
Abstract
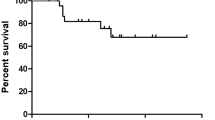
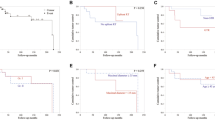
Skull base chondrosarcomas are rare tumors and individual experience with their management is limited. We present a series of such tumors treated at our institution. Particular attention was paid to their extension pattern, choice of surgical approach, and outcome. Twenty-five patients were operated consecutively over a period of 19 years. Their clinical presentation, radiological features, surgical treatment, early and late treatment outcome, as well as survival rate were analyzed. The most frequent initial symptom was abducent palsy. The typical bone destruction of the petrous apex was found in 83%. Chondrosarcomas extended in 92% to the posterior cranial fossa. Total number of surgeries was 39. The operative approach was tailored to each case. The retrosigmoid approach was used in 30.8%, the pterional in 23%, and the transethmoid in 15.4%. Total tumor removal was achieved in 19 of the surgeries. New neurological deficits immediately after surgery appeared in 33.3%. The perioperative mortality was 0%. The average Karnofsky performance score at last follow-up was 91%, and 5- and 10-year survival rates were 95%. Individually tailored approach in skull base chondrosarcomas allows radical removal with low morbidity rates and without mortality. Given the good long-term prognosis, surgical treatment should not deteriorate significantly patients’ quality of life.





Similar content being viewed by others

References
Burkey BB, Hoffman HT, Baker SR, Thornton AF, McClatchey KD (1990) Chondrosarcoma of the head and neck. Laryngoscope 100:1301–1305
Castro JR, Linstadt DE, Bahary JP, Petti PL, Daftari I, Collier JMGutin PH, Gauger G, Phillips TL (1994) Experience in charged particle irradiation of tumors of the skull base: 1977–1992. Int J Radiat Oncol Biol Phys 29:647–655
Crockard HA, Cheeseman A, Steel T, Revesz T, Holton JL, Plowman N, Singh A, Crossman J (2001) A multidisciplinary team approach to skull base chondrosarcomas. J Neurosurg 95:184–189
Debus J, SchulzErtner D, Schad L, Essig M, Rhein B, Thillmann CO, Wannenmacher M (2000) Stereotactic fractionated radiotherapy for chordomas and chondrosarcomas of the skull base. Int J Radiat Oncol Biol Phys 47:591–596
Evans HL, Ayala AG, Romsdahl MM (1977) Prognostic factors in chondrosarcoma of bone: a clinicopathologic analysis with emphasis on histologic grading. Cancer 40:818–831
Gay E, Sekhar LN, Rubinstein E, Wright DC, Sen C, Janecka IP, Snyderman CH (1995) Chordomas and chondrosarcomas of the cranial base: results and follow-up of 60 patients. Neurosurgery 36:887–896
Gwak HS, Yoo HJ, Youn SM, Chang U, Lee DH, Yoo SY, Rhee CH (2006) Hypofractionated stereotactic radiation therapy for skull base and upper cervical chordoma and chondrosarcoma: preliminary results. Stereotact Funct Neurosurg 83:233–243
Hassounah M, al Mefty O, Athar M, Jinkins JR, Fox JL (1985) Primary cranial and intracranial chondrosarcoma, a survey. Acta Neurochir 78:123–132
Heffelfinger MJ, Dahlin DC, MacCarty CS, Beabout JW (1973) Chordomas and cartilaginous tumors at the skull base. Cancer 32:410–420
Hug EB, Slater JD (2000) Proton radiation therapy for chordomas and chondrosarcomas of the skull base. Neurosurg Clin N Am 11:627–638
Kaplan EL, Meier P (1958) Nonparametric estimation from incomplete observations. J Am Stat Assoc 53:457–481
Karnofsky DA, Burchenal JH, Armistead GC, Southam CM, Bernstein JL, Craver LF, Rhoads CP (1951) Triethylene melamine in the treatment of neoplastic disease. Arch Intern Med 87:477–516
Kondziolka D, Lunsford LD, Flickinger JC (1991) The role of radiosurgery in the management of chordoma and chondrosarcoma of the cranial base. Neurosurgery 29:38–45
Korten AG, Terberg HJ, Spincemaille GH, Vanderlaan RT, Vandewel AM (1998) Intracranial chondrosarcoma: review of the literature and report of 15 cases. J Neurol Neurosurg Psychiatry 65:88–92
Krishnan S, Foote RL, Brown PD, Pollock BE, Link MJ, Garces YI (2005) Radiosurgery for cranial base chordomas and chondrosarcomas. Neurosurgery 56:777–784
Lanzino G, Dumont AS, Lopes BS, Laws ER Jr (2001) Skull base chordomas: overview of disease, management options, and outcome. Neurosurg Focus 10(3):E12
Meyers SP, Hirsch WL Jr, Curtin HD, Barnes L, Sekhar LN, Sen C (1992) Chondrosarcomas of the skull base: MR imaging features. Radiology 184:103–108
Munzenrider JE, Liebsch NJ (1999) Proton therapy for tumors of the skull base. Strahlenther Onkol 175:57–63
Muthukumar N, Kondziolka D, Lunsford LD, Flickinger JC (1998) Stereotactic radiosurgery for chordoma and chondrosarcoma: further experiences. Int J Radiat Oncol Biol Phys 41:387–392
Neff B, Sataloff RT, Storey L, Hawkshaw M, Spiegel JR (2002) Chondrosarcoma of the skull base. Laryngoscope 112:134–139
Oghalai JS, Buxbaum JL, Jackler RK, McDermott MW (2005) Skull base chondrosarkoma originating from the petroclival junction. Otol Neurotol 5:1052–1060
Rosenberg AE, Rosenberg AE, Nielsen GP, Keel SB, Renard LG, Fitzek MM, Munzenrider JE, Liebsch NJ (1999) Chondrosarcoma of the base of the skull: a clinicopathologic study of 200 cases with emphasis on its distinction from chordoma. Am J Surg Pathol 23:1370–1378
Samii M, Draf W (1988) Surgery of the clivus in surgery of the skull base. Springer, Berlin, pp 432–460
Samii M, Knosp E (1992) Temporal approaches. In: Samii M, Knosp E (eds) Approaches to the clivus—approaches to no man’s land. Springer, Berlin, pp 83–140
Schulz-Ertner D, Nikoghosyan A, Didinger B, Debus J (2004) Carbon ion radiation therapy for chordomas and low grade chondrosarcomas—current status of the clinical trials at GSI. Radiother Oncol 73:S53–S56
Sekhar LN, Pranatartiharan R, Chanda A, Wright DC (2001) Chordomas and chondrosarcomas of the skull base: results and complications of surgical management. Neurosurg Focus 10(3):E2
Volpe NJ, Liebsch NJ, Munzenrider JE, Lessell S (1993) Neuro-ophthalmologic findings in chordoma and chondrosarcoma of the skull base. Am J Ophthalmol 115:97–104
Wanebo JE, Bristol RE, Porter RR, Coons SW, Spetzler RF (2006) Management of cranial base chondrosarcomas. Neurosurgery 58:249–255
Weber DC, Rutz HP, Pedroni ES, Bolsi A, Timmermann B, Verwey J, Lomax AJ, Goitein G (2005) Results of spot-scanning proton radiation therapy for chordoma and chondrosarcoma of the skull base: the Paul Scherrer Institut experience. Int J Radiat Oncol Biol Phys 63:401–409
Werner J (1992) Biomathematik und Medizinische Statistik. Urban & Schwarzenberg, München, pp 228–231
Yasargil MG, Fox JL (1975) The microsurgical approach to intracranial aneurysms. Surg Neurol 3:7–14
Author information
Authors and Affiliations
Corresponding author
Additional information
Comments
Damianos Sakas, Athens, Greece
This report describes a reasonably big series of patients with a rare and difficult to manage tumor, of whom the great majority was managed by the same surgeon over a time period of 19 years. It is noteworthy that the authors conclude that neither the radicality of tumor resection nor the adjunct radiotherapy was found to affect the survival rates. Due to their histopathological origin, i.e., from tissue layers covering the cranial base, these tumors frequently not only displace or distort critical neurovascular structures but encase them for a considerable length. This makes radical excision of chondrosarcomas very difficult. It is important that the authors also found that the most important variables that have predictive value with respect to a less satisfactory outcome are the large tumor size and the tumor’s proximity to critical neurovascular structures. Based on the senior authors long-lasting experience, the contribution of the article in the relevant literature would be much greater if useful surgical tips on the management of these challenging tumors were provided. Nevertheless, the report of these patients treated by a distinguished surgeon, who is well-known for his highly successful radical surgical philosophy, is very useful; it confirms, with respect to this particular tumor, that the right approach is the more cautious one, namely the approach of safe cytoreduction, i.e., individualized subtotal resection combined with radiotherapy.
Takeshi Mikami, Tomakomai, Japan
In this report, the authors present a series of patients with chondrosarcoma of the skull base. Chondrosarcoma originating along the skull base is extremely rare, so this case series is exceptionally valuable.
The surgical results and long-term follow-up prognosis are extremely good, and the authors have even mentioned the correlation between extension pattern and surgical approach. This paper will allow readers to learn about surgical strategy and long-term management from experienced surgeons.
In this study, the authors have not included any conclusions on radiotherapy that were based on data, yet some of their cases must have received some benefit from radiotherapy. This leaves the door open for further developments in the management of chondrosarcoma, specifically in the use of multimodality treatment.
Rights and permissions
About this article
Cite this article
Samii, A., Gerganov, V., Herold, C. et al. Surgical treatment of skull base chondrosarcomas. Neurosurg Rev 32, 67–75 (2009). https://doi.org/10.1007/s10143-008-0170-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-008-0170-4