
Abstract
Objectives
To compare the outcomes of open darn repair vs open mesh repair in patients undergoing inguinal hernia repair.
Methods
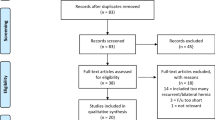
We performed a systematic review and conducted a search of electronic information sources to identify all observational studies and randomised controlled trials (RCTs) investigating outcomes of open darn repair vs open mesh repair for inguinal hernias. Hernia recurrence was considered as the primary outcome measure. The secondary outcome measures included surgical site infection (SSI), haematoma, seroma, neuralgia, urinary retention, length of hospital stay, time to return to normal activities or work, testicular atrophy, operative time and chronic pain. Random or fixed effects modelling was applied to calculate pooled outcome data.
Results
Six RCTs, enrolling 1480 patients with 1485 hernias, and 4 observational studies, enrolling 1564 patients with 1641 hernias, were included. Meta-analysis of RCTs showed no significant difference in terms of recurrence (RD 0.00, 95% CI − 0.01 to 0.01, P = 0.86), SSI (OR 0.83, 95% CI 0.46–1.49, P = 0.52), haematoma (OR 1.21, 95% CI 0.62–2.38, P = 0.57), seroma (OR 0.83, 95% CI 0.42–1.65, P = 0.60), neuralgia (OR 1.05, 95% CI 0.29–3.73, P = 0.94), urinary retention (OR 1.44, 95% CI 0.64–3.21, P = 0.38), length of hospital stay (MD 0.09, 95% CI − 0.28 to 0.46, P = 0.63), time to return to normal activities or work (MD 0.88, 95% CI − 0.90 to 2.66, P = 0.33), testicular atrophy (RD 0.00, 95% CI − 0.02 to 0.02, P = 1.00), and operative time (MD 2.69, 95% CI − 1.75 to 7.14, P = 0.62) between the darn repair and mesh repair groups. Meta-analysis of observational studies also showed no significant difference in terms of recurrence (RD 0.00, 95% CI − 0.02 to 0.02, P = 0.99), SSI (OR 0.47, 95% CI 0.14–1.62, P = 0.23), haematoma (OR 1.07, 95% CI 0.45–2.55, P = 0.89), seroma (OR 0.12, 95% CI 0.01–2.27, P = 0.16), neuralgia (OR 0.25, 95% CI 0.05–1.21, P = 0.08), urinary retention (OR 1.53, 95% CI 0.20–11.96, P = 0.69), time to return to normal activities or work (MD 2.13, 95% CI − 2.18 to 6.44, P = 0.33), testicular atrophy (RD − 0.01, 95% CI − 0.02 to 0.01, P = 0.49), and operative time (MD − 4.76, 95% CI − 13.23 to 3.71, P = 0.27) between the two groups. The evidence was inconclusive for chronic pain. The quality of available evidence was moderate.
Conclusions
Our results suggest that open darn repair is comparable with open mesh repair for inguinal hernias. Considering that consequences of mesh complications in inguinal hernia repair, albeit rare, can be significant, open darn repair provides an equally credible alternative to open mesh repair for inguinal hernias. Further studies are required to investigate patient-reported outcomes and to elicit a superior non-mesh technique.







Similar content being viewed by others


References
Rutkow IM (2003) Demographic and socioeconomic aspects of hernia repair in the United States in 2003. Surg Clin N Am 83(5):1045–1051
Kingsnorth A, LeBlanc K (2003) Hernias: inguinal and incisional. Lancet 362(9395):1561–1571
Bekker J, Keeman JN, Simons MP, Aufenacker TJ (2007) A brief history of the inguinal hernia operation in adults. Ned Tijdschr Geneeskd 151(16):924–931
Moloney GE, Gill WG, Barclay RC (1948) Operations for hernia: technique of nylon darn. Lancet 2(6515):45–48
Moloney GE (1958) Results of nylon-darn repairs of herniae. Lancet 1(7015):273–278
Leacock AL, Rowley RK (1962) Results of nylon repairs in inguinal hernias. Lancet 279(7219):20–21
Callum KG, Doig RL, Kimmonth JB (1974) The results of nylon darn repair for inguinal hernia. Arch Surg 108(1):25–27
Lifschutz H, Juler GL (1986) The inguinal darn. Arch Surg 121(6):717–719
Maingot R (1949) Floss silk darn for inguinal hernia. Proc R Soc Med 42(7):465
Spencer SL (1962) Premuscular nylon darn in inguinal hernia repair. Surg Gynecol Obstet 115:498–500
Lichtenstein IL, Shulman AG, Amid PK, Montllor M (1989) The tension-free hernioplasty. AM J Surg 157(2):188–193
EU Hernia Trialist Collaboration (2002) Repair of groin hernia with synthetic mesh: meta-analysis of randomized controlled trials. Ann Surg 235(3):322–332
Cobb WS, Kercher KW, Heniford BT (2005) The argument for lightweight Polypropylene mesh in hernia repair. Surg Innov 12(1):63–69
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 339:b2700
Sterne JAC, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M et al (2016) ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355:i4919
Higgins JP, Altman DG (2011) Chapter 8: assessing risk of bias in included studies. In: Higgins JP, Green S, editors. Cochrane handbook for systematic reviews of interventions. https://doi.org/10.1002/9780470712184.ch8. http://handbook-5-1.cochrane.org. Accessed 10 Oct 2018
Abd El Maksoud W, Abd El Salam M, Ahmed HH (2014) Comparative study between Lichtenstein procedure and modified darn repair in treating primary inguinal hernia: a prospective randomized controlled trial. Hernia 18:231–236
Chan KY, Rohaizak M, Sukumar N, Shaharuddin S, Jasmi AY (2004) Inguinal hernia repair by surgical trainees at a Malaysian teaching hospital. Asian J Surg 27(4):306–312
Kaynak B, Celik F, Guner A, Guler K, Kaya MA, Celik M (2007) Moloney darn repair versus Lichtenstein mesh hernioplasty for open inguinal hernia repair. Surg Today 37:958–960
Koukourou A, Lyon W, Rice J, Wattchow DA (2001) Prospective randomized trial of polypropylene mesh compared with nylon darn in inguinal hernia repair. Br J Surg 88(7):931–934
Kucuk HF, Sikar HE, Kurt N, Uzun H, Eser M, Tutal F, Tuncer Y (2010) Lichtenstein or darn procedure in inguinal hernia repair: a prospective randomized comparative study. Hernia 14(4):357–360
Al-Saiegh AM, Al-Saffar RS, Al-Khassaki HT (2009) Tension–free inguinal hernia repair comparing ‘mesh’ with ‘darn’ a prospective randomized clinical trial. Iraqi Postgrad Med J 8(3):220–227
Memon GA, Shah SKA, Rehman H (2017) An experience with mesh versus darn repair in inguinal hernias. Pak J Med Sci 33(3):699–702
Nixon SJ, Jawaid H (2009) Recurrence after inguinal hernia repair at ten years by open darn, open mesh and TEP—no advantage with mesh. Surgeon 7(2):71–74
Olasehinde O, Lawal OO, Agbakwuru EA, Adisa AO, Alatise OI, Arowolo OA, Adesunkanmi AR, Etonyeaku AC (2016) Comparing Lichtenstein with darning for inguinal hernia repair in an African population. Hernia 20(5):667–674
Zeybek N, Tas H, Peker Y, Yildiz F, Akdeniz A, Tufan T (2008) Comparison of modified darn repair and Lichtenstein repair of primary inguinal hernias. J Surg Res 146(2):225–229
Luijendijk RW, Hop WC, van den Tol MP, de Lange DC, Braaksma MM, IJzermans JN et al (2000) A comparison of suture repair with mesh repair for incisional hernia. N Engl J Med 343:392–398
Vrijland WW, van den Tol MP, Luijendijk RW, Hop WC, Busschbach JJ, de Lange DC et al (2002) Randomized clinical trial of non-mesh versus mesh repair of primary inguinal hernia. Br J Surg 89:293–297
Gilbert AI, Felton LL (1993) Infection in inguinal hernia repair considering biomaterials and antibiotics. Surg Gynecol Obstet 177:126–130
Montgomery A, Kallinowski F, Köckerling F (2015) Evidence for replacement of an infected synthetic by a biological mesh in abdominal wall hernia repair. Front Surg 2(67):1 – 6
Amato B, Moja L, Panico S, Persico G, Rispoli C, Rocco N, Moschetti I (2012) Shouldice technique versus other open techniques for inguinal hernia repair. Cochrane Database Syst Rev (4):CD001543
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Conception and design: SH. Data collection: DAF, VAM, and SH. Analysis and interpretation: DAF and SH. Writing the article: DAF and SH. Critical revision of the article: DAF and SH. Final approval of the article: DAF, VAM and SH. Statistical analysis: SH.
Corresponding author
Ethics declarations
Conflict of interest
DAF declares no conflict of interest. VAM declares no conflict of interest. SH declares no conflict of interest.
Ethical approval
This was deemed to not be required.
Human and animal rights
This article does not contain any direct involvement of human participants as it is comprised of data from papers already published.
Informed consent
Informed consent was not necessary for this study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Search no. | Search strategya |
|---|---|
#1 | darn: TI,AB,KW |
#2 | darning: TI,AB,KW |
#3 | modified near2 darn*: TI,AB,KW |
#4 | #1 OR #2 OR #3 |
#5 | mesh: TI,AB,KW |
#6 | lichtenstein: TI,AB,KW |
#7 | #5 OR #6 |
#8 | MeSH descriptor: [inguinal hernia] explode all trees |
#9 | inguinal hernia: TI,AB,KW |
#10 | #8 OR #9 |
#11 | #4 AND #7 AND #10 |
Rights and permissions
About this article

Cite this article
Finch, D.A., Misra, V.A. & Hajibandeh, S. Open darn repair vs open mesh repair of inguinal hernia: a systematic review and meta-analysis of randomised and non-randomised studies. Hernia 23, 523–539 (2019). https://doi.org/10.1007/s10029-019-01892-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-019-01892-1