
Abstract
Purpose
Inguinal hernioplasty could be used as an indicator of the surgical quality offered in different health institutions and countries, thereby establishing a scientific basis from which the procedure can be critically assessed and ultimately improved. Quality assessment of hernioplasties could be conducted using two different methods: either analyzing dedicated regional/national databases (DD) or reviewing administrative databases (AD).
Methods
A retrospective study of inguinal hernioplasties was carried out in the Emilia-Romagna hospitals between 2000 and 2009. Data were obtained by analyzing Hospital Discharge records regional Databases (HDD). Descriptive and multivariate statistical analysis was performed.
Results
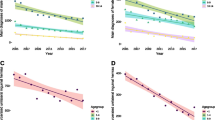
126,913 inguinal hernioplasty procedures were performed. The annual rate was on average 34 per 10,000 inhabitants. An increase of the case mix complexity and relevant changes in procedure technique were recorded. From multivariate analysis, the following independent factors related to a hospitalization longer than 1 day emerged: procedures in urgent setting (OR 3.6, CI 3.4–3.7), Charlson’s score ≥2 (OR 3.4, CI 3.1–3.7), laparoscopy (OR 2.1, CI 1.9–2.3), no mesh use (OR 2.1, CI 2–2.3), age >65 years (OR 1.9, CI 1.8–1.9), associated interventions (OR 1.9, CI 1.8–1.9), bilateral hernia (OR 1.7, CI 1.6–1.8), recurrent hernia (OR 1.2, CI 1.1–1.2) and female gender (OR 1.2, CI 1.2–1.3). Factors related to non-prosthetic hernioplasty were: bilateral hernia (OR 2.7, CI 2.5–2.9), female gender (OR 1.8, CI 1.8–2.0), emergency setting (OR 1.6, CI 1.5–1.8), recurrences (OR 1.5, CI 1.4–1.6) and associated interventions (OR 1.5, CI 1.4–1.6).
Conclusion
Inguinal hernia should be treated as an outpatient procedure in the majority of patients. Precise guidelines are necessary. HDD demonstrated to be a good and trustworthy system to collect clinical data. When precise guidelines are lacking, legal/institutional indications play a pivotal role in shifting the hernia surgery toward a one-day surgery regimen.


Similar content being viewed by others


References
Phillips W, Goldman M (2004) Groin Hernia. From “Health care needs assessment, the epidemiologically based needs assessment reviews” First Series, Vol 1, 2nd edn., Radcliffe Publishing UK
Lichtenstein IL, Shulman AG, Amid PK, Montlor MM (1989) The tension-free hernioplasty. Am J Surg 157:188–193
Scott N, Go PMNYH, Graham P, McCormack K, Ross SJ, Grant AM (2001) Open mesh vs non-mesh for groin hernia repair. Cochrane database of systematic reviews, issue 3. Art. No.:CD002197
Nilsson E, Haapaniemi S (1998) Hernia registers and specialization. Surg Clin North Am 78:1141–1155
Bay-Nielsen M, Kehlet H (1999) Establishment of a national Danish hernia data base: preliminary report. Hernia 3:81–83
Charlson ME, Pompei P, Ales K, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chron Dis 40:373–383
Halligan A, Donaldson L (2002) The meaning and implementation of clinical governance. G Ital Nefrol 19(suppl 21):S8–S13
Thompson RG, Donaldson LJ (1990) Medical audit and the wider quality debate. J Public Health Med 12:149–151
Koch A, Edwards A, Haapaniemi S, Nordin P, Kald A (2005) Prospective evaluation of 6,895 groin hernia repair in women. Br J Surg 92:1553–1558
Bay-Nielsen M, Kehlet H, Strand L et al (2001) Quality assessment of 26,304 herniorrhaphies in Denmark: a prospective nationwide study. Lancet 358:1124–1128
Haapaniemi S (2001) Quality assessment in groin hernia surgery—the role of a register. Medical dissertation no. 695. University of Linkoping: Linkoping
Nilsson E, Haapaniemi S (2002) Assessing the quality of hernia repair. In: Fitzgibbons RJ Jr, Greenburg AG (eds) Nyhus and Condon’s Hernia (5th edn). LippincottWilliams and Wilkins, Philadelphia, pp 567–573
O’Riordan DC, Kingsnorth AN (1998) Audit of patient outcomes after herniorrhaphy. Surg Clin North Am 78:1129–1139
National guideline cleringhouse. Work loss data institute. Hernia. Corpus Christi (TX): work loss data institute; 2006
Hair A, Duffy K, McLean J et al (2000) Groin hernia repair in Scotland. Br J Surg 87:1722–1726
McCormack, Wake B, Perez J et al (2005) Laparoscopic surgery for inguinal hernia repair: systematic review of effectiveness and economic evaluation. Health Technology Assessment Vol 9: No. 14
National institute for clinical excellence. (2004) Laparoscopic surgery for inguinal hernia repair. NICE technology appraisal guidance no. 83. National institute for clinical excellence, London
Association of surgeons of the Netherlands (2003) Dutch guidelines for inguinal hernia repair. Van Zuiden Communications BV, Alphen
Simmons MP, deLange D, Beetsw GL, van Geldere D, Heij HA, Go PM (2001) The “Inguinal Hernia” guideline of the association of surgeons of the Netherlands. Ned Tijdschr Geneeskd 147:2111–2117
de Lange DH, Aufenacker ThJ, Roest M, Simmermacher RKJ, Gouma DJ, Simons MP (2005) Inguinal hernia surgery in the Netherlands: a base line study before the introduction of the Dutch guidelines. Hernia 9:172–177
McCormack K, Scott NW, Go PM, Ross S, Grant AM On behalf of the EU hernia trialists collaboration (2003) Laparoscopic techniques versus open techniques for inguinal repair (review). Cochrane database of systematic reviews, issue 1. Art. No. CD001785
Report of a working party convened by the Royal College of Surgeon of England. Clinical guidelines on the management of groin hernias in adult. London: RCS, 1993
Mokete M, Earnshaw JJ (2001) Evolution of an inguinal hernia surgery practice. Postgrad Med J 77:188–190
Bay-Nielsen M, Nilsson E, Nordin P, Kehlet H (2004) Swedish Hernia Database the Danish Hernia Database. Chronic pain after open mesh and sutured repair of indirect inguinal hernia in young males. Br J Surg 91(10):1372–1376
Rosenberg J, Bisgaard T, Kehlet H, Wara P, Asmussen T, Juul P, Strand L, Andersen FH, Bay-Nielsen M.(2011) Danish Hernia Database. Danish Hernia Database recommendations for the management of inguinal and femoral hernia in adults. Dan Med Bull;58(2):C4243
Lundström KJ, Sandblom G, Smedberg S, Nordin P (2012) Risk factors for complications in groin hernia surgery: a national register study. Ann Surg 255(4):784–788
Schmidt CO, Kohlmann T (2008) When to use the odds ratio or the relative risk? Int J Public Health. 53(3):165–167
Acknowledgments
We dedicate this work to Orazio Campione, Professor of Surgery and Head of Emergency Surgery Department of the S.Orsola-Malpighi Hospital (University of Bologna, Italy) from 1995, who passed away prematurely in August 2003. We also want to thank Daniel Lazzareschi, from the department of Integrative Biology of the Berkeley University (USA), for the precious work of text editing.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ansaloni, L., Coccolini, F., Fortuna, D. et al. Assessment of 126,913 inguinal hernia repairs in the Emilia-Romagna region of Italy: analysis of 10 years. Hernia 18, 261–267 (2014). https://doi.org/10.1007/s10029-013-1091-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-013-1091-x