
Abstract
Rapid identification and antimicrobial susceptibility profiling of the bacteria in blood cultures can result in clinical and financial benefits. Addition of saponin to the fluid from blood culture bottles promotes the recovery of the bacteria and thus may shorten the turnaround time of the microbiological analyses. In this study we compared the identification and susceptibility profiles of saponin-treated and untreated (standard method) blood cultures monomicrobial for Gram-positive cocci using Vitek 2. We concordantly identified 49 (89%) of 55 monobacterial cultures using the results with the standard method as reference. Complete categorical agreement between the susceptibility profiles with the new and the standard method was found for 26 (53%) of 49 isolates, while discrepancies were seen for 23 (47%) cultures. E-tests indicated that the new method resulted in a correct susceptibility profile for 8 (35%) of these 23 blood cultures. Therefore, 34 (69%) of 49 cultures showed a concordant/correct susceptibility profile for all antimicrobials with an overall error rate of 2.3%. Thus, addition of saponin to the fluid from blood culture bottles of the Bactec 9240 leads to the rapid (results available ≥12 hours earlier) and reliable identification and susceptibility profiling of Gram-positive cocci in blood cultures with Vitek 2.
Similar content being viewed by others


Introduction
Bloodstream infections are a major cause of morbidity and mortality in critically ill patients. Approximately 250,000 cases of bloodstream infections occur in the United States per annum [1, 2]. Although studies of bloodstream infections are divergent and may involve specific and non-specific patient populations, several trends including an increasing incidence, a changing microbiology and a sustained high mortality [3] are apparent. Regarding the changing nature of the causative agents of bloodstream infections, Gram-negative bacteria were common in the 1970s, while nowadays Gram-positive bacteria are the predominant causative agents [4, 5]. Furthermore, the growing proportion of isolates exhibiting antimicrobial resistance is of concern.
Identification of the bacteria in blood samples and establishment of their antimicrobial susceptibility profile are very important for the clinician to determine whether a febrile episode in a patient is suggestive of an infectious or a non-infectious cause and whether to continue with the chosen empirical therapy or to streamline the antibiotic treatment to the susceptibility profile of the pathogen. Obviously, rapid and reliable identification of the pathogen at an early stage of the disease is critical for a favourable outcome for the patient [6–8]. The methodology currently used, further referred to as the standard method, to detect the infectious agent in positive blood cultures involves an overnight agar medium subculture from positive blood culture bottles to recover a sufficient bacterial inoculum size to prepare standard suspensions for species identification and antimicrobial susceptibility profiling with an automated system, e.g. the Vitek 2 system. In order to reduce the turnaround time of the microbiological analyses, studies have been performed in which specially processed fluid from a positive blood culture is directly inoculated into automated systems for the identification and antimicrobial susceptibility profiling of bacteria [9–17]. The results of these studies were favourable for Gram-negative bacteria with correct identification at the species level ranging from 62% to 93% [9–11, 13–15] depending on the combination of automated systems used. Unfortunately, direct inoculation of fluid from blood culture containing Gram-positive cocci into these automated systems yielded unsatisfactory results [9–11]. However, detergents may improve the recovery of bacteria from positive blood cultures by releasing intracellular bacteria from patients’ phagocytes [18]. Indeed, we recently reported that addition of saponin to the fluid of blood culture bottles containing Gram-positive cocci prior to inoculation into the Phoenix panels led to rapid and reliable identification and antimicrobial susceptibility profiling of these bacteria [19]. Based on the above considerations, a prospective study was undertaken to determine whether addition of saponin to the fluid from positive blood culture bottles from the Bactec 9240 before inoculation of the appropriate Vitek 2 cards leads to the rapid and reliable identification and susceptibility profiling of Gram-positive cocci in blood samples.
Materials and methods
Blood samples
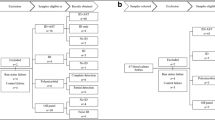
Blood samples were collected at the Unità Operativa di Microbiologia Universitaria, Azienda Ospedaliera Universitaria Pisana, Pisa, Italy. Samples were obtained from patients admitted to the Liver Transplant Intensive Care Unit, Haematological and Pediatric Haematological wards, Neonatology ward, and the Burn Care Center. Each sample was inoculated into a blood culture bottle (Plus Aerobic/F [product no. 442192], Plus Anaerobic/F [product no. 442193], or Peds Plus F [product no. 442194]; Becton Dickinson & Co, Milan, Italy) and transferred to the Bactec 9240 instrument (software version V4.70A) for monitoring the bacterial growth. Per patient, every first positive blood culture containing Gram-positive cocci that appeared monomicrobial in the Gram stain was included in the study. Overall, 64 blood cultures from different patients with Gram-positive cocci were investigated. After subculturing onto blood agar, salt mannitol agar, and McConkey agar plates (BD), seven of these samples proved to be polymicrobic and were therefore excluded from this study. Together, 57 monomicrobial blood cultures containing Gram-positive cocci were evaluated. Fifty-five (97%) isolates were correctly identified by the standard method. Among these blood samples 34 (62%) contained Staphylococcus epidermidis, five (9%) Staphylococcus hominis, five (9%) Staphylococcus haemolyticus, four (7%) Staphylococcus aureus, two (3%) Enterococcus faecium, one (2%) Enterococcus durans, one (2%) Streptococcus agalactiae, one (2%) Streptococcus pyogenes, one (2%) Streptococcus oralis group mitis, and one (2%) Kocuria kristinae. Of these Gram-positive cocci 44 (80%) were coagulase-negative staphylococci.
Standard method for identification and antimicrobial susceptibility profiling of bacteria in blood cultures
Blood samples were secured in Bactec culture vial types Plus Aerobic/F (enriched soybean-casein digest broth), Bactec Plus Anaerobic/F (prereduced enriched soybean-casein digest broth) or Peds Plus F (enriched soybean-casein digest broth), and bacterial growth was monitored with the Bactec 9240 fluorescent instrument. From the positive samples a small volume was inoculated onto blood agar, salt mannitol agar and McConkey agar plates and incubated overnight at 37°C. The inoculated blood agar plates were incubated at 5% CO2. Next, a standardized bacterial suspension, according to the manufacturer’s instructions, was prepared from pure cultures which had been grown overnight and the appropriate Vitek ID and AST cards were inoculated. The Vitek 2 system (Vitek 2, software version R04.03, and advanced Expert System software, version R04.02C; bioMérieux, Marcy l’Étoile, France) was used for reading and interpretation of the results. The ID GPC cards were used for the identification of Gram-positive cocci. The AST-536 cards were used for antimicrobial susceptibility testing (AST) of Gram-positive cocci with the staphylococcal Gram stain (in clusters and tetrads). The AST-534 cards were used for antimicrobial susceptibility testing of Gram-positive cocci with the streptococcal Gram stain (in pairs and chains). The following antimicrobial agents were included: benzylpenicillin, oxacillin, clindamycin, erythromycin, levofloxacin, ciprofloxacin, norfloxacin, linezolid, quinupristin/dalfopristin, rifampicin, tetracycline, gentamicin, tobramycin, trimethoprim/sulfamethoxazole, teicoplanin, and vancomycin. The antimicrobial susceptibility profile was assessed for a total of 768 isolate-antimicrobial combinations.
Detergent
Saponin was purchased from Sigma-Aldrich Co. (St. Louis, Missouri). A sterile stock solution of 1% wt/v saponin prepared in Airlife 0.45% sodium chloride (Cardinal Health, Allegiance Healthcare Corporation, Illinois) was stored at room temperature until use.
Rapid identification and antimicrobial susceptibility profiling of cocci in blood cultures
This new method was performed as previously described [19]. In short, a 7-ml sample of a positive blood culture bottle was incubated with saponin (0.01% final concentration, which was found to be optimal in our preliminary experiments) for 15 min at room temperature and then inoculated into Serum Separator Tubes (Becton Dickinson Vacutainer Systems). Bacteria were sedimented on the surface of the silicon layer of the vacutainer tube by centrifugation at 2,000 ×g for 10 min. The supernatant was discarded and the cocci were harvested with a pipette. Then, a suspension of 0.70–0.75 McFarland in 2 ml of Airlife 0.45% sodium chloride using the Densichek Vitek densitometer was prepared. Such a suspension was used to inoculate the appropriate Vitek identification cards. The Vitek 2 system automatically processes the antimicrobial susceptibility profile until the MICs (minimum inhibitory concentrations) were obtained. To find out if the cards had been inoculated with a sufficient bacterial inoculum size, a subculture of serial dilutions from the McFarland suspension was performed on blood agar plates and the number of viable bacteria determined microbiologically.
Data analysis
Identification and antimicrobial susceptibility profiling of the cocci with this new method were evaluated using the data by the standard method as reference. For this purpose, identification results were divided into three categories: concordantly identified, misidentified (where the bacterium was incorrectly identified at the genus or species level), and not identified. Discrepancies in bacterial identification between the two methods were resolved by ID32 Staph (bioMerieux) or Rapid ID32 Strep (bioMerieux) methodology. In case the two methods produced concordant results, no further attempt was undertaken to confirm the strain identities.
The MIC values of the bacteria for the various antimicrobials obtained by the new and the standard methods were translated into clinical categories (susceptible, intermediate or resistant) according to the interpretive criteria of the Vitek 2 expert system. Results in antimicrobial susceptibility profiles of the cocci according to the new and standard inoculation methods were recorded as follows: agreement, very major errors (false susceptible), major errors (false resistant), and minor errors (susceptible/resistant versus intermediate susceptibility). Finally, discrepancies between the results from the new and standard methods were resolved by the E-test (AB Biodisk, Solna, Sweden), which was performed in accordance with the manufacturer’s instructions. Clinical and Laboratory Standards Institute (CLSI, 2006)-defined breakpoints were used to interpret results.
Results
Identification of Gram-positive cocci in blood cultures by the new method
The results obtained with the new method were available at least 12 hours and often 24 hours earlier than those with the standard method, depending on how the workflow is organized in the laboratory. The latter results were used as reference for the analysis of the reliability of the new method. We found that 49 (89%) of the 55 Gram-positive cocci were concordantly identified and that six cocci (11%) were misidentified with the new method (Table 1). One of the misidentified strains was Enterococcus durans, which was reported as Enterococcus gallinarum, whereas the other five belong to the genus Staphylococcus: one S. aureus and one S. epidermidis were incorrectly identified as Kocuria kristinae, another S. epidermidis isolate was reported as Staphylococcus intermedius, one S. hominis was identified as S. epidermidis and another as Kocuria varians. In the cases of the misidentified S. aureus strain and one of the S. hominis strains, the number of bacteria in the suspension used to inoculate the Vitek cards, i.e. 104 and 105 CFU/ml, respectively, was too low for accurate identification. Differing from the studies in which only positive aerobic blood culture bottles were used [11, 15], in our study blood samples with Gram-positive cocci were obtained from aerobic (69%), anaerobic (12%), and pediatric (19%) bottles. We noted that three (8%) of 38 samples from aerobic blood culture bottles, one (10%) of ten from pediatric bottles, and two (29%) of seven from anaerobic bottles were misidentified by the new method.
Antimicrobial susceptibility profiling of Gram-positive cocci in blood cultures by the new method
The antimicrobial susceptibility profiles of only 46 concordantly identified bacterial isolates could be analysed, as no profiles for S. pyogenes, S. oralis group mitis, and Kocuria spp. were available from the Vitek 2 system. In addition, the susceptibility profile was automatically determined for three of the six misidentified bacterial isolates by the system; the 3 isolates that were incorrectly identified as Kocuria spp. were not further analysed. Comparison of the antimicrobial susceptibility profiles of the cocci obtained by the new and the standard methods revealed that 26 (53%) of the 49 isolates showed complete agreement for all clinical categories (Table 2). Discrepancies in clinical categories, at least for a single drug, between the different methods were further resolved by the E-test. The results revealed that with the new method, but not with the standard method, the antimicrobial susceptibility profile was correct for seven (15%) of 46 concordantly identified and one of the three misidentified strains. Therefore, eight (16%) of 49 bacteria showed correct antimicrobial susceptibility for all drugs. Together, 34 (69%) of 49 isolates showed a concordant/correct antimicrobial susceptibility profile for all drugs.
The results obtained by the new and standard methods were compared, and the total percent error as well as the percent error for each drug are shown in Table 2. The overall error rate was 2.3% (1% very major errors and 1.3% minor errors). All very major errors arose from aminoglycosides (gentamicin and tobramycin) and the sulfonamide trimethoprim/sulfamethoxazole, and the minor errors from gentamicin, the fluoroquinolone levofloxacin, and the glycopeptide teicoplanin. The categorical agreement for all drugs investigated was greater than 95% except for levofloxacin, gentamicin, and trimethoprim/sulfamethoxazole.
Discussion
The main finding of this study is that a simple modification, i.e. addition of a detergent like saponin to the fluid of positive blood cultures, leads to the rapid and reliable identification and antimicrobial susceptibility profiling of Gram-positive cocci in blood cultures by the Vitek 2 system. This conclusion is based on the following findings. First, a short exposure of the blood cultures to saponin resulted in a sufficient bacterial inoculum size for identification and susceptibility profiling, thus cutting down the time required to obtain the results for the identification and antimicrobial susceptibility profiling by at least 12 hours and often 24 hours depending on how the workflow is organized. Since a low inoculum is a known source of error in such microbiological analyses by automated systems [11], the number of viable bacteria in the bacterial suspension used to fill the Vitek cards was always determined to account for possible mistakes. However, low inoculum size was found in only two (3.6%) of the 55 blood samples exposed to saponin. The mechanism underlying the effects of saponin could be that the detergent lyses the nonmicrobial cells in blood thereby releasing their intracellular bacteria [18]. Moreover, we found similar results using other detergents, i.e. triton and tween-20 (unpublished observations). This reduction in time required to obtain the microbiological results is expected to lead to a significant decrease in patient morbidity, mortality, and costs [20]. An epidemiological study conducted in the United States [21] pointed out that the bacterial identification and antimicrobial susceptibility profiling results from the Vitek system can be simply verified on the first day that the results are available. This allowed initiation of appropriate antimicrobial therapy statistically earlier, resulting in a decreased length of hospital stay of two days and corresponding costs per patient. Since this rapid and reliable method would allow a further shortening of this time frame, further clinical and financial benefits are to be expected.
Second, concordant identification of the cocci by the new and the standard methods was found in 89% of the blood samples containing Gram-positive bacteria. In addition, the antimicrobial susceptibility profiles of almost 70% of the bacterial strains by the new method was concordant/correct in comparison to the results by the standard method. As the standard method, which includes the ability and accuracy of the Vitek 2 system under routine laboratory conditions, has been compared extensively to reference methods with good results [22–26], we used the results obtained with the standard method as reference in our study, except in a few cases where it was necessary to provide a definitive identification by a manual method, i.e. the ID32 Staph or Rapid ID32 Strep.
In this study we excluded all samples with more than one type of bacterium as mixed cultures are a known source of error in bacterial identification and antimicrobial susceptibility profiling. In agreement with previously published rates for polymicrobic bacteremia [11, 16, 17, 27, 28], seven (11%) of the 64 samples that appeared monomicrobic in the Gram stain were later found to be polymicrobic and therefore excluded from our further analyses. It should be realized that the results obtained for blood samples with the new method should be considered preliminary until the purity of inoculum has been verified by subculture.
The third important finding of this study is that the new method involving the Vitek 2 system can be used to provide antimicrobial susceptibility results for monomicrobic blood cultures containing Gram-positive cocci detected by the Bactec 9240 with 97.7% overall agreement of clinical categories, with only 1% very major errors and 1.3% minor errors, in comparison with the standard method. Of note, almost no errors were observed for the antibiotics most frequently used to treat systemic infections caused by staphylococci and enterococci (i.e. vancomycin, teicoplanin, and linezolid). Complete agreement in clinical categories was found for 53% of the isolates. On the basis of another reference method (E-test) used for arbitration of discrepancies in clinical categories between the new and the standard inoculation methods, an additional 16% showed correct antimicrobial susceptibility by the new method for all drugs, thus reaching about 70% concordant/correct antimicrobial susceptibility profiling. For all except two antibiotic agents (levofloxacin and gentamicin) the agreement in clinical categories was >90%, thus meeting the selection criteria for an antimicrobial susceptibility profiling system proposed by Jorgensen [29]. In conclusion, direct inoculation of Vitek 2 cards with specially processed fluid from positive Bactec 9240 blood culture bottles allows the rapid and reliable identification and susceptibility profiling of Gram-positive cocci. It should be noted that the purity of the direct inoculum should be established before the results obtained with this new method can be reported. This does not delay the report as it can be analysed on subcultures inoculated the previous day. In addition, as misidentification or mistakes in the antimicrobial susceptibility profiling of bacteria by the direct method incidently may occur we also propose a confirmation test for identification and antimicrobial susceptibility profiling of the bacteria in these subcultures. Obviously, further studies including a larger number of blood samples containing Gram-positive bacteria and a set of Gram-positive bacteria that are difficult to identify or that have unusual antimicrobial susceptibility patterns are needed to appreciate the potential of this new and rapid method.
References
Pittet D, Li N, Woolson RF, Wenzel RP (1997) Microbiological factors influencing the outcome of nosocomial bloodstream infections: a 6-year validated, population-based model. Clin Infect Dis 24:1068–1078
Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB (2004) Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis 39:309–317. doi:10.1086/421946
Bearman GM, Wenzel RP (2005) Bacteremias: a leading cause of death. Arch Med Res 36:646–659. doi:10.1016/j.arcmed.2005.02.005
Esel D, Doganay M, Alp E, Sumerkan B (2003) Prospective evaluation of blood cultures in a Turkish university hospital: epidemiology, microbiology and patient outcome. Clin Microbiol Infect 9:1038–1044. doi:10.1046/j.1469-0691.2003.00714.x
Haug J, Harthug S, Kalager T, Digranes A, Solberg CO (1994) Bloodstream infections at a Norwegian university hospital, 1974–1979 and 1988–1989: changing etiology, clinical features, and outcome. Clin Infect Dis 19:246–256
Kaden J, Zwerenz P, Lambrecht HG, Dostatni R (2002) Lipopolysaccharide-binding protein as a new and reliable infection marker after kidney transplantation. Transpl Int 15:163-172. doi:10.1111/j.1432-2277.2002.tb00147.x
Rizoli SB, Marshall JC (2002) Saturday night fever: finding and controlling the source of sepsis in critical illness. Lancet Infect Dis 2:137–144
van Langevelde P, Joop K, van Loon J, Frolich M, Groeneveld PH, Westendorp RG, van Dissel JT (2000) Endotoxin, cytokines, and procalcitonin in febrile patients admitted to the hospital: identification of subjects at high risk of mortality. Clin Infect Dis 31:1343–1348. doi:10.1086/317480
Bruins MJ, Bloembergen P, Ruijs GJ, Wolfhagen MJ (2004) Identification and susceptibility testing of Enterobacteriaceae and Pseudomonas aeruginosa by direct inoculation from positive BACTEC blood culture bottles into Vitek 2. J Clin Microbiol 42:7–11. doi:10.1128/JCM.42.1.7-11.2004
Chen JR, Lee SY, Yang BH, Lu JJ (2008) Rapid identification and susceptibility testing using the VITEK(R) 2 system using culture fluids from positive BacT/ALERT(R) blood cultures. J Microbiol Immunol Infect 41:259–264
de Cueto M, Ceballos E, Martinez-Martinez L, Perea EJ, Pascual A (2004) Use of positive blood cultures for direct identification and susceptibility testing with the Vitek 2 system. J Clin Microbiol 42:3734–3738. doi:10.1128/JCM.42.8.3734-3738.2004
Fontanals D, Salceda F, Hernández J, Sanfeliu I, Torra M (2002) Evaluation of wider system for direct identification and antimicrobial susceptibility testing of gram-negative bacilli from positive blood culture bottles. Eur J Clin Microbiol Infect Dis 21:693–695. doi:10.1007/s10096-002-0791-4
Funke G, Funke-Kissling P (2004) Use of the BD PHOENIX automated microbiology system for direct identification and susceptibility testing of gram-negative rods from positive blood cultures in a three-phase trial. J Clin Microbiol 42:1466–1470. doi:10.1128/JCM.42.4.1466-1470.2004
Hansen DS, Jensen AG, Nørskov-Lauritsen N, Skov R, Bruun B (2002) Direct identification and susceptibility testing of enteric bacilli from positive blood cultures using VITEK (GNI+/GNS-GA). Clin Microbiol Infect 8:38–44. doi:10.1046/j.1469-0691.2002.00372.x
Ling TK, Liu ZK, Cheng AF (2003) Evaluation of the VITEK 2 system for rapid direct identification and susceptibility testing of gram-negative bacilli from positive blood cultures. J Clin Microbiol 41:4705–4707. doi:10.1128/JCM.41.10.4705-4707.2003
Waites KB, Brookings ES, Moser SA, Zimmer BL (1998) Direct susceptibility testing with positive BacT/Alert blood cultures by using MicroScan overnight and rapid panels. J Clin Microbiol 36:2052–2056
Waites KB, Brookings ES, Moser SA, Zimmer BL (1998) Direct bacterial identification from positive BacT/Alert blood cultures using MicroScan overnight and rapid panels. Diagn Microbiol Infect Dis 32:21–26. doi:10.1016/S0732-8893(98)00058-3
Murray PR, Spizzo AW, Niles AC (1991) Clinical comparison of the recoveries of bloodstream pathogens in Septi-Chek brain heart infusion broth with saponin, Septi-Chek tryptic soy broth, and the isolator lysis-centrifugation system. J Clin Microbiol 29:901–905
Lupetti A, Barnini S, Castagna B, Nibbering PH, Campa M (2009) Rapid identification and antimicrobial susceptibility testing of Gram-positive cocci in blood cultures by direct inoculation into the BD Phoenix system. Clin Microbiol Infect. doi:10.1111/i.1469-0691.2009.03006.x
Doern GV, Vautour R, Gaudet M, Levy B (1994) Clinical impact of rapid in vitro susceptibility testing and bacterial identification. J Clin Microbiol 32:1757–1762
Barenfanger J, Drake C, Kacich G (1999) Clinical and financial benefits of rapid bacterial identification and antimicrobial susceptibility testing. J Clin Microbiol 37:1415–1418
Barry J, Brown A, Ensor V, Lakhani U, Petts D, Warren C, Winstanley T (2003) Comparative evaluation of the VITEK 2 Advanced Expert System (AES) in five UK hospitals. J Antimicrob Chemother 51:1191–1202
Funke G, Funke-Kissling P (2005) Performance of the new VITEK 2 GP card for identification of medically relevant gram-positive cocci in a routine clinical laboratory. J Clin Microbiol 43:84–88. doi:10.1128/JCM.43.1.84-88.2005
Garcia-Garrote F, Cercenado E, Bouza E (2000) Evaluation of a new system, VITEK 2, for identification and antimicrobial susceptibility testing of enterococci. J Clin Microbiol 38:2108–2111
Joyanes P, del Carmen Conejo M, Martínez-Martínez L, Perea EJ (2001) Evaluation of the VITEK 2 system for the identification and susceptibility testing of three species of nonfermenting gram-negative rods frequently isolated from clinical samples. J Clin Microbiol 39:3247–3253. doi:10.1128/JCM.39.9.3247-3253.2001
Livermore DM, Struelens M, Amorim J, Baquero F, Bille J, Canton R, Henning S, Gatermann S, Marchese A, Mittermayer H, Nonhoff C, Oakton KJ, Praplan F, Ramos H, Schito GC, Van Eldere J, Verhaegen J, Verhoef J, Visser MR (2002) Multicentre evaluation of the VITEK 2 Advanced Expert System for interpretive reading of antimicrobial resistance tests. J Antimicrob Chemother 49:289–300
Moore DF, Hamada SS, Marso E, Martin WJ (1981) Rapid identification and antimicrobial susceptibility testing of gram-negative bacilli from blood cultures by the AutoMicrobic system. J Clin Microbiol 13:934–939
Putnam LR, Howard WJ, Pfaller MA, Koontz FP, Jones RN (1997) Accuracy of the Vitek system for antimicrobial susceptibility testing Enterobacteriaceae bloodstream infection isolates: use of “direct” inoculation from Bactec 9240 blood culture bottles. Diagn Microbiol Infect Dis 28:101–104. doi:10.1016/S0732-8893(97)00014-X
Jorgensen JH (1993) Selection criteria for an antimicrobial susceptibility testing system. J Clin Microbiol 31:2841–2844
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Lupetti, A., Barnini, S., Castagna, B. et al. Rapid identification and antimicrobial susceptibility profiling of Gram-positive cocci in blood cultures with the Vitek 2 system. Eur J Clin Microbiol Infect Dis 29, 89–95 (2010). https://doi.org/10.1007/s10096-009-0825-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-009-0825-2