
Abstract
Central nervous system infection (CNSI) results in significant health and economic burdens worldwide, but the diversity of causative pathogens makes differential diagnosis very difficult. Although PCR and real-time fluorescent quantitative PCR (q-PCR) assays are widely applied for pathogen detection, they are generally optimized for the detection of a single or limited number of targets and are not suitable for the diagnosis of numerous CNSI agents. In this study, we describe the development of a resequencing pathogen microarray (RPM-IVDC4) method for the simultaneous detection of viruses, bacteria, fungi and parasites that cause CNSI. The test panel of this assay included more than 100 microorganism species across 45 genera and 30 families. The analytical specificity and sensitivity were examined using a panel of positive reference strains, and the clinical performance was evaluated using 432 clinical samples by comparing the results with q-PCR assays. Our results demonstrated good performance of the RPM-IVDC4 assay in terms of sensitivity, specificity and detection range, suggesting that the platform can be further developed for high-throughput CNSI diagnosis.
Similar content being viewed by others

Introduction
Central nervous system infection (CNSI) results in significant health and economic burdens worldwide, but the diversity of pathogens makes differential diagnosis very difficult. Encephalitis and meningitis are serious diseases of the CNS, however, their etiology remains unknown in most cases [1]. More than 100 infectious causes have been described, but it is difficult to provide a consensual clinical or biological definition of their syndromes, and it is even more difficult to relate encephalitis and meningitis to a specific agent [2, 3].
CNSI agents can be found across viral, bacterial, fungal and parasitic taxonomic groups. The clear majority of aseptic meningitis cases are caused by enterovirus (EV) species that mostly target children [4]. In developed countries, the most common and important cause of viral encephalitis is human herpesviruses (HHV), including herpes simplex viruses (HSV-1, HSV-2), varicella-zoster virus (VZV), Epstein-Barr virus (EBV), cytomegalovirus (CMV) and human herpes virus 6 (HHV6). Most cases (>85%) are due to HSV-1 [2, 5]. Japanese encephalitis virus (JEV) is more likely to cause encephalitis in children than in adults, whereas the elderly are more susceptible to West Nile virus (WNV) infection. Subacute sclerosingpanencephalitis results from persistent measles virus (MeV) infection, and progressive panencephalitis may occur many years after congenital or perinatal rubella virus (RuV) infection [6, 7]. Neisseria meningitidis, Haemophilusinfluenzae and Streptococcus pneumoniae are the leading causes of bacterial meningitis [8, 9]. Many other microorganisms, including fungi and parasites, are related to CNSI, but are far less common.
Traditional methods for identification of CNSI agents are based on culture, and although reliable and familiar, have a series of drawbacks. Pathogen culture can be time consuming and a significant proportion of microorganisms are not amenable to culture. Moreover, facilities are needed to assure safety and containment of the high-risk agents. Molecular methods such as PCR and real-time fluorescent quantitative PCR (q-PCR) may provide rapid identification based on nucleic acid amplification techniques (NAAT). Compared with culture-based assays, NAAT are more rapid, sensitive and appropriate for the identification of non-culturable pathogen serotypes [5]. However, most PCR/q-PCR methods in use are optimized for the detection of a single or a limited number of targets. Although sensitive and specific, they are not appropriate for the detection of multiple and varied pathogens. As CNSI agents are numerous, it is therefore highly desirable to develop a method that achieves simultaneous detection of multiple agents that cause similar clinical syndromes and/or share similar epidemiological features of encephalitis and meningitis.
The resequencing pathogen microarray (RPM) is a promising technology that allows simultaneous detection of many infectious agents. Thousands of synthesized oligonucleotide probes are covalently fixated on glass- or silicon-based high-density microarrays. The nucleic acid is amplified using specific PCR, followed by purification, fragmentation and labelling. The labeled sample is then injected into the RPM and hybridized overnight in the hybridization oven. Short fluorophore labeled DNA fragments (20–200 bp), which are derived from the samples, hybridize to these probes. After washing and staining on the fluidics station, the microarrays are scanned to calculate the C3 fluorescence signal value, then pathogen-specific sequence information is produced as FASTA-format output files [10, 11]. The sequence information produced by RPM allows high-resolution pathogen identification and near-neighbor discrimination, which makes RPM suitable for outbreak investigations caused by atypical or uncommon pathogens. Several RPM assays have been developed as diagnostic platforms to effectively and simultaneously detect large numbers of diverse clinical or environmental pathogens [11,12,13,14,15,16,17,18], but no RPM assay has been reported for the identification of CNSI pathogens.
In this study, we describe the development of an RPM method (RPM-IVDC4) for the simultaneous detection of CNSI agents, including viruses, bacteria, fungi and parasites. The detection panel of RPM-IVDC4 listed in Table 1 consists of more than 100 microorganism species from 45 genera and 30 families. The analytical specificity and sensitivity were examined and the clinical performance of the RPM-IVDC4 assay was evaluated by comparing the results with related q-PCR assays.
Material and methods
Samples
Between January and December 2015, 432 clinical cerebrospinal fluid (CSF) samples were collected from patients who were diagnosed with acute viral meningitis or encephalitis based on clinical symptoms. The clinical diagnosis and CSF sampling were conducted by the Beijing Children’s Hospital, Children’s Hospital of Hebei Province, No. 1 Hospital of Shijiazhuang, and The Second Hospital of Hebei Medical University. All aspects of the study were performed in accordance with national ethics regulations and approved by the Institutional Review Boards of the Chinese Center for Disease Control and Prevention (China CDC) and each hospital. Patients or children’s parents were apprised of the study’s purpose and of their right to keep information confidential. Written consent was obtained from patients or children’s parents.
Nucleic acid extraction
Total nucleic acids were extracted from 150 μL of CSF using the MasterPure Complete DNA and RNA purification kit (Epicenter Technologies, Madison, WI) according to the manufacturer’s instructions. Purified DNA and RNA were stored at −80 °C.
Primer design and internal control
In total, 214 pairs of gene-specific primers were designed for the RPM-IVDC4 by the Institute of Viral Disease Control and Prevention (IVDC) and TessArae LLC. The detailed sequence information of primers and probes are presented in the supplementary material. For each pathogen, primers and probes were designed according to criteria described previously [19]. In brief, the uniqueness of primers was checked using a full search of the GenBank database with the BLAST program. To minimize the possibility of primer dimerization and to help ensure sufficient amplification, six independent multiplex primer cocktails/pools were developed for amplification of targeted sequences represented in the RPM-IVDC4 microarray. Of the six multiplex primer cocktails, which are shown in Figure 1, Mix I was dedicated primarily to bunyaviruses, paramyxoviruses and rhabdoviruses; Mix II to flaviviruses; Mix III to picornaviruses and retroviruses; Mix IV to arenaviruses, togaviruses, retroviruses and herpesviruses; Mix V to bacteria; and Mix VI to fungi and parasites. The strategy of temperature switch PCR (TSP) [20] was applied in this RPM assay and one pair of universal primers was adapted from our previous studies [14, 21]. The chimeric primers consisted of a gene-specific sequence fused at the 5ʹ-end to the universal tag sequence, thus, all the chimeric primers had similar annealing temperatures to assure the same approximate amplification efficiency. Two Arabidopsis thaliana genes, NAC1 and TIM, were selected as internal negative controls, as these plant genes would be unlikely to occur naturally in clinical samples [22].

The RPM-IVDC4 work flow. Total nucleic acids were extracted from 150 μL of CSF samples and the RNA transcribed to cDNA. Six independent primer cocktails/pools were used in multiplex PCRs, and the products were pooled together and subjected to purification. Purified PCR products were fragmented for 5 min and then labeled for 30 min. Microarray hybridization and processing was carried out at 49 °C according to the manufacturer’s recommended protocol. The raw image files obtained from scanning of the microarrays were converted into FASTA files using TessArray Sequence Analysis (TSEQ) software. The data were analyzed using a bioinformatics cloud server and the final diagnostic reports were sent back to the RPM operator
Reverse transcription and multiplex PCR
A reverse transcription using SuperScript III (Invitrogen LifeTechnologies, Carlsbad, CA) was performed using random hexamers in a total volume of 20 μL before six targeted multiplex PCR assays (Primer Mixes I to VI). Each multiple PCR amplification was performed using 2.5 μL of cDNA solution, 1.5 μL of 10× primer mixture, and 7.5 μL of 2× Multiplex Master Mix (Qiagen, Hilden, Germany) in a total volume of 15 μL. The amplification protocol was: initial denaturation at 94 °C for 15 min, 10 cycles of 95 °C for 30 s, 56 °C for 30 s, and 72 °C for 60 s; 10 cycles of 95 °C for 30 s, 68 °C for 30 s, and 72 °C for 60 s; 20 cycles of 95 °C for 30 s, 50 °C for 30 s, and 72 °C for 60 s; and a final incubation at 72 °C for 3 min. The thermal cycling was performed using a PCR Amplifier (Thermo Electron Corp, Vantaa, Finland).
RPM-IVDC4 processing
The products from the six multiplex PCR tubes were pooled together and subjected to purification (Qiagen). Purified PCR products were fragmented for 5 min and then labeled for 30 min. Microarray hybridization and processing were carried out at 49 °C according to the manufacturer’s recommended protocol (Affymetrix Inc., Santa Clara, CA) using a GeneChip resequencing assay kit (Affymetrix Inc.). The raw image files obtained from scanning of the microarrays were converted into FASTA files using TessArray Sequence Analysis (TSEQ) software. A FASTA output file was subjected to alignment with corresponding detector tile sequences, which are prototype sequences that represent portions of the genomic DNA/RNA of a targeted organism. The quality of the sequence was evaluated by the “C3 Score”, which is the total number of TSEQ-identified nucleotides that appear in runs of three or more consecutive (non-N) base calls, expressed as a percentage of the length (nucleotides) of each RPM-IVDC4 detector tile sequence [23, 24]. The data were analyzed using a bioinformatics cloud server and the final diagnostic reports were sent back to the RPM operator.
Analytical specificity and sensitivity
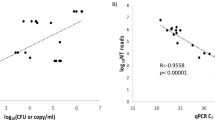
The primer specificity of RPM was tested with 40 previously confirmed positive CNSI samples, among which 33 were viral-positive and 7 were bacterial-positive. For the remaining pathogens (for which positive samples were unavailable), we artificially synthesized the target DNA from their genome sequence. Thus, all the primers and probes of the RPM were tested. A subset of 14 samples from these 40 positive samples was selected to evaluate the limit of detection (LOD) of the RPM assay. The quantitative recombinant plasmids (for DNA viruses and bacteria) or in vitro transcribed RNA (for RNA viruses) were prepared as we have previously described [25]. Ten-fold serial dilutions of these RNA/DNA templates with known copy numbers (20 to 200,000 copies/μL) were used to evaluate the LOD of the RPM assay.
Clinical evaluation
A total of 432 samples were tested simultaneously by RPM assay and q-PCR. The primers and probes were adopted from reported q-PCR methods for the detection of EV [26], HSV 1 and 2, VZV, EBV, CMV and HHV 6 [27]. All statistical analyses were performed using Statistical Package for Social Sciences software. The 2 test and McNemar’s test were conducted to measure the sensitivity, specificity, and the detection agreement of the RPM and q-PCR assays.
Results
The RPM assay could discriminate and identify all the reference strains listed in Table 2 except for rhinovirus (RV). All the artificially synthesized DNAs, which represented unavailable positive samples, were mixed together and tested using the RPM; no cross-reaction was observed. The analytical sensitivity of the RPM assay was evaluated using serial 10-fold dilutions of in vitro transcribed RNA or DNA clones. The LOD ranged from 20 to 200 copies/reaction for mono-sample, and 20 to 2000 copies/reaction for mixed-samples (Table 2).
Results were obtained for 432 clinical CSF samples (Figure 2), with positive results determined in 118 cases (27.31%) using the RPM, including 93 positive for EV (80.87% of positives; 21.53% of the total); 10 for JEV (8.47% and 2.31%); 2 for HSV-1 (1.69% and 0.46%); 2 for CMV (1.69% and 0.46%); 2 for HHV-6 (1.69% and 0.46%); 1 for EBV (0.85% and 0.23%); and 1 for MuV (0.85% and 0.23%). There were mixed infections in seven cases (5.93% and 1.62%), including 5 EV and JEV, and 2 EV and EBV. Thus, among mixed infections, 7 EV, 5 JEV, and 2 EBV infections were identified. No cases were found for HIV, MeV, TBEV, RuV, WNV, JCV, HSV2, VZV or AdV infections.

The distribution of viruses among the 432 clinical samples tested using the RPM-IVDC4 assay. Results were obtained for 432 clinical CSF samples, with positive results determined in 118 cases using the RPM (27.31%), including 93 positive for EV (80.87% of positives; 21.53% of the total); 10 for JEV (8.47% and 2.31%); 2 for HSV-1 (1.69% and 0.46%); 2 for CMV (1.69% and 0.46%); 2 for HHV-6 (1.69% and 0.46%); 1 for EBV (0.85% and 0.23%); and 1 for MuV (0.85% and 0.23%). There were mixed infections in seven cases (5.93% and 1.62%): 5 EV and JEV, and 2 EV and EBV. Thus, among mixed infections, 7 EV, 5 JEV, and 2 EBV infections were identified
For HSV1, HSV2, VZV and CMV, the detection results by RPM-IVDC4 coincided with those obtained from the parallel q-PCR assays. For EV, EBV and HHV6, the RPM detection sensitivity was 100% and the RPM assay detected five more cases of EV infection, one more of EBV, and one more of HHV6 than by q-PCR (Table 3). In addition, the RPM assay detected 15 cases of JEV infection and one of MuV infection, which were not included in the q-PCR panel. For the aforementioned 23 cases not detected by q-PCR, true positives were confirmed by monoplex PCR followed by Sanger sequencing.
Discussion
The RPM platform has proven successful for the identification and characterization of numerous clinical pathogens including avian influenza, rhinoviruses, enteroviruses, and arboviral virus, as well as pathogens in environmental samples [12, 13, 22, 23]. In this study, we developed and evaluated RPM-IVDC4 for the identification of viral, bacterial, fungal and parasite pathogens known to cause, or to be related to, CNSI.
This study demonstrates that the RPM-IVDC4 platform can achieve highly-sensitive and specific detection of multiple CNS disease agents in a single test. A properly designed multiplex PCR strategy is essential to improve the performance of the RPM because the hybridization process is already standardized. The specificity test using 40 known positive samples demonstrated the capability of the RPM-IVDC4 to discriminate among different CNSI pathogens. As the primers and tiles for EV were designed according to the 5ʹ-untranslated region (UTR), the RPM could not discriminate RV from EV, which is the same situation as with the q-PCR assay. In our study, the use of TSP technology maintained target enrichment and mitigated amplification bias among different primer pairs. LOD experiments showed that the RPM-IVDC4 could detect as little as 20 copies/reaction of targeted genes, which is comparable to other reported methods and meets diagnostic requirements [14, 21].
As we described above, the RPM- IVDC4 was designed to detect a broad range of pathogens (Table 1) in a single specimen. Thus, in addition to the common CNSI agents, this method also allows the detection of low-prevalence or emerging infectious agents. For example, arenaviruses, bunyaviruses, Anaplasmataceae, Mycoplasma and Rickettsia, not commonly present in CSF or universally distributed, were included in the RPM-IVDC4 panel. In addition, the RPM-IVDC4 was designed to amplify several different gene targets from one microorganism to improve detection rates. With multiple primer pairs and tiles per pathogen, the sequences of two or more separate regions of one pathogen were amplified and hybridized. For example, the 3ʹ-UTR and NS5 regions were detected simultaneously using specific primers for the identification of WNV; as many as nine gene targets, including aroE, gyrB, mecA, luk-PV, e-toxA, e-toxB, e-toxC, alpha-tox and TS-tox, were tiled on the microarray to detect and identify Staphylococcus aureus.
Compared to q-PCR or other conventional methods, the main advantage of RPM- IVDC4 is the enablement of more comprehensive detection of CNSI pathogens. As shown in the Table 1, almost all common CNSI pathogens were included in the test menu of RPM-IVDC4, and some atypical/uncommon CNSI pathogens could also be detected by this method. By amplifying highly-conserved sequences using multiple primers, a greater number of positive cases could be detected with RPM than by q-PCR. For example, as variation in the 5ʹ-UTR is sufficient to allow accurate identification of groupings of EV [22], we designed 19 primer pairs specific to this region. As shown in Table 3, the RPM reported five more EV-positive cases than the equivalent q-PCR assay. Although both methods targeted the 5ʹ-UTR for EV detection, the 19 sets of primer pairs and probes in the RPM undoubtedly provided a greater probability of oligonucleotide matching than the one set (as is used in the reference q-PCR), resulting in higher clinical sensitivity for the RPM. Similarly, one more EBV, and one more HHV6, mistakenly defined as cases with unclear etiology by q-PCR, could be successfully identified by RPM. Thus, we conclude that the RPM array maximizes the likelihood of hybridization of primers to conserved regions within a given viral genus/family, demonstrating an effective strategy for detecting highly-variable or uncharacterized viruses.
In addition to the multiplicity, the RPM-IVDC4 generates sequence information concerning pathogen variation and achieves greater discrimination among subtypes, while none of the available commercial assays provide pathogen-specific sequence information [11]. This characteristic not only makes RPM a powerful identification tool, but also allows pathogens to be phylogenetically categorized based on their genetic variation in the same assay [28, 29].
Our laboratory has established several microorganism identification methods using Roche 454, Illumina or Ion torrent platforms [30,31,32]. Having compared the throughput, multiplicity, complexity, time-cost, reagent-cost and labor-cost of RPM and next-generation sequencing (NGS) to perform similar clinical studies, we found that the RPM is more convenient and sufficient to meet the needs of pathogen identification. Although the library construction and sequencing process of NGS are becoming easier as reagent kits are now commercially available, the bioinformatics analysis remains a complex and time-consuming hurdle that requires a high level of expertise. In contrast, the primers and probes for RPM are predetermined, relating to critical regions of sequence of the targeted pathogens, and thus require very little bioinformatics expertise among the operators [11].
Of the 432 clinical samples tested in the present study, positive samples accounted for 27.31% (118/432). No pathogen was detected in 314 (72.69%) samples, indicating testing the CSF alone is not sensitive enough for CNSI diagnosis. To maximize the detection rate of CNSI agents, we recommend that both NAAT and antibody studies are used together. CSF testing generally allows a definitive result, but testing of other sample types such as blood, throat swabs, feces and skin biopsies may also provide additional diagnostic information. The causative agent in ‘test-negative’ clinical samples might represent a known or variant microorganism, previously not associated with CNSI, or indeed a completely unknown pathogen. Failure in detection might also be attributable to the limited sensitivity and specificity of currently used methods or suboptimal sample collection time. As is the case with other PCR-based methods, the disadvantage of RPM is the pre-requirement for knowledge of the microorganism’s genome sequences. To overcome the disadvantages of RPM, NGS could be used to identify potential causative agents in test-negative samples, as unbiased sequencing enables identification of all pathogens in a single run.
The current RPM-IVDC4 assay showed good performance in terms of sensitivity, specificity and detection range, suggesting that the platform can be developed further for high-throughput CNSI diagnosis. However, automation must be considered to optimize the RPM design or process. In its current format, the RPM-IVDC4 assay for 24 samples can be finished within 12 h with a combination of manual and automated processes. To decrease the assay time and reduce ‘hands-on’ user error, the RPM should be adapted for full-automation. The difficulty lies in the trade-off between automation and the risk of nucleic acid contamination.
References
Dupuis M, Hull R, Wang H, Nattanmai S, Glasheen B, Fusco H, Dzigua L, Markey K, Tavakoli NP (2011) Molecular detection of viral causes of encephalitis and meningitis in New York State. J Med Virol 83(12):2172–2181. doi:10.1002/jmv.22169
Stahl JP, Mailles A, Dacheux L, Morand P (2011) Epidemiology of viral encephalitis in 2011. Med Mal Infect 41(9):453–464. doi:10.1016/j.medmal.2011.05.015
Whitley RJ, Gnann JW (2002) Viral encephalitis: familiar infections and emerging pathogens. Lancet 359(9305):507–513. doi:10.1016/S0140-6736(02)07681-X
Michos AG, Syriopoulou VP, Hadjichristodoulou C, Daikos GL, Lagona E, Douridas P, Mostrou G, Theodoridou M (2007) Aseptic meningitis in children: analysis of 506 cases. PloS One 2(7):e674. doi:10.1371/journal.pone.0000674
Rice P (2009) Viral meningitis and encephalitis. Medicine 37(11):574–578
Schonberger K, Ludwig MS, Wildner M, Weissbrich B (2013) Epidemiology of subacute sclerosing panencephalitis (SSPE) in Germany from 2003 to 2009: a risk estimation. PloS One 8(7):e68909. doi:10.1371/journal.pone.0068909
Mutton K, Guiver M (2011) Laboratory techniques for human viral encephalitis diagnosis. Infect Disord Drug Targets 11(3):206–234
Vuong J, Collard JM, Whaley MJ, Bassira I, Seidou I, Diarra S, Ouedraogo RT, Kambire D, Taylor TH Jr, Sacchi C, Mayer LW, Wang X (2016) Development of real-time PCR methods for the detection of bacterial meningitis pathogens without DNA extraction. PloS One 11(2):e0147765. doi:10.1371/journal.pone.0147765
Gasparini R, Panatto D, Bragazzi NL, Lai PL, Bechini A, Levi M, Durando P, Amicizia D (2015) How the knowledge of interactions between meningococcus and the human immune system has been used to prepare effective Neisseria meningitidis vaccines. J Immunol Res 2015:189153. doi:10.1155/2015/189153
Donatin E, Drancourt M (2012) DNA microarrays for the diagnosis of infectious diseases. Med Mal Infect 42(10):453–459. doi:10.1016/j.medmal.2012.07.017
Kourout M, Fisher C, Purkayastha A, Tibbetts C, Winkelman V, Williamson P, Nakhasi HL, Duncan R (2016) Multiplex detection and identification of viral, bacterial, and protozoan pathogens in human blood and plasma using a high-density resequencing pathogen microarray platform. Transfusion 56(6 Pt 2):1537–1547. doi:10.1111/trf.13524
Leski TA, Malanoski AP, Gregory MJ, Lin B, Stenger DA (2011) Application of a broad-range resequencing array for detection of pathogens in desert dust samples from Kuwait and Iraq. Appl Environ Microbiol 77(13):4285–4292. doi:10.1128/AEM.00021-11
Berthet N, Paulous S, Coffey LL, Frenkiel MP, Moltini I, Tran C, Matheus S, Ottone C, Ungeheuer MN, Renaudat C, Caro V, Dussart P, Gessain A, Despres P (2013) Resequencing microarray method for molecular diagnosis of human arboviral diseases. J Clin Virol 56(3):238–243. doi:10.1016/j.jcv.2012.10.022
Shen H, Zhu B, Wang S, Mo H, Wang J, Li J, Zhang C, Zeng H, Guan L, Shi W, Zhang Y, Ma X (2015) Association of targeted multiplex PCR with resequencing microarray for the detection of multiple respiratory pathogens. Front Microbiol 6:532. doi:10.3389/fmicb.2015.00532
Dacheux L, Berthet N, Dissard G, Holmes EC, Delmas O, Larrous F, Guigon G, Dickinson P, Faye O, Sall AA, Old IG, Kong K, Kennedy GC, Manuguerra JC, Cole ST, Caro V, Gessain A, Bourhy H (2010) Application of broad-spectrum resequencing microarray for genotyping rhabdoviruses. J Virol 84(18):9557–9574. doi:10.1128/JVI.00771-10
Woo PC, Lau SK, Choi GK, Fung HT, Shek KC, Miao J, Chan BY, Ng KH, Ngan AH, Ellis-Behnke R, Que TL, Kam CW, Yuen KY (2010) Resequencing microarray for detection of human adenoviruses in patients with conjunctivitis. J Clin Virol 47(3):282–285. doi:10.1016/j.jcv.2009.12.014
Berthet N, Dickinson P, Filliol I, Reinhardt AK, Batejat C, Vallaeys T, Kong KA, Davies C, Lee W, Zhang S, Turpaz Y, Heym B, Coralie G, Dacheux L, Burguiere AM, Bourhy H, Old IG, Manuguerra JC, Cole ST, Kennedy GC (2008) Massively parallel pathogen identification using high-density microarrays. Microb Biotechnol 1(1):79–86. doi:10.1111/j.1751-7915.2007.00012.x
Leski TA, Ansumana R, Malanoski AP, Jimmy DH, Bangura U, Barrows BR, Alpha M, Koroma BM, Long NC, Sundufu AJ, Bockarie AS, Lin B, Stenger DA (2012) Leapfrog diagnostics: demonstration of a broad spectrum pathogen identification platform in a resource-limited setting. Health Res Policy Syst 10:22. doi:10.1186/1478-4505-10-22
Lin B, Blaney KM, Malanoski AP, Ligler AG, Schnur JM, Metzgar D, Russell KL, Stenger DA (2007) Using a resequencing microarray as a multiple respiratory pathogen detection assay. J Clin Microbiol 45(2):443–452. doi:10.1128/JCM.01870-06
Tabone T, Mather DE, Hayden MJ (2009) Temperature switch PCR (TSP): robust assay design for reliable amplification and genotyping of SNPs. BMC Genom 10:580. doi:10.1186/1471-2164-10-580
Shen H, Shi W, Wang J, Wang M, Li J, Zhang C, Nie K, Yang M, Zhang Y, Li A, Tan W, Ma X (2013) Development of a new resequencing pathogen microarray based assay for detection of broad-spectrum respiratory tract viruses in patients with community-acquired pneumonia. PloS One 8(9):e75704. doi:10.1371/journal.pone.0075704
Wang Z, Malanoski AP, Lin B, Kidd C, Long NC, Blaney KM, Thach DC, Tibbetts C, Stenger DA (2008) Resequencing microarray probe design for typing genetically diverse viruses: human rhinoviruses and enteroviruses. BMC Genom 9:577. doi:10.1186/1471-2164-9-577
Lin B, Malanoski AP, Wang Z, Blaney KM, Long NC, Meador CE, Metzgar D, Myers CA, Yingst SL, Monteville MR, Saad MD, Schnur JM, Tibbetts C, Stenger DA (2009) Universal detection and identification of avian influenza virus by use of resequencing microarrays. J Clin Microbiol 47(4):988–993. doi:10.1128/JCM.01346-08
Malanoski AP, Lin B, Stenger DA (2008) A model of base-call resolution on broad-spectrum pathogen detection resequencing DNA microarrays. Nucleic Acids Res 36(10):3194–3201. doi:10.1093/nar/gkm1156
Wang J, Xu Z, Niu P, Zhang C, Zhang J, Guan L, Kan B, Duan Z, Ma X (2014) A two-tube multiplex reverse transcription PCR assay for simultaneous detection of viral and bacterial pathogens of infectious diarrhea. BioMed Res Int 2014:648520. doi:10.1155/2014/648520
Cabrerizo M, Calvo C, Rabella N, Munoz-Almagro C, del Amo E, Perez-Ruiz M, Sanbonmatsu-Gamez S, Moreno-Docon A, Otero A, Trallero G (2014) Design and validation of a real-time RT-PCR for the simultaneous detection of enteroviruses and parechoviruses in clinical samples. J Virol Methods 208:125–128. doi:10.1016/j.jviromet.2014.08.008
Sugita S, Shimizu N, Watanabe K, Mizukami M, Morio T, Sugamoto Y, Mochizuki M (2008) Use of multiplex PCR and real-time PCR to detect human herpes virus genome in ocular fluids of patients with uveitis. Br J Ophthalmol 92(7):928–932. doi:10.1136/bjo.2007.133967
Lin B, Wang Z, Vora GJ, Thornton JA, Schnur JM, Thach DC, Blaney KM, Ligler AG, Malanoski AP, Santiago J, Walter EA, Agan BK, Metzgar D, Seto D, Daum LT, Kruzelock R, Rowley RK, Hanson EH, Tibbetts C, Stenger DA (2006) Broad-spectrum respiratory tract pathogen identification using resequencing DNA microarrays. Genome Res 16(4):527–535. doi:10.1101/gr.4337206
Wang Z, Daum LT, Vora GJ, Metzgar D, Walter EA, Canas LC, Malanoski AP, Lin B, Stenger DA (2006) Identifying influenza viruses with resequencing microarrays. Emerg Infect Dis 12(4):638–646. doi:10.3201/eid1204.051441
Li Y, Wang H, Nie K, Zhang C, Zhang Y, Wang J, Niu P, Ma X (2016) VIP: an integrated pipeline for metagenomics of virus identification and discovery. Sci Rep 6:23774. doi:10.1038/srep23774
Liu L, Wu W, Zhao X, Xiong Y, Zhang S, Liu X, Qu J, Li J, Nei K, Liang M, Shu Y, Hu G, Ma X, Li D (2016) Complete genome sequence of Zika virus from the first imported case in mainland China. Genome Announc. doi:10.1128/genomeA.00291-16
Lu R, Wang Y, Wang W, Nie K, Zhao Y, Su J, Deng Y, Zhou W, Li Y, Wang H, Ke C, Ma X, Wu G, Tan W (2015) Complete genome sequence of middle east respiratory syndrome coronavirus (MERS-CoV) from the first imported MERS-CoV case in China. Genome Announc. doi:10.1128/genomeA.00818-15
Author information
Authors and Affiliations
Contributions
Xuejun Ma, Suzhen Sun and Ji Wang designed the study; Ji Wang, Panhui Yu and Tengfei Yan performed the RPM experiments; Chen Chen and Xinxin Shen prepared the samples and the labware; Xiangpeng Chen and ZhengdeXie analyzed the data; Lixin Li, Xiuxia Wang, ZhengdeXie and Suzhen Sun collected the samples and performed q-PCR. Ji Wang wrote the manuscript. The first three authors in the author list contributed equally to this research.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
This work was supported by the National Key Research and Development Plan (2016TFC1202700, 2016YFC120090), Beijing Municipal Science and Technology Commission Project (D151100002115003), the Capital Clinical Feature Project of Beijing Technology Program (Z151100004015046), and Guangzhou Municipal Science and Technology Commission Project (2015B2150820).
Additional information
Handling Editor: Martin Schwemmle.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Wang, J., Yu, P., Xie, Z. et al. A resequencing pathogen microarray method for high-throughput molecular diagnosis of multiple etiologies associated with central nervous system infection. Arch Virol 162, 3769–3778 (2017). https://doi.org/10.1007/s00705-017-3550-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00705-017-3550-7