
Abstract
Purpose
This prospective, randomized, double-blind study compared the analgesic efficacy and safety of parecoxib sodium versus lornoxicam and diclofenac, after Lichtenstein tension-free mesh inguinal hernia repair.
Methods
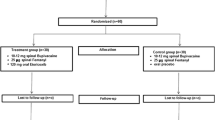
Patients were randomly assigned to receive parecoxib 80 mg daily i.v. (Group A), lornoxicam 16 mg daily i.v. (Group B) or diclofenac 150 mg daily i.m. (Group C). Rescue analgesia in all groups consisted of pethidine 25 mg i.m. Pain was measured with an analogue scale (pain intensity score).
Results
Patients treated with parecoxib 80 mg reported significantly lower summed pain intensity scores compared with lornoxicam and diclofenac-treated patients. Duration of analgesia was also significantly longer with parecoxib than with lornoxicam and diclofenac. Adverse events were significantly less common in the parecoxib and lornoxicam group, compared with diclofenac group.
Conclusions
Multiple-day administration of parecoxib 40 mg twice daily is more effective than equivalent doses of lornoxicam and diclofenac, and generally better tolerated than diclofenac after Lichtenstein tension-free mesh inguinal hernia repair.

Similar content being viewed by others


References
Bisgaard T, Klarskov B, Rosenberg J et al (2001) Characteristics and prediction of early pain after laparoscopic cholecystectomy. Pain 90:261–269
Stichtenoth DO, Frolich JC (2003) The second generation of COX-2 inhibitors: what advantages do the newest offer? Drugs 63:33–45
McMurray RW, Hardy KJ (2002) COX-2 inhibitors: today and tomorrow. Am J Med Sci 323:181–189
Emery P, Zeidler H, Kvien TK, Guslandi M, Naudin R, Stead H, Verburg KM, Isakson PC, Hubbard RC, Geis GS (1999) Celecoxib versus diclofenac in long-term management of rheumatoid arthritis: randomised double-blind comparison. Lancet 354(9196):2106–2111
Deeks J, Smith L, Bradley M (2002) Efficacy, tolerability, and upper gastrointestinal safety of celecoxib for treatment of osteoarthritis and rheumatoid arthritis: systematic review of randomised controlled trials. BMJ 325:619
Rasmusen G, Steckner K, Hogue C et al (2002) Intravenous parecoxib sodium for acute pain after orthopedic knee surgery. Am J Orthop 31:336–343
Barton S, Langeland F, Snabes M et al (2002) Efficacy and safety of intravenous parecoxib sodium in relieving acute postoperative pain following gynecologic laparotomy surgery. Anesthesiology 96:306–314
Vane JR (1971) Inhibition of prostaglandin synthesis as a mechanism of action of aspirin-like drugs. Nat New Biol 231:232–235
Masferrer JL, Zweifel BS, Seibert K et al (1990) Selective regulation of cellular cyclooxygenase by dexamethasone and endotoxin in mice. J Clin Invest 86:1375–1379
Xie W, Chipman JG, Robertson DL et al (1991) Expression of a mitogen-responsive gene encoding prostaglandin synthase is regulated by mRNA splicing. Proc Natl Acad Sci USA 88:2692–2696
Beiche F, Scheuerer S, Brune K et al (1996) Upregulation of cyclooxygenase-2 mRNA in the rat spinal cord following peripheral inflammation. FEBS Lett 390:165–169
Bombardier C, Laine L, Reicin A et al (2000) Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. VIGOR Study Group. N Engl J Med 343:1520–1528
Schnitzer TJ, Burmester GR, Mysler E et al (2004) Comparison of lumiracoxib with naproxen and ibuprofen in the therapeutic arthritis research and gastrointestinal event trial (TARGET), reduction in ulcer complications: randomised controlled trial. Lancet 364:665–674
Silverstein FE, Faich G, Goldstein JL, Simon LS, Pincus T, Whelton A et al (2000) Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: the CLASS study: a randomized controlled trial. Celecoxib Long-term Arthritis Safety Study. J Am Med Assoc 284:1247–1255
Chan FK, Hung LC, Suen BY et al (2002) Celecoxib versus diclofenac and omeprazole in reducing the risk of recurrent ulcer bleeding in patients with arthritis. N Engl J Med 347:2104–2110
Lai KC, Chu KM, Hui WM et al (2005) Celecoxib compared with lansoprazole and naproxen to prevent gastrointestinal ulcer complications. Am J Med 118:1271–1278
Rodrigues AD, Halpin RA, Geer LA, Cui D, Woolf EJ, Matthews CZ, Gottesdiener KM, Larson PJ (2003) Absorption, metabolism, and excretion of etoricoxib, a potent and selective cyclooxygenase-2 inhibitor, in healthy male volunteers. Drug Metab Dispos 31:224–232
Esser R, Berry C, Du Z et al (2005) Preclinical pharmacology of lumiracoxib: a novel selective inhibitor of cyclooxygenase-2. Br J Pharmacol 144:538–550
Szczeklik A, Nizankowska E, Bochenek G et al (2001) Safety of a specific COX2 inhibitor in aspirin-induced asthma. Clin Exp Allergy 31:219–225
Farkouh ME, Kirshner H, Harrington RA et al (2004) Comparison of lumiracoxib with naproxen and ibuprofen in the therapeutic arthritis research and gastrointestinal event trial (TARGET), cardiovascular outcomes: randomised controlled trial. Lancet 364:675–684
Capone ML, Tacconelli S, Sciulli MG et al (2004) Clinical pharmacology of platelet, monocyte, and vascular cyclooxygenase inhibition by naproxen and low-dose aspirin in healthy subjects. Circulation 109:1468–1471
Meagher EA (2004) Cardiovascular and renovascular implications of COX-2 inhibition. Curr Pharm Des 10:603–611
Viscusi E, Gimbel J, Halder A et al (2008) A multiple-day regimen of parecoxib sodium 20 mg twice daily provides pain relief after total hip arthroplasty. Anesth Analg 107:652–660
Joshi GP, Viiscusi ER, Gan TJ et al (2004) Effective treatment of laparoscopic cholecystectomy pain with intravenous followed by oral COX-2 specific inhibitor. Anesth Analg 98:336–342
Papadima A, Lagoudianakis E, Antonakis P et al (2007) Parecoxib vs. Lornoxicam in the treatment of postoperative pain after laparoscopic cholecystectomy: a prospective randomized placebo-controlled trial. Eur J Anaesthesiol 24(2):154–158
Tang J, Li S, White PF, Chen X, Wender RH, Quon R, Sloninsky A, Naruse R, Kariger R, Webb T, Norel E (2002) Effect of parecoxib, a novel intravenous cyclooxygenase type-2 inhibitor, on the postoperative opioid requirement and quality of pain control. Anesthesiology 96(6):1305–1309
Nussmeier NA, Whelton AA, Brown MT et al (2006) Safety and efficacy of the cyclooxygenase-2 inhibitors parecoxib and valdecoxib after noncardiac surgery. Anesthesiology 104(3):518–526
Beaussier M, Weickmans H, Paugam C et al (2005) A randomized, double-blind comparison between parecoxib sodium and propacetamol for parenteral postoperative analgesia after inguinal hernia repair in adult patients. Anesth Analg 100:1309–1315
Kranke P, Morin A, Roewer N et al (2004) Patients’ global evaluation of analgesia and safety of injected parecoxib for postoperative pain: a quantitative systematic review. Anesth Analg 99:797–806
Narchi P, Carry PY, Catoire P (1998) Postoperative pain relief and recovery with ropivacaine infiltration after inguinal hernia repair. Ambul Surg 6(4):221–226
Aasbø V, Thuen A, Ræder J (2002) Improved long-lasting postoperative analgesia, recovery function and patient satisfaction after inguinal hernia repair with inguinal field block compared with general anesthesia. Acta Anaesth Scand 46(6):674–678
Harrison CA, Morris S, Harvey JS (1994) Effect of ilioinguinal and iliohypogastric nerve block and wound infiltration with 0.5% bupivacaine on postoperative pain after hernia repair. Brit J Anaesth 72(6):691–693
Vintar N, Pozlep G, Rawal N, Godec M, Rakovec S (2002) Incisional self-administration of bupivacaine or ropivacaine provides effective analgesia after inguinal hernia repair. Can J Anesth 49(5):481–486
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kyriakidis, A.V., Perysinakis, I., Alexandris, I. et al. Parecoxib sodium in the treatment of postoperative pain after Lichtenstein tension-free mesh inguinal hernia repair. Hernia 15, 59–64 (2011). https://doi.org/10.1007/s10029-010-0737-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-010-0737-1