
Abstract
Quantitative SPECT analysis contributes to the diagnostic and prognostic assessment of coronary artery disease. A novel automated scoring system (heart score view) can provide identical quantitative information to that determined by expert visual analysis. The aim of the present study is to evaluate the prognostic value of the automated SPECT scoring system when applied to stress thallium and resting beta-methyl-iodophenyl pentadecanoic acid (BMIPP) SPECT images. After a preliminary validation of the automated system by comparison with expert visual analyses, outcome data from 151 consecutive patients with suspected or known coronary artery disease without prior myocardial infarction were analyzed using automated SPECT scores on stress thallium and resting BMIPP images. The software quantified abnormalities as summed stress (SSS), summed rest and summed difference scores for stress thallium and as summed BMIPP scores (SBS). Cardiac events occurred over a period of 48 months in 29 (19.2 %) patients with diabetes mellitus, a lower left ventricular ejection fraction (LVEF) and more abnormal scores for thallium and BMIPP. Multivariate predictors of all cardiac events included diabetes mellitus and thallium SSS. The global Chi-square value was significantly increased when SSS was added to the clinical information (diabetes mellitus and LVEF). Negative predictive values of thallium SSS and SBS were almost identical at 84 % for all cardiac events and 98 % for hard cardiac events. Automatically quantified perfusion and BMIPP scores are related to cardiac events and these values can improve the risk stratification of coronary patients particularly when stress thallium imaging is combined with clinical information.
Similar content being viewed by others


Introduction
Together with major clinical risks, stress myocardial perfusion imaging with quantitative assessment has diagnostic and prognostic values for identifying patients at high risk for coronary events [1]. Myocardial perfusion abnormality is visually assessed using summed stress (SSS), summed rest (SRS) and summed difference (SDS) scores in major myocardial perfusion SPECT studies [2–5]. The SPECT scores have been shown to be related to fatal or non-fatal cardiac events [2–5]. The ACNC guidelines recommend the semi-quantitative assessment and further interpretation of myocardial perfusion imaging by experts [6]. However, SPECT analysis is not necessarily a routine procedure in clinical practice at community-based facilities because of a shortage of experts. Standardization of visual assessment requires appropriate training and much experience. Thus, we developed a PC-operated automated scoring system for myocardial SPECT imaging (heart score view software). We previously [7] validated the high reproducibility and accuracy of the automated scoring system for quantitative SPECT analysis when compared with visual expert assessment. Summed SPECT scores were nearly identical between the automated and expert visual assessments on Bland–Altman analysis [7].
Another imaging technique that can be used for the diagnostic and prognostic assessment of coronary patients without stress testing is myocardial fatty acid imaging with 123I-beta-methyl-iodophenyl pentadecanoic acid (BMIPP) [8–11]. Myocardial BMIPP imaging has diagnostic and prognostic value for acute and chronic stable coronary artery diseases [8–11]. The automated SPECT software is also applicable to myocardial SPECT imaging with BMIPP. Our earlier study [8] compared the prognostic value of myocardial BMIPP with that of stress thallium imaging in patients with stable coronary artery disease using standard expert visual analysis. However, whether the automated scoring software has prognostic value for myocardial perfusion and BMIPP images remained unknown. Thus, the present study evaluates the prognostic value of the automated SPECT scoring system when applied to stress thallium and resting BMIPP SPECT images of coronary artery disease from this viewpoint. A preliminary study compared automated SPECT scores with semi-quantitative visual scores for prognostic value among 50 patients with coronary disease. This is a statistically acceptable number of patients for analysis using receiver operating characteristics (ROC) curves [12]. Subsequently, the outcomes of all enrolled patients were analyzed using the automated scoring system.
Methods
Patient selection
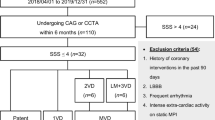
We retrospectively analyzed data from 151 of 196 consecutive patients with suspected or stable coronary artery disease who were originally registered in our database based on the following entry criteria: no history of myocardial infarction, images obtained from resting BMIPP and subsequent stress thallium SPECT imaging, and regular follow up [8]. Data from 45 patients were deleted from outcome analysis based on the following exclusion criteria: loss during follow-up, unknown cause of death, death due to malignancy, coronary revascularization within 3 months of myocardial SPECT imaging and loss of original digital SPECT data files. The Ethics Committee of Shin-Nittetsu Muroran General Hospital approved the study protocol.
Patient follow-up
The subjects underwent resting BMIPP imaging followed by stress thallium imaging at an interval of 15.8 ± 13.5 (range 2–57) days using a standard protocol and were then followed up to the end points of cardiac death, non-fatal myocardial infarction, late revascularization and hospital admission due to recurrent refractory angina or congestive heart failure. Cardiac death was defined as death attributable to congestive heart failure, myocardial infarction or cardiac arrest or sudden cardiac death. Hard events were defined as cardiac death, non-fatal myocardial infarction and admission due to heart failure.
Automated quantitative system using heart score view software
We developed the automated software, heart score view, which is a scoring system that is applicable to any type of myocardial SPECT imaging using a standard Windows PC. The automated quantitative method was recently validated by comparison with expert-visual assessment [7]. The software generates a polar-map from myocardial SPECT images then mean % tracer uptake in each segment is automatically scored from normal (0) to absent (4) using a 5-point model based on ASNC guidelines [13]. Thresholds of % tracer uptake for scoring are described elsewhere [7]. Values for SSS, SRS and SDS on stress and rest thallium myocardial perfusion images and summed BMIPP score (SBS) on rest fatty acid image were calculated by summing 17-segment scores on SPECT polar-map images to globally assess SPECT abnormalities. Visual-expert analysis and automated scoring were compared using SPECT images from 50 randomly selected patients with coronary artery disease who were among the 151 patients as a technical validation before starting this outcome study.
Statistical analysis
Values are expressed as means ± SD. Means of continuous variables were compared using an unpaired t-test and categorical data were analyzed using the χ2 test. Cardiac event-free survival rates were analyzed using Kaplan–Meier analysis and compared using the log-rank test. Univariable analysis and a subsequent multivariable Cox hazards proportional regression model were applied to identify independent predictive parameters for cardiac events with a hazard ratio and 95 % confidence intervals (CI). Areas under the curve (AUC) among the summed scores were compared using ROC curve analysis. All data were statistically analyzed using MedCalc software, version 9.4.2.0 (Mariakerke, Belgium). A p value below 0.05 was considered significant.
Results
Preliminary comparison of visual and automated scores in prognosis
Thallium SSS were higher in the non-event group and the AUC in the ROC curve analysis was smaller when assessed by automated SPECT than by expert visual scoring (Tables 1, 2). However, automated SPECT scoring significantly distinguished the event from the non-event group as well as expert visual analysis.
Figure 1 shows that thallium and BMIPP cut-off values derived from the automated scoring system differentiated between high- and low-risk patients as did those determined by expert visual analysis.

Preliminary comparison of event-free curves between visual expert (left panels) and automated SPECT (right panels) analyses using cut-off values of SSS and SBS in 50 randomly selected coronary patients
Main outcome study
Twenty-nine cardiac events (7 hard and 22 soft) documented in the 151 patients during a mean follow-up of 48 months were analyzed. One patient had sudden cardiac death, one had cardiac death due to heart failure, two had congestive heart failure, three had non-fatal acute myocardial infarction, eight underwent coronary revascularization at a later stage, and 14 had recurrent angina pectoris requiring hospitalization. Left ventricular ejection fraction (LVEF) was significantly lower and the rate of complication with diabetes mellitus was higher in the group with, than without cardiac events (Table 3). Automated SPECT scores were significantly greater in the group with, than without cardiac events. Likewise, except for SRS, abnormal SPECT scores of ≥4 for thallium SSS, thallium SDS and SBS were more frequent in the group with cardiac events. These results were consistent when only hard cardiac events were considered in the comparison (Table 4).
Time dependent analyses using abnormal SPECT scores
Event-free curves were created using the threshold SPECT score of ≥4 that has been established from a 17-segment model as being abnormal [14–19]. Patient subgroups with abnormal scores had significantly lower event free rates for SSS, SDS and SBS when compared with each counterpart for all cardiac events (Fig. 2) and for hard cardiac events (Fig. 3).

Event-free curves for all cardiac events using SSS, SRS, summed difference SDS and SBS Event-free rates significantly differ between two groups divided by SSS, SDS and SBS but not by SRS. Event-free rates at 2,500 days were 62 and 80 % for patients with SSS ≥ 4 and <4, respectively (a), 77 and 75 % with SRS ≥ 4 and <4, respectively (b), 55 and 80 % with SDS ≥ 4 and <4, respectively (c) and 52 and 82 % with SBS ≥ 4 and <4, respectively (d)

Event-free curves for hard cardiac events using SSS, SRS, SDS and SBS Event-free rates significantly differ between two groups divided by SSS, SDS and SBS but not by SRS. Event-free rates at 2,500 days were 82 and 98 % with SSS ≥ 4 and <4, respectively (a), 85 and 94 % with SRS ≥ 4 and <4, respectively (b), 80 and 97 % for patients with SDS ≥ 4 and <4, respectively (c) and 80 and 97 % with SBS ≥ 4 and <4, respectively (d)
Univariable and multivariable analyses
Univariable Cox analysis revealed LVEF, diabetes mellitus, SSS, SDS and SBS as significant predictors of all cardiac events (Table 5). When four variables identified as clearly significant were included, multivariable Cox analysis uncovered that diabetes mellitus and SSS as significant independent predictors of all cardiac events, whereas LVEF and SBS were not (Table 6). The prognostic value (global Chi-square value) significantly (p < 0.01) increased from 21.5 to 31.9 when SSS was added to the clinical information about diabetes mellitus and LVEF.
Correlation between stress thallium and BMIPP scores in automated SPECT scoring system
The SBS and SSS significantly correlated in all patients (r = 0.644, p < 0.001), as well as in those with (r = 0.770, p < 0.001) and without (r = 0.403, p < 0.001) cardiac events (Fig. 4).

Correlations between SSS and SBS obtained using automated SPECT scoring system
Positive and negative predictive values
Figure 5 compares positive and negative predictive values for overall and hard cardiac events when abnormal SSS and SBS were defined as ≥4. Positive predictive values of the abnormal scores were low but increased by combination with SSS and SBS. On the other hand, the negative predictive values of normal SSS and SBS were high and identical without combination at essentially 84 and 98 % for all and hard cardiac events, respectively.

Positive (white columns) and negative (black columns) predictive values for all (a) and hard (b) cardiac events using SSS for stress thallium images and/or SBS. Abnormal SSS and SBS are both defined as ≥4; normal scores are defined as ≤3
Case presentation
Figure 6 shows two typical polar-map displays and heart score view maps of rest BMIPP, stress and rest thallium images. A 77-year-old woman with hypertension and diabetes mellitus underwent rest BMIPP followed by exercise-stress thallium imaging due to having suspected stable coronary artery disease. The automated heart score view scores were 6, 10 and 3 for the SBS, SSS and SRS, respectively, indicating an intermediate risk for coronary events. Ninety days later, she underwent emergency percutaneous coronary interventional therapy because of acute coronary syndrome.

SPECT, polar and heart score view maps of stress and rest thallium myocardial perfusion and rest BMIPP images. a Suspected stable coronary artery disease in a 77-year-old hypertensive, diabetic woman. Automated scoring system scored 6, 10 and 3 for BMIPP, stress and rest thallium, respectively, indicating intermediate risk for coronary events. Ninety days later, she underwent emergency percutaneous coronary intervention to treat acute coronary syndrome. b Suspected coronary artery disease in a 61-year-old hypertensive, dyslipidemic man with a smoking history. Automated scoring system scored 0, 2 and 0 for BMIPP, stress and rest thallium images, respectively, indicating low risk for cardiac events. He has remained free of cardiac events for 4 years
A 61-year-old man with a history of smoking, hypertension and dyslipidemia underwent rest BMIPP followed by exercise-stress thallium imaging due to suspected angina pectoris. The automated heart score view system scored 0, 2 and 0 for BMIPP, stress and rest thallium, respectively, indicating a low risk for cardiac events. This patient has remained free of cardiac events for 4 years.
Discussion
The present findings show that automated SPECT analysis of stress thallium and fatty acid metabolism images can provide reliable, quantitative and additive information for the risk-stratification of patients with coronary artery disease based on high negative predictive values alone and in combination with conventional clinical information such as diabetes mellitus and/or left ventricular function.
Clinical implications of automated quantitative analysis
Following our previous validation study [7], the current outcome study clarified the prognostic value of automated risk-assessment system using heart score view software in stress thallium and resting metabolic SPECT images in patients with stable coronary artery disease. This is attributable to its high reproducibility, objective and quantitative nature. This PC-operated system can serve as a routine clinical tool for risk stratification, for monitoring therapeutic effects and for creation of large-scale database of an outcome study. Berman et al. [20] reported another type of computer-assisted quantitative analysis using a normal circumferential profile curve in myocardial perfusion SPECT imaging. Although the automated method also used a 5-point scoring system for comparison with standard visual expert analysis, the automated method was not completely identical to the visual scoring system. Expert visual analysis with a 5-point, 17-segment model [1–4] uses three representative short-axis slices at basal, mid-ventricular and apical portions and one vertical-long axis slice. The present automated scoring system uses all short-axis slices derived from SPECT images and count data (% tracer uptake) on polar maps for scoring. In addition, a SPECT abnormality is defined by comparison with a normal SPECT database. Thus, the presented method can provide more global, objective and quantitative information about SPECT images than standard visual analysis. Nevertheless, the present study showed that the prognostic value of the automated scoring system of stress thallium and resting BMIPP SPECT images is as good as that of standard visual analysis.
Prognostic values of stress thallium and fatty acid uptake abnormalities
As previously demonstrated by visual expert analysis, multivariable analysis in the present study confirmed SSS and diabetes mellitus as powerful independent prognostic determinants. Although SBS and LVEF were significant, they were not necessarily independent variables. Studies including some from Japan have already established the prognostic implications of diabetes mellitus in coronary artery disease [3, 8–10]. Several mechanisms might be involved in the independent correlation between diabetes mellitus and cardiac events found in the present study. Diabetes mellitus is a powerful atherogenic factor that induces or augments coronary sclerosis. The capacity to utilize glucose and fatty acid to generate energy in the diabetic myocardium is reduced, which might lead to cardiac dysfunction. Diabetes mellitus also impairs endothelial vasodilator action and kidney function, which has been recognized as an important determinant of prognosis in cardiac disease [21, 22]. The prognostic power of BMIPP data was not necessarily additive in the present study when stress thallium information (SSS) was included. The discrepant findings of the prognostic value of myocardial BMIPP imaging between the present and our previous [8] study might be attributable to the use of different scoring algorithms. Nevertheless, the present findings clarified that myocardial fatty acid metabolism imaging alone can provide prognostic information without a stress approach. The myocardium produces large amounts of high-energy phosphates by consuming a large amount of oxygen, while it is very vulnerable to ATP depletion [23]. The myocardium can sustain impaired fatty acid uptake for several days to months after acute ischemic events [24–27] or under prolonged ischemia [28–30]. Such metabolic stunning or ischemic memory assessed by BMIPP imaging corresponds to an ischemic risk area that could be responsible for future cardiac events [31, 32]. The present results also revealed that normal SSS and normal SBS had equally high negative predictive values (almost 98 %) for hard cardiac events. Thus, resting myocardial BMIPP values provide additive prognostic information not only for clinically high-risk patients with diabetes mellitus and/or left ventricular dysfunction but also for identifying low-risk patients, particularly as an alternative imaging strategy when stress myocardial perfusion is contraindicated.
Study limitations
Compared with visual expert analysis in this study, the automated scoring system tended to overestimate thallium SSS and SBS in patients without cardiac events. The automated scoring system in the preliminary study overestimated the SSS in 5 of 37 patients without cardiac events who had heterogeneous hypertrophy or high activity. The discrepancy between the two methods might be due to differences between the scoring systems. The automated system uses all short-axis slices for scoring and quantifies using percent tracer uptake that reflects tracer activity relative to a maximal data point among short-axis slices. Nevertheless, the automated scoring system is unlikely to underestimate the probability of cardiac events in high-risk patients. Automated SPECT analysis is applicable to other types of SPECT imaging. A recent comparison with visual analysis showed that the automated software analysis is technically applicable to 99mTc-tetrofosmin stress myocardial SPECT [33]. Finally, this study retrospectively analyzed myocardial SPECT data from patients without prior myocardial infarction. A future prospective study of a large population is needed to confirm prognostic value of the automated software for the myocardial SPECT imaging of patients with and without prior myocardial infarction.
Conclusions
Automatically quantified myocardial SPECT abnormality using heart score view software can identify patients at high-risk for coronary artery diseases with high positive and negative predictive values particularly when applied to stress thallium imaging. The automated technique contributes to better prognosis assessment by myocardial SPECT imaging when combined with clinical information such as diabetes mellitus and/or left ventricular function.
References
Klocke FJ, Baird MG, Lorell BH, Bateman TM, Messer JV, Berman DS et al (2003) ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging–executive summary: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (ACC/AHA/ASNC Committee to revise the 1995 guidelines for the clinical use of cardiac radionuclide imaging). Circulation 108:1404–1418
Hachamovitch R, Berman DS, Shaw LJ, Kiat H, Cohen I, Cabico JA et al (1998) Incremental prognostic value of myocardial perfusion single photon emission computed tomography for the prediction of cardiac death: differential stratification for risk of cardiac death and myocardial infarction. Circulation 97:535–543
Nishimura T, Nakajima K, Kusuoka H, Yamashina A, Nishimura S (2008) Prognostic study of risk stratification among Japanese patients with ischemic heart disease using gated myocardial perfusion SPECT: J-ACCESS study. Eur J Nucl Mol Imaging 35:319–328
Nakata T, Hashimoto A, Wakabayashi T, Kusuoka H, Nishimura T (2009) Prediction of new-onset refractory congestive heart failure using stress/rest gated perfusion SPECT imaging in patients with known or suspected coronary artery disease: Sub-analysis of the J-ACCESS. J Am Coll Cardiol Imaging 2:1393–1400
Kato M, Matsumoto N, Nakano Y, Suzuki Y, Yoda S, Kasama S et al (2011) Combined assessment of myocardial perfusion and function by ECG-gated myocardial perfusion single-photon emission computed tomography for the prediction of future cardiac patients with type 2 diabetes mellitus. Circ J 75:376–382
Holly TA, Abbot BG, Al-Mallah M, Calnon DA, Cohen MC, Difilippo FP et al (2010) ASNC imaging guidelines for nuclear cardiology procedures: single photon-emission computed tomography. J Nucl Cardiol. http://www.asnc.org/imageuploads/ImagingGuidelineSPECTJune2010.pdf
Yoshinaga K, Matsuki T, Hashimoto A, Tsukamoto K, Nakata T, Tamaki N (2011) Validation of automated quantification of myocardial perfusion and fatty acid metabolism abnormalities on SPECT images. Circ J 75:2187–2195
Matsuki T, Tamaki N, Nakata T, Doi A, Takahashi H, Iwata M et al (2004) Prognostic value of fatty acid imaging in patients with angina pectoris without prior infarction: comparison with stress thallium imaging. Eur J Nucl Mol Imaging 31:1585–1591
Nakata T, Kobayashi T, Tamaki N, Kobayashi H, Wakabayashi T, Shimoshige S, Oh-hori K, Hamabe K, Hirasawa K, Matsuki T, Shogase T, Furudate M, Shimamoto K (2000) Prognostic values of impaired myocardial fatty acid uptake in patients with acute myocardial infarction. Nucl Med Comm 21:897–906
Chikamori T, Fujita H, Nanasato M, Toba M, Nishimura T (2005) Prognostic value of 1-123-(p-iodophenyl)-3-(R,S) methylpentadecanoic acid myocardial imaging in patients with known or suspected coronary artery disease. J Nucl Cardiol 12:172–178
Nishimura M, Tsukamoto K, Hasebe N, Tamaki N, Kikuchi K, Ono T (2008) Prediction of cardiac death in hemodialysis patients by myocardial fatty acid imaging. J Am Coll Cardiol 51:139–145
Obuchowski NA, Lieber ML, Wians FH Jr (2004) ROC curves in clinical chemistry: uses, misuses, and possible solutions. Clin Chem 50:1118–1125
Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK et al (2002) Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart: a statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation 105:539–542
Berman DS, Kang X, Tamarappoo B, Wolak A, Hayes SW, Nakazato R et al (2009) Stress Thallium-201/rest technetium-99m sequential dual isotope high-speed myocardial perfusion imaging. J Am Coll Cardiol Imaging 2:273–282
van Werkhoven JM, Schuijf JD, Gaemperli O, Wouter Jukema J, Boersma E, Wijns W et al (2009) Prognostic value of multislice computed tomography and gated single-photon emission computed tomography in patients with suspected coronary artery disease. J Am Coll Cardiol 53:623–632
Nakazato R, Moroi M (2006) Prognostic value of stress myocardial perfusion imaging in patients with mildly impaired systolic left ventricular function or left ventricular asynergy without chest pain but with suspected coronary artery disease. Circ J 70:762–767
Shin JH, Pokharna HK, Williams KA, Mehta R, Ward RP (2009) SPECT myocardial perfusion imaging with prone-only acquisitions: correlation with coronary angiography. J Nucl Cardiol 16:590–596
Gera N, Taillon LA, Ward RP (2009) Usefulness of abnormal heart rate recovery on exercise stress testing to predict high-risk findings on single-photon emission computed tomography myocardial perfusion imaging in men. Am J Cardiol 103:611–614
Jain D, Lessig H, Patel R, Sandler L, Weiland F, Edell SL et al (2009) Influence of 99mTc-Tetrofosmin SPECT myocardial perfusion imaging on the prediction of future adverse cardiac events. J Nucl Cardiol 16:540–548
Berman DS, Kang X, Gransar H, Gerlach J, Friedman JD, Hayes SW et al (2009) Quantitative assessment of myocardial perfusion abnormality on SPECT myocardial perfusion imaging is more reproducible than expert visual analysis. J Nucl Cardiol 16:45–53
Grundy S, Howard B, Smith SJ, Eckel R, Redberg R, Bonow RO (2002) Prevention conference VI: diabetes and cardiovascular disease: executive summary: conference proceeding for healthcare professionals from a special writing group of the American Heart Association. Circulation 105:2231–2239
Marso SP, Miller T, Rutherford BD, Gibbons RJ, Qureshi M, Kalynych A et al (2007) Comparison of myocardial reperfusion in patients undergoing percutaneous coronary intervention in ST-segment elevation acute myocardial infarction with versus without diabetes mellitus (from the EMERALD trial). Am J Cardiol 100:206–210
Fujibayashi Y, Yonekura Y, Takemura Y, Wada K, Matsumoto K, Tamaki N, Yamamoto K, Konishi J, Yokoyama A (1990) Myocardial accumulation of iodinated beta-methyl-branched fatty acid analogue, iodine-125-15-(p-iodophenyl)-3-(R,S) methylpentadecanoic acid (BMIPP), in relation to ATP concentration. J Nucl Med 31:1818–1822
Hashimoto A, Nakata T, Tsuchihashi K, Tanaka S, Fujimori K, Iimura O (1996) Post-ischemic functional recovery and BMIPP uptake following primary percutaneous transluminal coronary angioplasty in acute myocardial infarction. Am J Cardiol 77:25–30
Nakata T, Hashimoto A, Kobayashi H, Miyamoto K, Tsuchihashi K, Miura T, Shimamoto K (1998) Outcome significance of Tl-201 and I-123 BMIPP perfusion- metabolism mismatch in pre-infarction angina. J Nucl Med 39:1492–1499
Nakata T, Hashimoto A, Eguchi M (1999) Cardiac BMIPP imaging in acute myocardial infarction. Int J Cardiac Imaging 14:21–26
Kawai Y, Tsukamoto E, Nozaki Y, Morita K, Sakurai M, Tamaki N (2001) Significance of reduced uptake of iodinated fatty acid analogue for the evaluation of patients with acute chest pain. J Am Coll Cardiol 38:1888–1894
Kontos MC, Dilsizian V, Weiland F, DePuey G, Mahmarian JJ, Iskandrian AE et al (2010) Iodofiltic acid I 123 (BMIPP) fatty acid imaging improves initial diagnosis in emergency department patients with suspected acute coronary syndromes: a multicenter trial. J Am Coll Cardiol 56:290–299
Taki J, Nakajima K, Matsunari I, Bunko H, Takata S, Kawasuji M et al (1997) Assessment of improvement of myocardial fatty acid uptake and function after revascularization using iodine-123-BMIPP. J Nucl Med 38:1503–1510
Dilsizian V, Bateman TM, Bergmann SR, Des Prez R, Magram MY, Goodbody AE et al (2005) Metabolic imaging with beta-methyl-p-[(123)I]-iodophenyl- pentadecanoic acid identifies ischemic memory after demand ischemia. Circulation 112:2169–2174
Kawai Y, Tsukamoto E, Nozaki Y, Kishino K, Kohya T, Tamaki N (1998) Use of 123I-BMIPP single-photon emission tomography to estimate areas at risk following successful revascularization in patients with acute myocardial infarction. Eur J Nucl Med 25:1390–1395
Hashimoto A, Nakata T, Tamaki N, Kobayashi T, Matsuki T, Shogase T et al (2006) Serial alterations and prognostic implications of myocardial perfusion and fatty aid metabolism in patients with acute myocardial infarction. Circ J 70:1466–1474
Nakajima K, Matsuo S, Okuda K, Wakabayashi H, Tsukamoto K, Nishimura T (2011) Estimation of cardiac event risk by gated myocardial perfusion imaging and quantitative scoring methods based on a multi-center J-ACCESS database. Circ J 75:2417–2423
Acknowledgments
The authors thank Mr. Masatsuyo Takano, RT, and Ms. Maki Ogura, RT for technical expertise and Ms. Norma Foster for critical reading of the manuscript.
Conflict on interest
All authors declare that they have no conflict of interest regarding this study.
Open Access
This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Nakata, T., Hashimoto, A., Matsuki, T. et al. Prognostic value of automated SPECT scoring system for coronary artery disease in stress myocardial perfusion and fatty acid metabolism imaging. Int J Cardiovasc Imaging 29, 253–262 (2013). https://doi.org/10.1007/s10554-012-0069-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-012-0069-6