, Wiviott SD, et al. Early intensive vs a delayed conservative simvastatin strategy in patients with acute coronary syndromes: phase Z of the a to Z trial. JAMA. 2004;292:1307–16.
Cannon CP, Braunwald E, McCabe CH, et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. 2004;350:1495–504.
Harris LJ, Thapa R, Brown M, et al. Clinical and laboratory phenotype of patients experiencing statin intolerance attributable to myalgia. J Clin Lipidol. 2011;5:299–307.
Pedersen TR, Kjekshus J, Berg K, et al. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian simvastatin survival study (4S). Atheroscler Suppl. 2004;5:81–7.
Sacks FM, Pfeffer MA, Moye LA, et al. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events Trial investigators N Engl J Med. 1996;335:1001–9.
The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339:1349–57.
Colantonio LD, Kent ST, Kilgore ML, et al. Agreement between Medicare pharmacy claims, self-report, and medication inventory for assessing lipid-lowering medication use. Pharmacoepidemiol Drug Saf. 2016. doi:10.1002/pds.3970.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The design and conduct of the study, analysis, and interpretation of the data, and preparation of the manuscript, was supported through a research grant from Amgen, Inc. (Thousand Oaks, CA). The academic authors conducted all analyses and maintained the rights to publish this article.
Conflict of Interest
STK received research support from Amgen, Inc. KLM and AM work in the Center for Observational Research at Amgen, Inc. KLM and AM also have stock ownership in Amgen, Inc. MLK, RSR and PM receive research support from Amgen, Inc. RSR also receives research support from Medicines Company, Regeneron and Sanofi, and serves on Advisory Boards for Amgen, Inc., Regeneron and Sanofi. LDC, LH, LC and MCS have no disclosures.
Electronic supplementary material
ESM 1
(DOCX 52 kb)
Rights and permissions
About this article

Cite this article
Colantonio, L.D., Kent, S.T., Huang, L. et al. Algorithms to Identify Statin Intolerance in Medicare Administrative Claim Data. Cardiovasc Drugs Ther 30, 525–533 (2016). https://doi.org/10.1007/s10557-016-6680-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10557-016-6680-3