
Abstract
Like the apolipoprotein E (APOE) gene, the most common genetic determinant for Alzheimer’s disease (AD), the cholesteryl ester transfer protein (CETP) is involved in lipid metabolism. We studied the I405V polymorphism of the CETP gene in relation to AD. We genotyped 544 AD cases and 5,404 controls from the Rotterdam study, using a TaqMan allelic discrimination assay. Odds ratios (ORs) for AD were estimated using logistic regression analysis. CETP VV carriers showed significantly increased high-density lipoprotein levels compared to the IV and II carriers. In the overall analysis of AD, the risk of disease for the VV carriers of the CETP polymorphism was non-significantly increased compared to II carriers ORVV = 1.33, 95% confidence interval (CI) 0.96–1.90 p = 0.08). In those without the APOE*4 allele, the risk of AD for VV carriers was increased 1.67-fold (95% CI 1.11–2.52, p = 0.01). The difference in the relationship between CETP and AD between APOE*4 carriers and APOE*4 non-carriers was statistically significant (p for interaction = 0.04). Our results suggest that the VV genotype of the I405V polymorphism of the CETP gene increases the risk of AD in the absence of the APOE*4 allele, probably through a cholesterol metabolism pathway in the brain.
Similar content being viewed by others


Introduction
Alzheimer’s disease (AD) is a complex neurodegenerative disorder characterized by progressive memory loss and deterioration of cognitive function. Of the many genes studied thus far, the only consistently replicated genetic risk factor for AD has been the apolipoprotein E (APOE) gene. APOE, which transports cholesterol in the brain [1], may relate to AD by modifying the production of Amyloid β (Aβ). High cellular cholesterol may promote Aβ production and senile plaque deposition, thus increasing the risk of AD [2–7]. Cholesterol dysregulation is linked to the pathogenesis of AD [8, 9]. Lack of cholesterol supply to neurons impairs neurotransmission and synaptic plasticity [10] and induces neurodegeneration and tau pathology [11]. Additionally, there is some evidence that patients treated with cholesterol lowering drugs, such as statins, have a reduced prevalence of AD [12].
High-density lipoprotein (HDL), essential for the removal of excess cholesterol from cells, exerts several potentially anti-atherogenic effects, including reverse cholesterol transport from peripheral cells to the liver [13]. Cholesteryl ester transfer protein (CETP) is a key player in lipid metabolism that catalyses the transfer of cholesteryl esters from HDL particles to triglyceride-rich lipoproteins in exchange for triglycerides [14]. CETP, a protein composed of 439 amino acid residues, is coded by the CETP gene, which is located on chromosome 16q21 and contains 14 exons. The 405V allele of the CETP I405V polymorphism (rs5882) in exon 14 was previously associated with lower levels of CETP protein, higher levels of circulating HDL [15], a lower incidence of cardiovascular disease [15], and longer survival [16].
Studies evaluating the role of the CETP gene in AD have shown intriguing results. While one previous study [17] showed evidence that the C-629A polymorphism of the CETP gene modifies the risk of AD in association with the APOE gene by reducing the risk of AD, another study found no effect of this gene on the disease [18]. We studied the I405V polymorphism of the CETP gene in relation to AD in a large population-based study and investigated whether this polymorphism is independently associated with AD, or acts in concert with the APOE gene in conferring risk for the disease.
Materials and methods
Study population
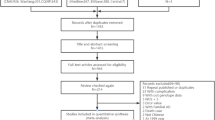
Our study is part of the Rotterdam study, a population-based follow-up study of determinants of diseases in the elderly. All inhabitants of Ommoord, a suburb of Rotterdam, aged 55 years or more, were invited to participate. The design of the study was previously described [19]. From all subjects, an informed consent was obtained and the Medical Ethics committee of the Erasmus Medical Center approved the study. A number of 7,983 participants (response rate of 78%) were examined at baseline (1990 to 1993). Information on age, smoking behavior, and medical history was obtained using a computerized questionnaire.
Patient ascertainment
Dementia was diagnosed following a three-step protocol [20, 21]. All participants were screened at follow-up visits using two tests of cognition: the mini-mental state examination (MMSE) [22] and the geriatric mental state schedule (GMS) [23]. Participants that were screen-positives (MMSE score<26 or GMS organic level>0) underwent the Cambridge examination for mental disorders of the elderly (CAMDEX). In addition, the cohort was continuously monitored for incident dementia through a computerized link between the study database and the medical records from general practitioners and the Regional Institute for Outpatient Mental Health Care until January 1, 2005. The diagnosis of dementia, and dementia subtype, was made in accordance with accepted criteria for dementia (DSM-III-R) [24] and Alzheimer’s disease (NINDS-ADRDA) [25] by a panel consisting of a neurologist, a neuropsychologist and a research physician.
Genotyping
DNA was extracted from whole blood samples using standard methods [26]. The APOE gene was genotyped using the conditions described by Wenham et al. [27]. Samples were genotyped for the CETP I405V polymorphism using a TaqMan allelic discrimination Assay-By-Design (Applied Biosystems, Foster City, CA). We genotyped 317 samples twice and used them as controls by comparing both genotypes, and if present, samples with discordant genotypes were excluded. Forward and reverse primer sequences are available on request. The assays utilized 5 ng of genomic DNA and 2 μl reaction volumes. The amplification and extension protocol was as follows: an initial activation step of 10 min at 95°C preceded 40 cycles of denaturation at 95°C for 15 s. and annealing and extension at 50°C for 60 s. Allele-specific fluorescence was then analyzed on an ABI Prism 7900HT Sequence Detection System with SDS v 2.1 (Applied Biosystems, Foster City, CA).
Statistical analysis
Genotype frequency of the CETP I405V was compared between cases and controls and Hardy-Weinberg equilibrium (HWE) was assessed for all genotypes using the χ 2 test. Odds ratios (OR) and 95% confidence intervals (CI) were estimated using multivariate logistic regression, adjusting for age, gender, and APOE*4 status, using all available AD cases (prevalent and incident). The APOE*4 stratified analyses were adjusted for age and gender. All analyses were performed using SPSS 11.0
Results
Table 1 shows the general characteristics of the study population. The distribution of the CETP I405V genotypes was in HWE (p = 0.38). The mean serum HDL level of the VV carriers was significantly increased compared to the IV and II carriers (p = 0.001). There were no statistically significant differences in the distributions of the other variables between the genotype groups.
The genotype frequencies of the CETP I405V polymorphism are shown in Table 2. Overall, we did not find any significant difference in the genotypic distribution of the CETP I405V polymorphism between AD cases (prevalent and incident) and controls. After stratifying for APOE*4, we found a statistically significant difference in the distribution between cases and controls in those without APOE*4 (χ 2 = 6.62, p = 0.04). This difference was explained by an increased frequency of the VV genotype in cases.
Table 3 shows the odds ratios overall and stratified by APOE*4. Including all prevalent and incident cases, a non-significant increase in the odds ratios was seen in the overall analysis when comparing the VV carriers to the II carriers of the I405V polymorphism, (OR = 1.33, 95% CI 0.96–1.90, p = 0.08). In those without APOE*4, the OR increased to 1.67 (95% CI 1.11–2.52, p = 0.01). The IV carriers showed a non-significant increase in risk of AD compared to II carriers in those without APOE*4, OR = 1.26 (95% CI 0.96–1.64, p = 0.09). These estimates did not change after adjusting for serum HDL levels. Serum HDL level itself was not associated with AD. The frequencies of the CETP genotypes in the two types of cases (incident and prevalent) were not statistically different. This indicates that the AD patient selection does not affect the proposed genotype-outcome relationship. When we restricted the analysis to the incident cases only, the OR for the VV carriers compared to the II carriers was 1.24 (0.86–1.82, p = 0.24) in the overall analysis. This OR significantly increased to 1.58 (1.0–2.5, p = 0.05). When we analyzed the incident and prevalent cases together we did not detect an effect of the VV genotype of the CETP gene on the risk of AD in those with APOE*4 (p = 0.65; Table 3). The difference in the relationship of the CETP gene and AD between APOE*4 carriers and non-carriers was statistically significant (p for interaction = 0.04). The mean age at onset in patients carrying the VV genotype of the CETP I405V polymorphism (88.64 years, SD = 7.19) did not differ significantly compared to that of the II and IV carriers (88.75 years, SD = 8.02 for IV carriers and 87.75 years, SD = 817 for II carriers, p = 0.41). In those without the APOE*4 allele, the difference in age at onset between VV carriers and non-carriers was also not significant (p = 0.48).
Discussion
Our results suggest an increased risk of AD for carriers of the VV genotype of the I405V polymorphism in the CETP gene. The increase in risk was 1.67-fold in non-carriers of the APOE*4 allele. No association was observed between this CETP polymorphism and AD in those with the APOE*4 allele. We detected a statistically significant difference in the relationship between CETP and AD in APOE*4 carriers and non-carriers (p for interaction = 0.04). The association was independent of serum HDL levels, which by itself was not associated with AD.
The relationship between lipid transfer proteins, such as CETP, and AD has been previously studied. In an experimental study, Yamada et al. [28] showed that in brains of patients with AD, reactive astrocytes in gray and white matter exhibit CETP-like immunoreactivity. Thus, CETP-positive astrocytes may play a role in the pathology of Alzheimer’s disease, in particular tissue repair. Our findings partly overlap with those of other genetic studies. The CETP C-629A and TaqI B polymorphisms have been studied with respect to AD. A study in a Spanish population of the relationship between the CETP C-629A and I405V polymorphisms and the APOE*4 allele indicated that the CETP gene modifies AD risk possibly through modulation of brain cholesterol metabolism [17]. This modification effect was seen only for the C-629A polymorphism and not for the I405V. This could be explained by the LD pattern of these two polymorphisms, but according to data available in HapMap [29], the D′ and r 2 values between these two variants are not high enough that can serve as tagging markers for each other in this gene (D′ = 0.51, r 2 = 0.076). On the other hand, studies that evaluated the effect of other promoter polymorphisms and the TaqI B polymorphism found no effect of this gene on the disease [18, 30].
Since the VV genotype is associated with lower levels of CETP and higher HDL, our study is compatible with the view that low CETP levels may increase the risk of AD through a reduction in neuronal repair capacity. An alternative mechanism is related to cholesterol removal by HDL; this is one of the mechanisms that cells use to keep the levels of cholesterol in their membranes fairly constant [9, 13, 31]. This would imply that VV carriers might be at lower risk of developing AD. The fact that we found this group to be at a higher risk of AD could be explained by previous findings suggesting that the actions of HDL in the transfer of lipids in brain may differ from those in the peripheral system [32]. In fact, the processing of cholesterol in brain is restricted in the central nervous system by the blood-brain barrier, which is impermeable to plasma lipoproteins [33]. Unlike fatty acids that must be transported to the central nervous system from the periphery, brain cholesterol is mainly independent of dietary uptake or synthesis in the liver and is synthesized almost entirely in the brain [34]. The CETP and APOE genes overlap physiologically [35, 36], which provides extra support for a role of the CETP gene independent of the APOE gene in the risk of Alzheimer’s disease. In our overall analysis (all cases and controls, all APOE*4 carriers), we observed a borderline significant association between the VV carriers and AD of 1.33, (95% CI 0.96–1.90 p = 0.08), which could indicate that the effect of the CETP gene is observable in both APOE*4 groups, but after stratification by APOE*4, in the carrier group, the effect of the CETP gene is overwhelmed by APOE.
Taken together, our results suggest that the V allele of the I405V polymorphism of the CETP gene increases the risk of AD independently of the APOE gene, probably through the regulation of cholesterol metabolism in the brain. Our data, however, are not supported by the literature, which calls for more studies needed to clarify the role of the CETP gene, as well as the CETP protein and HDL cholesterol, in AD.
References
Mahley RW, Weisgraber KH, Huang Y (2006) Apolipoprotein E4: a causative factor and therapeutic target in neuropathology, including Alzheimer’s disease. Proc Natl Acad Sci USA 103(15):5644–5651
Yanagisawa K, Matsuzaki K (2002) Cholesterol-dependent aggregation of amyloid beta-protein. Ann N Y Acad Sci 977:384–386
Yanagisawa K (2002) Cholesterol and pathological processes in Alzheimer’s disease. J Neurosci Res 70(3):361–366
Puglielli L, Tanzi RE, Kovacs DM (2003) Alzheimer’s disease: the cholesterol connection. Nat Neurosci 6(4):345–351
Michikawa M (2003) The role of cholesterol in pathogenesis of Alzheimer’s disease: dual metabolic interaction between amyloid beta-protein and cholesterol. Mol Neurobiol 27(1):1–12
Michikawa M (2004) Neurodegenerative disorders and cholesterol. Curr Alzheimer Res 1(4):271–275
Abad-Rodriguez J, Ledesma MD, Craessaerts K, Perga S, Medina M, Delacourte A, Dingwall C, De Strooper B, Dotti CG (2004) Neuronal membrane cholesterol loss enhances amyloid peptide generation. J Cell Biol 167(5):953–960
Wolozin B, Kellman W, Ruosseau P, Celesia GG, Siegel G (2000) Decreased prevalence of Alzheimer disease associated with 3-hydroxy-3-methyglutaryl coenzyme a reductase inhibitors. Arch Neurol 57(10):1439–1443
Simons M, Keller P, Dichgans J, Schulz JB (2001) Cholesterol and Alzheimer’s disease: is there a link? Neurology 57(6):1089–1093
Mauch DH, Nagler K, Schumacher S, Goritz C, Muller EC, Otto A, Pfrieger FW (2001) Cns synaptogenesis promoted by glia-derived cholesterol. Science 294(5545):1354–1357
Fan QW, Yu W, Senda T, Yanagisawa K, Michikawa M (2001) Cholesterol-dependent modulation of tau phosphorylation in cultured neurons. J Neurochem 76(2):391–400
Reiss AB (2005) Cholesterol and apolipoprotein E in Alzheimer’s disease. Am J Alzheimers Dis Other Dement 20(2):91–96
Hersberger M, von Eckardstein A (2005) Modulation of high-density lipoprotein cholesterol metabolism and reverse cholesterol transport. Handb Exp Pharmacol (170):537–561
Barter PJ, Kastelein JJ (2006) Targeting cholesteryl ester transfer protein for the prevention and management of cardiovascular disease. J Am Coll Cardiol 47(3):492–499
Blankenberg S, Rupprecht HJ, Bickel C, Jiang XC, Poirier O, Lackner KJ, Meyer J, Cambien F, Tiret L (2003) Common genetic variation of the cholesteryl ester transfer protein gene strongly predicts future cardiovascular death in patients with coronary artery disease. J Am Coll Cardiol 41(11):1983–1989
Atzmon G, Rincon M, Rabizadeh P, Barzilai N (2005) Biological evidence for inheritance of exceptional longevity. Mech Ageing Dev 126(2):341–345
Rodriguez E, Mateo I, Infante J, Llorca J, Berciano J, Combarros O (2006) Cholesteryl Ester Transfer Protein (Cetp) polymorphism modifies the Alzheimer’s disease risk associated with Apoe Epsilon4 Allele. J Neurol 253(2):181–185
Zhu H, Gopalraj RK, Kelly JF, Bennett DA, Estus S (2005) Lack of genetic association of cholesteryl ester transfer protein polymorphisms with late onset Alzheimer’s disease. Neurosci Lett 381(1–2):36–41
Hofman A, Grobbee DE, de Jong PT, van den Ouweland FA (1991) Determinants of disease and disability in the elderly: the Rotterdam elderly study. Eur J Epidemiol 7(4):403–422
Vermeer SE, Prins ND, den Heijer T, Hofman A, Koudstaal PJ, Breteler MM (2003) Silent brain infarcts and the risk of dementia and cognitive decline. N Engl J Med 348(13):1215–1222
Barendregt JJ, Ott A (2005) Consistency of epidemiologic estimates. Eur J Epidemiol 20(10):827–832
Folstein MF, Folstein SE, McHugh PR (1975) “Mini-Mental State”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12(3):189–198
Copeland JR, Kelleher MJ, Kellett JM, Gourlay AJ, Gurland BJ, Fleiss JL, Sharpe L (1976) A semi-structured clinical interview for the assessment of diagnosis and mental state in the elderly: the geriatric mental state schedule. I. Development and reliability. Psychol Med 6(3):439–449
American Psychiatry Association (1987) Diagnostic and statistical manual of mental disorders
McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM (1984) Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA work group under the auspices of department of health and human services task force on Alzheimer’s disease. Neurology 34(7):939–944
Miller SA, Dykes DD, Polesky HF (1988) A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res 16(3):1215
Wenham PR, Price WH, Blandell G (1991) Apolipoprotein E genotyping by one-stage Pcr. Lancet 337(8750):1158–1159
Yamada T, Kawata M, Arai H, Fukasawa M, Inoue K, Sato T (1995) Astroglial localization of cholesteryl ester transfer protein in normal and Alzheimer’s disease brain tissues. Acta Neuropathol (Berl) 90(6):633–636
(2005) A Haplotype Map of the Human Genome. Nature 437(7063):1299–1320
Fidani L, Goulas A, Crook R, Petersen RC, Tangalos E, Kotsis A, Hardy J (2004) An association study of the cholesteryl ester transfer protein taqi B polymorphism with late onset Alzheimer’s disease. Neurosci Lett 357(2):152–154
Jiang XC, Zhou HW (2006) Plasma lipid transfer proteins. Curr Opin Lipidol 17(3):302–308
Bjorkhem I, Meaney S (2004) Brain cholesterol: long secret life behind a barrier. Arterioscler Thromb Vasc Biol 24(5):806–815
Vance JE, Hayashi H, Karten B (2005) Cholesterol homeostasis in neurons and glial cells. Semin Cell Dev Biol 16(2):193–212
Jurevics H, Morell P (1995) Cholesterol for synthesis of myelin is made locally, not imported into brain. J Neurochem 64(2):895–901
Carter CJ, Mahley RW, Huang Y, Weisgraber KH (2007) Convergence of genes implicated in Alzheimer’s disease on the cerebral cholesterol shuttle: app, cholesterol, lipoproteins, and atherosclerosis putting cholesterol in its place: apoe and reverse cholesterol transport. Neurochem Int 50(1):12–38
Mahley RW, Huang Y, Weisgraber KH (2006) Putting cholesterol in its place: apoe and reverse cholesterol transport. J Clin Invest 116(5):1226–1229
Acknowledgement
A. Arias-Vasquez is supported by a grant from the Centre of Medical Systems Biology, grant no. 297-2003 and the Hersenstichting Nederland. The Rotterdam study is supported by the Erasmus Medical Center and Erasmus University Rotterdam, the Netherlands Organization for Scientific Research (NWO), the Netherlands Organization for Health Research and Development (ZonMw), the Research Institute for Diseases in the Elderly (RIDE), the Ministry of Education, Culture and Science, the Ministry of Health, Welfare and Sports, the European Commission (DG XII), and the Municipality of Rotterdam. The contributions of the general practitioners and pharmacists of the Ommoord district are greatly acknowledged. The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Arias-Vásquez, A., Isaacs, A., Aulchenko, Y.S. et al. The cholesteryl ester transfer protein (CETP) gene and the risk of Alzheimer’s disease. Neurogenetics 8, 189–193 (2007). https://doi.org/10.1007/s10048-007-0089-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10048-007-0089-x