
Abstract
Background
Repair of primary and recurrent giant incisional herniae is extremely challenging and more so in the face of surgical field contamination. Literature supports the single- and multi-staged approaches including the use of biological meshes for these difficult patients with their associated benefits and limitations.
Patients and methods
This is a retrospective analysis of a prospective study of five patients who were successfully treated through a multi-staged approach but in the same hospital admission, not previously described, for the repair of contaminated primary and recurrent giant incisional herniae in a district general hospital between 2009 and 2012. Patient demographics including their BMI and ASA, previous and current operative history including complications and follow-up were collected in a secure database. The first stage involved the eradication of contamination, and the second stage was the definitive hernia repair with the new generation-coated synthetic meshes.
Results
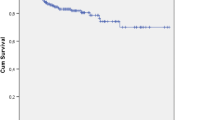
Of the five patients, three were men and two women with a mean age of 58 (45–74) years. Two patients had grade 4 while the remaining had grade 3 hernia as per the hernia grading system with a mean BMI of 35 (30–46). All patients required extensive adhesiolysis, bowel resection and anastomoses and wash out. Hernial defect was measured as 204* (105–440) cm2, size of mesh implant was 568* (375–930) cm2 and the total duration of operation (1st + 2nd Stage) was 354* (270–540) min. Duration of hospital stay was 11* (7–19) days with a follow-up of 17* (6–36) months.
Conclusion
We believe that our multi-staged approach in the same hospital admission (for the repair of contaminated primary and recurrent giant incisional herniae), excludes the disadvantages of a true multi-staged approach and simultaneously minimises the risks and complications associated with a single-staged repair, can be adopted for these challenging patients for a successful outcome (* indicates mean).





Similar content being viewed by others


Notes
* mean.
References
Cobb WS, Kercher KW, Heniford BT (2005) Laparoscopic repair of incisional hernias. Surg Clin North Am 85:91–103
Millikan KW (2003) Incisional hernia repair. Surg Clin North Am 83:1223–1234
Luijendijk RW, Hop WCJ, van den Tol MP et al (2000) A comparison of suture repair with mesh repair for incisional hernia. N Engl J Med 343:392–397
Campanelli G, Catena F, Ansaloni L (2008) Prosthetic abdominal wall hernia repair in emergency surgery: from polypropylene to biological meshes. World J Emerg Surg 3:33
Catena F, Ansaloni L, Gazzotti F et al (2007) Use of porcine dermal collagen graft (permacol) for hernia repair in contaminated fields. Hernia 11:57–60
Loganathan A, Ainslie WG, Wedgewood KR (2010) Initial evaluation of Permacol bioprosthesis for the repair of complex incisional and parastomal hernias. Surgeon 8:202–205
Shrestha AK, Abd ELsayed SE, Bin Saeid J, Basu S (2012) Repair of giant abdominal incisional hernia: our technique. Ann R Coll Surg Engl 94:13–14
Ramirez OM, Ruas E, Dellon AL (1990) “Components separation” method for closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg 86:519–526
Buinewicz B, Rosen B (2004) Acellular cadaveric dermis (Alloderm): a new alternative for abdominal hernia repair. Ann Plast Surg 52:188–194
van Geffen HJ, Simmermacher RK, van Vroonhoven TJ et al (2005) Surgical treatment of large contaminated abdominal wall defects. J Am Coll Surg 201:206–212
Alaedeen DI, Lipman J, Medalie D et al (2007) The single-staged approach to the surgical management of abdominal wall hernias in contaminated fields. Hernia 11:41–45
Dayton MT, Buchele BA, Shirazi SS et al (1986) Use of an absorbable mesh to repair contaminated abdominal wall defects. Arch Surg 121:954–960
Fansler RF, Taheri P, Cullinane C et al (1995) Polypropylene mesh closure of the complicated abdominal wound. Am J Surg 170:15–18
Campanelli G, Nicolosi FM, Pettinari D (2004) Prosthetic repair, intestinal resection and potentially contaminated areas: safe and feasible? Hernia 8:190–192
Itani K, Rosen M, Vargo D, et al (2010) Multicenter clinical study of Single stage repair of large contaminated hernia defects with Strattice reconstructive tissue matrix reinforcement of component separation. Hernia 14(Suppl 1):11
van Geffen HJ, Simmermacher RK, van Vroonhoven TJ et al (2005) Surgical treatment of large contaminated abdominal wall defects. J Am Coll Surg 201:206–212
Cavallaro A, Lo Menzo E, Di Vita M et al (2010) Use of biological meshes for abdominal wall reconstruction in highly contaminated fields. World J Gastroenterol 16:1928–1933
Diaz JJ Jr, Guy J, Berkes MB et al (2006) Allograft for ventral hernia repair in the contaminated surgical field. Am Surg 72:1187–1188
Ueno T, Pickett LC, de la Fuente SG et al (2004) Clinical application of porcine small intestinal submucosa in the management of infected or potentially contaminated abdominal defects. J Gastrointest Surg 8:109–112
Bleichordt RP, de Vries Reilingh TS, Malyar AW et al (2004) Compartment separation technique to repair large midline hernias. Op Tech Gen Surg 6:179–188
Leber GE, Garb JL, Alexander AI et al (1998) Long-term complications associated with prosthetic repair of incisional hernias. Arch Surg 133:378–382
Fabian TC, Croce MA, Pritchard FE et al (1994) Planned ventral hernia. Staged management for acute abdominal wall defects. Ann Surg 219:643–650
Jernigan TW, Fabian TC, Croce MA et al (2003) Staged management of giant abdominal wall defects: acute and long-term results. Ann Surg 238:349–355
Baker S, Millard DR Jr (1995) Two-staged adbomonal wall reconstruction of sepsis-induced dehiscence. Plast Reconstr Surg 96:898–904
Gilbert AI, Graham MF (1997) Infected grafts of incisional hernioplasties. Hernia 1:77–81
de Vries Reiling TS, van Goor H, Charbon JA et al (2007) Repair of giant midline abdominal wall hernias: “components separation technique” versus prosthetic repair: interim analysis of a randomized controlled trial. World J Surg 31:756–763
LeBlanc KA, Elieson MJ, Corder JM (2007) Enterotomy and mortality rates of laparoscopic incisional and ventral hernia repair: a review of the literature. JSLS 11(4):408–414
Hodde J (2002) Naturally occurring scaffolds for soft tissue repair and regeneration. Tissue Eng 8:295–308
Bauer JJ, Harris MT, Gorfine SR et al (2002) Rives-Stoppa procedure for repair of large incisional hernias: experience with 57 patients. Hernia 6:120–123
Stoppa RE (1989) The treatment of complicated groin and incisional hernias. World J Surg 13:545–554
Vix J, Meyer Ch, Rohr S et al (1997) The treatment of incisional and abdominal hernia with a prosthesis in potentially infected tissues—a series of 47 cases. Hernia 1:157–161
Wantz GE (1998) Giant prosthetic reinforcement of the visceral sac. Surg Clin North Am 78:1075–1087
Conflict of interest
All authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Siddique, K., Shrestha, A. & Basu, S. Multi-staged repair of contaminated primary and recurrent giant incisional herniae in the same hospital admission: a proposal for a new approach. Hernia 18, 57–63 (2014). https://doi.org/10.1007/s10029-013-1051-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-013-1051-5