
Abstract
To compare the accuracy of cone beam CT scanning (NewTom 3G) with intraoral periapical radiography (Dixi2, Planmeca CCD sensor and Insight film) for the detection of periapical bone defects. Ten frozen pig mandibles were used. All soft tissues were removed and the jaws were sagittally sectioned to obtain three blocks from each side of the jaw containing the premolars and the molars with surrounding jaw bone. All teeth with intact roots were then “extracted”. First, 15 blocks were used to define defect size and exposure parameters; then, the remaining 45 blocks were divided into three equal groups. In one group, cylindrical defects of 1 × 1 mm were prepared beyond the apices of the extraction sockets, in another group defects of 2 × 2 mm were similarly prepared, while no defects were prepared in the last group. The teeth were replaced into their sockets and digital and conventional radiographs of all blocks were taken under reproducible conditions. In addition, all blocks were CT scanned with the same volumetric data and then reconstructed to provide sagittal and coronal 2-D sections. Masked evaluation of the images (defect present vs no defect) was performed by four calibrated examiners. Statistical analysis was performed with ANOVA and the significance level was set to P < 0.05. NewTom 3G was statistically significantly better in terms of sensitivity (54%), positive (82.6%) and negative (44.5%) predictive values, and diagnostic accuracy (61%) when compared with digital radiographs (23%, 60%, 31%, 39%), and with conventional ones (28%, 70%, 35%, 44%)—except in the positive predictive value. Specificity was similar for all three methods. No difference was observed between the two periapical (digital vs conventional) radiographs. NewTom 3G may be useful in cases of immediate implants intended to replace teeth with suspicion for possible existing endodontic pathology, or in candidate implant sites neighboring such teeth.
Similar content being viewed by others

Introduction
Prosthetic rehabilitation by means of endosseous titanium implants has become a routine treatment modality. Among other factors, the presence of sufficient alveolar bone volume is considered a prerequisite for implant placement and integration, and subsequent success; thus, the original surgical protocol advocated long healing periods after tooth extraction before implant placement (for review, see [31]). In recent years, however, it has become evident that postponing implant installation after tooth removal may not be a critical factor per se for their osseointegration, since the success rate of implants installed shortly or immediately after tooth extraction has been demonstrated to be similar to those installed in completely healed sockets (for review, see [8, 19]). On the other hand, due to inconclusive information, it is currently suggested that in case of the presence of infection associated with the tooth to be extracted, immediate implant installation should not be performed [19]. This, in turn, implies that in such cases implant surgery should be postponed until healing of the extraction site is concluded several months after tooth removal.
In a recent retrospective analysis, however, a higher incidence of early failures and/or complications (e.g. apical peri-implantitis) of implants inserted in sites with a history of a periapical granuloma or in the neighborhood of teeth with endodontic pathology was observed [25]. In addition, implant failures/complications linked to periapical pathology of neighboring asymptomatic or endodontically treated teeth with no radiographic evidence of failure were previously reported [6, 7, 29]. It seems, thus, that knowledge of the presence or absence of existing periapical tooth pathology is essential both when immediate implant installation is considered and in implant treatment planning in general.
Diagnosis of the presence/absence of endodontic/periapical pathology is largely based on periapical radiographic examination. The ability of detecting a periapical bone lesion radiographically depends among other factors on the localization (i.e. involving trabecular and/or cortical bone) and size (i.e. amount of bone destruction in relation to the dimensions of the jaw at the particular site) of the defect [1, 3–5, 16, 28]. Several studies showed that the diagnostic accuracy of detecting periapical bone defects/lesions in digital intraoral radiographs is at least as high as that of conventional film [1, 20, 30, 34], while manipulation of digitized, poor quality film radiographs may indeed enhance diagnostic accuracy [33]. Existing studies have failed to find differences among the various intraoral digital systems [9, 14]. However, technological advancement in digital imaging, imaging software and computer systems warrants continuous testing of their performance.
Computed tomography (CT) technology overcomes the inherent disadvantage of conventional radiography in which 3-D structures are presented as 2-D images. CT was shown to be superior to periapical radiography in identifying various type of bone defects, including periapical ones [10–12, 15, 30, 32]. A drawback of medical CT is the high dose compared to periapical radiography together with high costs and availability. However, the introduction of dental cone beam CT (CBCT) [21], which provides radiation doses of approximately 50–70 times less than medical CT scanners [17, 21], has facilitated 3-D examination of the teeth and jaws.
The aim of the present study was to compare the accuracy of CBCT (NewTom 3G) with intraoral periapical radiography (Dixi2, Planmeca CCD sensor and Insight film) for the detection of simulated (i.e. mechanically prepared) periapical bone defects in dry pig jaws.
Materials and methods
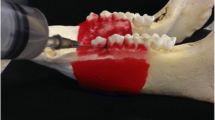
Ten frozen mandibles from young adult pigs were used in the present study. After boiling the mandibles twice for 8 h, all soft tissues (gingiva, mucosa, muscles) including marrow and fat were removed and the jaws were sagitally sectioned by means of a band saw to obtain three blocks from each side of the mandible (i.e. 60 blocks in total) containing the premolars and the molars with surrounding jawbone (Fig. 1a). Care was taken so that the blocks from the left and right side of the jaw were similar to each other in terms of size and number of teeth. Thereafter, all teeth with roots not destroyed by the sawing procedure (i.e. completely surrounded by bone) were carefully extracted with a pair of forceps.

Blocks of specimens containing the teeth and surrounding bone were prepared (a) and after careful “extraction” of the teeth (b), cylindrical defects (arrow) were created beyond the apices of the extraction sockets (one defect per block) by means of a pillar drill (c)
To determine the size of the defect, which in the present model is readily detectable in the periapical conventional film (Insight, Eastman Kodak Company, Rochester, NY, USA) and the suitable exposure parameters, cylindrical defects 1 × 1 mm, 2 × 2 mm, and 3 × 3 mm were randomly prepared beyond the apices of the extraction sockets in 15 blocks (one defect per block) by means of a pillar drill (Fig. 1b and c). Then, the teeth were replaced in their sockets and the blocks were radiographed under standardized conditions (Gendex DC X-ray unit; Gendex, Des Plaines, IL, USA) with rectangular collimation operating at 65 kVp and 10 mA, a target-to-film distance of 32 cm, a central beam orientation and 2 cm block-receptor distance) using various exposure parameters. Masked evaluation of the radiographs revealed that the 3 × 3 mm defects were easy to recognize; therefore, it was decided to use only 1 × 1 mm and 2 × 2 mm defects in the study. Exposure time was set to 0.34 s.
Thereafter, the remaining 45 blocks were coded and divided into three groups equal in number and similar in the amount of premolar and molar teeth available in the blocks. In one group (test 1), defects of 1 × 1 mm were prepared as described above. In the second group (test 2), defects of 2 × 2 mm were prepared, while no defects were prepared in the third group (control). All teeth were then replaced into their sockets, and conventional film and CCD sensor based digital radiographs (Dixi2, Planmeca, Oy, Helsinki, Finland) of all blocks were obtained. Thereafter, all blocks were examined by CBCT (NewTom 3G, Quantitative Radiology, Verona, Italy) with a 6 in. field of view. The volumetric data were reconstructed to provide serial coronal and sagittal 1 mm thick sections with 0.5 mm interval (Fig. 2a and b).

Consecutive coronal (a) and sagittal (b) sections were produced from the CBCT examination and incorporated in single images of 12 sections per image. The computer program, used in the evaluation of the images, had a zoom function and image enhancement facilities (e.g. contrast, brightness) (c)
Evaluation of the presence of a defect was dichotomous, yes/no. The conventional film radiographs were examined on a light-box with an X-ray viewer while the digital images were assessed on a 19 in. quality computer monitor using a custom-made program (CaScO, Erik Gotfredsen, School of Dentistry, University of Aarhus, Denmark) that had a zoom function and image enhancement facilities, contrast, brightness and gamma curve functions (Fig. 2c). Four previously calibrated examiners evaluated the images separately and masked. Statistical analysis was performed by two-way analysis of variance between observers and methods and post hoc t tests tested differences in sensitivity, specificity, positive and negative predictive values and overall accuracy (i.e. true positive + true negative: TP + TN). The significance level was set to P < 0.05.
Results
The analysis showed no significant differences between test groups 1 and 2 (1 mm and 2 mm defects), nor among the examiners (data not shown). Therefore, the data from all examiners and the two test groups were averaged and are presented in Table 1.
A statistically significant difference in sensitivity was observed between NewTom 3G images and Insight film (P = 0.001) and between NewTom 3G images and Dixi2 images (P = 0.002), but there was no difference between digital and conventional (P = 0.34) intraoral radiographs. No difference in specificity between the three methods was observed (NewTom 3G vs Insight film, P = 0.83; NewTom 3G vs Dixi2, P = 0.52; Dixi2 vs Insight film, P = 0.40). The positive predictive value (PPV) for the NewTom 3G was significantly higher than for Dixi2 (P = 0.006), but marginally non-significant compared to Insight film (P = 0.06). There was no significant difference between film and digital intraoral radiographs regarding PPV (P = 0.11). The negative predictive value (NPV) of NewTom 3G was significantly higher than that of intraoral radiographs (P = 0.02) while there was no significant difference between the two latter methods (P = 0.30). The diagnostic accuracy of NewTom 3G was significantly higher than that of intraoral radiographs (P = 0.006), but again no differences could be observed between the latter two methods (P = 0.21).
Discussion
The results of the present study showed that NewTom 3G obtained twice as high a sensitivity as intraoral radiographs for the detection of mechanically created periapical defects in pig jaws without jeopardizing specificity. PPV and NPV were also higher, resulting in a significantly higher overall diagnostic accuracy (i.e. obtaining the correct diagnosis) with CBCT than with intraoral radiography, digital or conventional. PPV was relatively high for all modalities (i.e. the test results are very trustworthy), but this may not be surprising since this value is prevalence dependent, and a higher number of teeth with defects than without defects was included in the present study. It is unlikely, however, that this fact has created any bias in favor of one of the evaluated methods over the others. In this context, one may argue that due to their “normalized” shape, the cylindrical defects evaluated in the present study are probably easier to identify than naturally occurring periapical lesions, which have rather diffused borders. Indeed, this fact may have somehow contributed to the high PPV values observed here and it is possible that lower PPV values may be expected/obtained in the clinic.
The findings are in accordance with previous results where conventional medical CT was found to be superior to periapical radiography in identifying various types of artificially created bone defects (including periapical ones) [10–12, 15] or bone lesions of endodontic origin [30, 32]. Fuhrmann et al. [10], for instance, produced mechanical defects of varying dimensions in the antral floor adjacent to 40 roots of maxillary premolars and molars in human autopsy specimens. Periapical radiographs and 1 mm axial high resolution CT scans of all specimens were obtained, and the radiolographic findings of both sets of images were compared to the known sites of the defects. None of the created bone defects could be identified on the intraoral radiographs, while 62.5% could indeed be identified in the CT scans. However, a control group with no defects was not included in that study. In a clinical study, Velvart et al. [32] performed periapical radiography and high resolution CT examination of 50 mandibular premolars or molars (80 roots) with clinical signs of persistent apical periodontitis, displaying a failing root canal treatment (i.e. the endodontic treatment was either already performed but had failed, or was not feasible because of canal obstruction, or the patient had refused to sacrifice the coronal restoration for re-treatment). The presence or absence of a periapical lesion was evaluated in the radiographs and the CT scans, and the results were correlated to the observations made during endodontic/periapical surgery. The authors reported that the 78 defects discovered during surgery, could also be identified in the CT scans, while only 79% of those were discernible in the periapical radiographs.
It may be expected that CT examination is indeed better than intraoral radiography because the possible problem of projection of neighboring anatomical features over the area of interest is not present. Thus, the fact that the examiners in the above-mentioned studies knew in advance that defects truly existed (in the ex vivo studies) [10–12, 15] or were extremely probable (from the signs and symptoms in the clinical studies) [30, 32], may have led them to more readily “identify” the defects on the CT images. This may, in turn, also explain the higher sensitivity values observed in those studies compared to the present.
It was previously shown that identification of artificially created periapical defects not involving the cortical plates may be difficult [3, 4, 28] but not impossible [1, 5, 16] and that the detection rate actually depends on the relative amount of mineralized tissue loss compared to the total amount of mineralized tissue in the radiation field [2]. Obviously, the relative densities of the cortical plate and the trabecular bone on a given site are of importance in the possibility to detect a defect of given dimensions localized solely inside the trabecular compartment of the jaw. The relatively low sensitivity values of digital and film intraoral radiography observed in the present experiment may thus be due to the fact that the defects in the present study did not involve the cortical bone plate, but were located inside the very loose trabecular bone compartment of the pig jaws. The finding in the present study that no difference between digital and conventional intraoral radiographs could be observed, is in accordance with previous reports [1, 20, 30, 34].
Diagnosing accurately the presence or absence of a periapical lesion associated with a tooth to be extracted seems to be of importance in implant treatment planning. Although results from some animal and clinical studies showed that the survival rates of implants placed immediately/shortly after the extraction of teeth with root fractures, perforations and combined endodontic-periodontal problems are similar to that of implants placed in healed ridges [22–24], other studies showed somewhat lower success and/or survival rates [13, 26, 27]. In fact, due to lack of conclusive evidence, it is currently suggested that if infection is associated with the tooth to be extracted, immediate implant installation should be avoided [19]. In a retrospective analysis on 539 single implants published recently [25], it was found approximately 3–5 times higher frequency of history of endodontic pathologies (periapical lesion around the extracted tooth or around neighboring teeth) for early failed implants and/or implants with complications requiring surgical intervention (e.g. apical peri-implantitis) vs successful ones. Although it is mentioned in this study that only few implants were installed immediately after tooth extraction, no account is given on how many of these (if any) have failed. However, all implants developing apical peri-implantitis (approximately 30% of the failures) were placed at least 6 months after tooth extraction. Cases of failures/complications of implants placed in healed edentulous ridges, which could be linked to periapical pathology of neighboring asymptomatic or endodontically treated teeth with no radiographic evidence of failure were also previously reported [6, 7, 29].
On the other hand, it is not known whether there is a “threshold” for periapical lesion size beyond which there is a higher risk for developing complications around implants, and it may be that only lesions larger than the 2 × 2 mm cylindrical defects evaluated in the present study are clinically relevant. As already mentioned, the relative densities of the cortical plate and the trabecular bone in the periapical area are of importance in the ability to visualize a given defect. However, jaw bone defects of larger dimensions than 2 × 2 mm may be expected to be easily identifiable (at least in most of the cases) with intraoral radiography, as indeed confirmed in the initial part of the present study where the 3 × 3 mm defects were deemed easy to recognize. This assumption is corroborated by the results of a retrospective clinical evaluation where periapical defects of 3.6 mm wide on average, could readily be identified in conventional radiographs irrespective of their location in the jaw (i.e. involving only trabecular or also cortical bone) or in the mouth (i.e. anterior or posterior region) [18]. Obviously, no assumptions can be made regarding defects with dimensions between 2 × 2 mm and 3 × 3 mm.
Taking into consideration the discussion above and the finding in the present study that specificity for the NewTom 3G was not significantly different from the periapical techniques, and the facts that CBCT has a 3–7 times higher dose than film orthopantomograms traditionally used in implant treatment planning [17] and is a quite time-consuming method, it would be wrong to suggest that all patients intended for implant treatment should be examined with CBCT. However, it may be suggested that when teeth with diffuse symptoms or asymptomatic teeth with suspicion for endodontic pathology (e.g. inadequate root canal treatment, history of recurrent problems of endodontic etiology etc.) are intended to be replaced with immediate implants, or in case such teeth are neighbors to candidate implant sites, the use of the CBCT may be beneficial. Apart from the possibility of having a higher chance of accurately identifying the presence of an existing periapical lesion, CBCT may also provide additional information relative to implant treatment (e.g. appreciate anatomical features of importance, choose the size of the implant more accurately, better orientation during surgery etc).
In conclusion, the results of the present study show that the NewTom 3G has a higher sensitivity, PPV, and diagnostic accuracy than intraoral radiography, digital (Dixi2) or conventional radiographs when evaluating the presence of artificially created periapical bone defects. NewTom 3G may be useful in cases of immediate implants intended to replace teeth with suspicion for endodontic pathology, or in candidate implant sites neighboring such teeth.
References
Barbat J, Messer HH (1998) Detectability of artificial periapical lesions using direct digital and conventional radiography. J Endod 24:837–842
Bender IB (1997) Factors influencing the radiographic appearance of bony lesions. J Endod 23:5–14
Bender IB, Seltzer S (2003) Roentgenographic and direct observation of experimental lesions in bone: I. 1961. J Endod 29:702–706
Bender IB, Seltzer S (2003) Roentgenographic and direct observation of experimental lesions in bone: II. 1961. J Endod 29:707–712
Bianchi SD, Roccuzzo M, Cappello N, Libero A, Rendine S (1991) Radiological visibility of small artificial periapical bone lesions. Dentomaxillofac Radiol 20:35–39
Brisman DL, Brisman AS, Moses MS (2001) Implant failures associated with asymptomatic endodontically treated teeth. J Am Dent Assoc 132:191–195
Chaffee NR, Lowden K, Tiffee JC, Cooper LF (2001) Periapical abscess formation and resolution adjacent to dental implants: a clinical report. J Prosthet Dent 85:109–112
Chen ST, Wilson TG Jr, Hammerle CH (2004) Immediate or early placement of implants following tooth extraction: review of biologic basis, clinical procedures, and outcomes. Int J Oral Maxillofac Implants 19(Suppl):12–25
Folk RB, Thorpe JR, McClanahan SB, Johnson JD, Strother JM (2005) Comparison of two different direct digital radiography systems for the ability to detect artificially prepared periapical lesions. J Endod 31:304–306
Fuhrmann R, Bucker A, Diedrich P (1997) Radiological assessment of artificial bone defects in the floor of the maxillary sinus. Dentomaxillofac Radiol 26:112–116
Fuhrmann RA, Bucker A, Diedrich PR (1995) Assessment of alveolar bone loss with high resolution computed tomography. J Periodontal Res 30:258–263
Fuhrmann RA, Bucker A, Diedrich PR (1997) Furcation involvement: comparison of dental radiographs and HR-CT-slices in human specimens. J Periodontal Res 32:409–418
Grunder U, Polizzi G, Goene R, Hatano N, Henry P, Jackson WJ, Kawamura K, Kohler S, Renouard F, Rosenberg R, Triplett G, Werbitt M, Lithner B (1999) A 3-year prospective multicenter follow-up report on the immediate and delayed-immediate placement of implants. Int J Oral Maxillofac Implants 14:210–216
Kullendorff B, Nilsson M (1996) Diagnostic accuracy of direct digital dental radiography for the detection of periapical bone lesions. II. Effects on diagnostic accuracy after application of image processing. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 82:585–589
Langen HJ, Fuhrmann R, Diedrich P, Gunther RW (1995) Diagnosis of infra-alveolar bony lesions in the dentate alveolar process with high-resolution computed tomography. Experimental results. Invest Radiol 30:421–426
LeQuire AK, Cunningham CJ, Pelleu GB Jr (1977) Radiographic interpretation of experimentally produced osseous lesions of the human mandible. J Endod 3:274–276
Ludlow JB, Davies-Ludlow LE, Brooks SL (2003) Dosimetry of two extraoral direct digital imaging devices: NewTom cone beam CT and Orthophos Plus DS panoramic unit. Dentomaxillofac Radiol 32:229–234
Marmary Y, Koter T, Heling I (1999) The effect of periapical rarefying osteitis on cortical and cancellous bone. A study comparing conventional radiographs with computed tomography. Dentomaxillofac Radiol 28:267–271
Mayfield LJA (1999) Immediate, delayed and late submerged and transmucosal implants. In: Lang NP, Karring T, Lindhe J (eds) Proceedings of the 3rd European Workshop on Periodontology. Implant dentistry. Quintessence Publishing, Berlin, pp 520–534
Mistak EJ, Loushine RJ, Primack PD, West LA, Runyan DA (1998) Interpretation of periapical lesions comparing conventional, direct digital, and telephonically transmitted radiographic images. J Endod 24:262–266
Mozzo P, Procacci C, Tacconi A, Martini PT, Andreis IA (1998) A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. Eur Radiol 8:1558–1564
Novaes Junior AB, Novaes AB (1995) Immediate implants placed into infected sites: a clinical report. Int J Oral Maxillofac Implants 10:609–613
Novaes Junior AB, Vidigal Junior GM, Novaes AB, Grisi MF, Polloni S, Rosa A (1998) Immediate implants placed into infected sites: a histomorphometric study in dogs. Int J Oral Maxillofac Implants 13:422–427
Pecora G, Andreana S, Covani U, De Leonardis D, Schifferle RE (1996) New directions in surgical endodontics; immediate implantation into an extraction site. J Endod 22:135–139
Quirynen M, Vogels R, Alsaadi G, Naert I, Jacobs R, van Steenberghe D (2005) Predisposing conditions for retrograde peri-implantitis, and treatment suggestions. Clin Oral Implants Res 16:599–608
Reiser GM, Nevins M (1995) The implant periapical lesion: etiology, prevention, and treatment. Compend Contin Educ Dent 16:768, 770, 772
Rosenquist B, Grenthe B (1996) Immediate placement of implants into extraction sockets: implant survival. Int J Oral Maxillofac Implants 11:205–209
Schwartz SF, Foster JK Jr (1971) Roentgenographic interpretation of experimentally produced bony lesions. I. Oral Surg Oral Med Oral Pathol 32:606–612
Shaffer MD, Juruaz DA, Haggerty PC (1998) The effect of periradicular endodontic pathosis on the apical region of adjacent implants. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 86:578–581
Tammisalo T, Luostarinen T, Vahatalo K, Tammisalo EH (1993) Comparison of periapical and detailed narrow-beam radiography for diagnosis of periapical bone lesions. Dentomaxillofac Radiol 22:183–187
van Steenberghe D, Naert I (1998) The first two-stage dental implant system and its clinical application. Periodontol 2000 17:89–95
Velvart P, Hecker H, Tillinger G (2001) Detection of the apical lesion and the mandibular canal in conventional radiography and computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 92:682–688
Wenzel A (1988) Effect of image enhancement for detectability of bone lesions in digitized intraoral radiographs. Scand J Dent Res 96:149–160
Yokota ET, Miles DA, Newton CW, Brown CE Jr (1994) Interpretation of periapical lesions using RadioVisioGraphy. J Endod 20:490–494
Acknowledgements
The authors wish to thank Dr. Susanne Mortensen and Dr. Moe Rezai Kallaj for recording the intraoral radiographs and for their participation as examiners in the present study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Stavropoulos, A., Wenzel, A. Accuracy of cone beam dental CT, intraoral digital and conventional film radiography for the detection of periapical lesions. An ex vivo study in pig jaws. Clin Oral Invest 11, 101–106 (2007). https://doi.org/10.1007/s00784-006-0078-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-006-0078-8