
Abstract
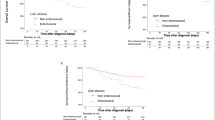
Clinicians sometimes experience treatment failure in the initial empirical antibiotics treatment using cephalosporins in cirrhotic patients with spontaneous bacterial peritonitis (SBP). Enterococcus, which is intrinsically resistant to cephalosporins, may be one of the causes of treatment failure. The aim of this study was to evaluate the clinical importance and the clinical characteristics of spontaneous enterococcal peritonitis (SEP). This was a retrospective cohort study of 359 patients with SBP treated in a single tertiary care center in South Korea from January 2000 through December 2004. We evaluated the clinical manifestation and the treatment results of SBP patients with enterococci identified from ascites culture. During the observation period, 13 of 359 patients (3.6%) diagnosed with culture-positive SBP had enterococcal peritonitis. For the initial empirical treatment, third-generation cephalosporins were administered to the 13 patients, ten of whom (76.9%) did not improve in the first 48 h. An in vitro antibiotic sensitivity test showed that the identified enterococci were susceptible to ampicillin plus gentamycin in eight patients (61.5%) and there was no vancomycin-resistant enterococcus. Although antibiotics were changed to antienterococcal antibiotics in 11 patients, only five patients improved. As a result, eight of the 13 patients (61.5%) with enterococcal SBP died during the observation period, and the one-month mortality was significantly higher from enterococcal SBP than from nonenterococcal SBP (P = 0.038). We conclude that enterococcal SBP has poor prognosis and it is reasonable to use antienterococcal antibiotics when enterococcus is identified from ascites culture of patients with liver cirrhosis.
Similar content being viewed by others

References
Guarner C, Soriano G (1997) Spontaneous bacterial peritonitis. Semin Liver Dis 17:203–217
Such J, Runyon BA (1998) Spontaneous bacterial peritonitis. Clin Infect Dis 27:669–676. doi:10.1086/514940
Felisart J, Rimola A, Arroyo V et al (1985) Cefotaxime is more effective than is ampicillin-tobramycin in cirrhotics with severe infections. Hepatology 5:457–462. doi:10.1002/hep.1840050319
Navasa M, Follo A, Llovet JM et al (1996) Randomized, comparative study of oral ofloxacin versus intravenous cefotaxime in spontaneous bacterial peritonitis. Gastroenterology 111:1011–1017. doi:10.1016/S0016-5085(96)70069-0
Moellering RC Jr, Eliopoulos GM (1984) Activity of cefotaxime against enterococci. Diagn Microbiol Infect Dis 2:85S–90S
Barie PS, Christou NV, Dellinger EP et al (1990) Pathogenicity of the enterococcus in surgical infections. Ann Surg 212:155–159. doi:10.1097/00000658-199008000-00007
Dougherty SH (1984) Role of enterococcus in intraabdominal sepsis. Am J Surg 148:308–312. doi:10.1016/0002-9610(84)90460-4
Gorbach SL (1993) Intraabdominal infections. Clin Infect Dis 17:961–965
Nichols RL, Muzik AC (1992) Enterococcal infections in surgical patients: the mystery continues. Clin Infect Dis 15:72–76
Rohrborn A, Wacha H, Schoffel U et al (2000) Coverage of enterococci in community acquired secondary peritonitis: results of a randomized trial. Surg Infect (Larchmt) 1:95–107. doi:10.1089/109629600321137
Dupont H, Montravers P, Mohler J et al (1998) Disparate findings on the role of virulence factors of Enterococcus faecalis in mouse and rat models of peritonitis. Infect Immun 66:2570–2575
Onderdonk AB, Bartlett JG, Louie T et al (1976) Microbial synergy in experimental intra-abdominal abscess. Infect Immun 13:22–26
Montravers P, Mohler J, Saint Julien L et al (1997) Evidence of the proinflammatory role of Enterococcus faecalis in polymicrobial peritonitis in rats. Infect Immun 65:144–149
Hassner A, Kletter Y, Shlag D et al (1981) Impaired monocyte function in liver cirrhosis. Br Med J (Clin Res Ed) 282:1262–1263
Kourilsky O, Leroy C, Peltier AP (1973) Complement and liver cell function in 53 patients with liver disease. Am J Med 55:783–790. doi:10.1016/0002-9343(73)90259-3
Rajkovic IA, Williams R (1986) Abnormalities of neutrophil phagocytosis, intracellular killing and metabolic activity in alcoholic cirrhosis and hepatitis. Hepatology 6:252–262. doi:10.1002/hep.1840060217
Soriano G, Guarner C, Tomás A et al (1992) Norfloxacin prevents bacterial infection in cirrhotics with gastrointestinal hemorrhage. Gastroenterology 103:1267–1272
Blaise M, Pateron D, Trinchet JC et al (1994) Systemic antibiotic therapy prevents bacterial infection in cirrhotic patients with gastrointestinal hemorrhage. Hepatology 20:34–38
Rimola A, Bory F, Teres J et al (1985) Oral, nonabsorbable antibiotics prevent infection in cirrhotics with gastrointestinal hemorrhage. Hepatology 5:463–467. doi:10.1002/hep.1840050320
Barrall DT, Kenney PR, Slotman GJ et al (1985) Enterococcal bacteremia in surgical patients. Arch Surg 120:57–63
Schlossberg D (2006) Clinical approach to antibiotic failure. Med Clin North Am 90:1265–1277. doi:10.1016/j.mcna.2006.07.004
Williamson R, le Bouguénec C, Gutmann L et al (1985) One or two low affinity penicillin-binding proteins may be responsible for the range of susceptibility of Enterococcus faecium to benzylpenicillin. J Gen Microbiol 131:1933–1940
Moellering RC Jr (1983) Antibiotic synergism—lessons from the enterococcus. Trans Am Clin Climatol Assoc 94:55–62
Hampel H, Bynum GD, Zamora E et al (2001) Risk factors for the development of renal dysfunction in hospitalized patients with cirrhosis. Am J Gastroenterol 96:2206–2210. doi:10.1111/j.1572-0241.2001.03958.x
Acknowledgment
This study was supported by the Seoul National University Hospital Research Fund (#03-2006-019) and the Korea Health 21 R&D Project (#0412-CR01-0704-0001).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lee, JH., Yoon, JH., Kim, B.H. et al. Enterococcus: not an innocent bystander in cirrhotic patients with spontaneous bacterial peritonitis. Eur J Clin Microbiol Infect Dis 28, 21–26 (2009). https://doi.org/10.1007/s10096-008-0578-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-008-0578-3