
Abstract
Dengue virus (DENV) causes a life-threatening illness, with a wide range of symptoms from mild febrile illness, dengue fever (DF), to life-threatening illness, dengue hemorrhagic fever (DHF). Antibody-dependent enhancement (ADE) is considered to be a risk factor for DHF. In the present study, we determined the parameters for ADE assays using FcγR-expressing BHK cells. Monoclonal antibodies and human serum samples were used in the assays. We examined antibody concentration and virus concentration and analyzed whether antibody concentration or DENV-antibody ratio determines ADE activity. Virus growth was quantified by a conventional plaque titration method using FcγR-expressing BHK cells. The assay allowed the detection of DENV growth with inoculation doses ranging from 102 PFU/ml to 106 PFU/ml using monoclonal antibodies and undiluted or diluted serum samples. The results indicate that antibody concentration rather than DENV-antibody ratio determines the demonstration of ADE activity. Thus, antibody concentration rather than multiplicity of infection was defined as the main determinant in ADE assays using FcγR-expressing BHK cells.
Similar content being viewed by others


Introduction
Antibody-dependent enhancement (ADE) of virus infection has been reported for various viruses [1–6], and it has been suggested that ADE may contribute to disease severity in DENV infection [7–12]. In particular, the possibility that dengue-vaccine-induced ADE might potentially increase the risk of severe dengue illness has been a concern in vaccine development [13–15]. It is therefore necessary to develop assays and methodologies to investigate the infection-enhancing activity of antibodies induced by natural infection and vaccination.
Fc gamma receptor (FcγR)-expressing cell lines have proved useful in ADE studies in vitro [16–20]. Additionally, human peripheral blood mononuclear cells (PBMCs) have been used in the determination of ADE activity using undiluted serum samples [21]. The use of primary human monocytes has been limited because of their lesser convenience for use and limited availability compared to established cell lines [22], in addition to poor viral replication at low passages and high experimental variation [23]. Cell lines, including a human acute monocytic leukemia cell line (THP1), a human myelogenous cell line (K562), and a mouse macrophage cell line (PD3881), have also been used in studies of ADE activity using human serum samples [17, 24–28]. Although assay reproducibility has been reported previously in ADE patterns using established cell lines, the amount of infectious virus required to infect the FcγR-expressing hematopoietic cell lines varied among DENV isolates [28]. Furthermore, hematopoietic cell lines are naturally non-adherent, and thus titration of infectious virus particles requires surrogate plaque titration assays.
We have previously developed an antibody-dependent enhancement assay for DENV using BHK cells that stably expresses human FcγR [29]. ADE activity was constantly detected in DENV-antibody-positive human serum samples by using the FcγR-expressing cells. In this paper, we report the parameters that influence ADE activity levels using monoclonal antibodies and serum samples from dengue patients in the early and late phases of the disease.
Materials and methods
Virus
Dengue virus (DENV) strain DENV-2 (D2/Hu/OPD030NIID/2005, GenBank accession no. AB219135) was used in all infection assays. The DENV-2 strain was isolated from a patient in East Timor and belonged to the genotype 2 group [30].
Cell lines
BHK-21, a hamster kidney cell line (Japan Health Science Research Resources Bank), was cultured in Eagle’s minimum essential medium (EMEM; Sigma, St. Louis, MO, USA) supplemented with 10 % heat-inactivated FBS (Sigma) without antibiotics at 37 °C in 5 % CO2. FcγR-expressing BHK cell lines [29] were cultured in EMEM supplemented with 10 % heat-inactivated FBS and 0.5 mg/ml neomycin (PAA Laboratories GmbH, Austria)
Monoclonal antibodies and human serum samples
Flavivirus cross-reactive mouse monoclonal IgG antibodies (mAb) used in this study were 6B6C (5.9 mg/ml), 4G2 (2.6 mg/ml, ATCC MAb HB-112 D1-4G2-4-15), and 3H12 (1.6 mg/ml) [31–33].
Four serum samples were obtained from two patients (two samples each) with secondary DENV-2 infection. Serum samples from patient 1 were obtained at day 3 (serum sample 1a) and day 12 (serum sample 1b) after onset of disease. Serum samples from patient 2 were obtained at day 3 (serum sample 2a) and day 6 (serum sample 2b) after the onset of disease. Sample 1a was negative for anti-DENV IgM (Focus Diagnostics, Cypress, CA, USA) and positive for anti-DENV IgG (PanBio, Australia). The serum samples were examined for the presence of DENV viral RNA (vRNA) by RT-PCR, and anti-DENV IgM and IgG by enzyme-linked immunosorbent assay [34–36]. Serum samples 1b, 2a, and 2b were positive for anti-DENV IgM and IgG. The presence of secondary flavivirus infection was defined by a DENV IgM/IgG ratio of <1.2 [37]. Serum samples used in the experiments were heat-inactivated at 56 °C for 30 minutes.
Preparation of virus-antibody immune complex
Heat-inactivated undiluted serum samples were prepared with EMEM supplemented with 10 % FBS and serially diluted tenfold from 1:101 to 1:104. Twenty-five microliters of DENV at concentrations of 1 × 106 PFU/ml, 1 × 105 PFU/ml, 1 × 104 PFU/ml, 1 × 103 PFU/ml, and 1 × 102 PFU/ml was added to 25 μl of serially diluted serum samples. For infection in the absence of patient serum, 25 μl of virus suspension was added to 25 μl of 10 % FBS EMEM. The diluent for these assays consisted of EMEM supplemented with 10 % FBS. The virus-antibody mixture was incubated at 37 °C for 1 hour.
Infection assay
After incubation, virus mixtures were serially diluted tenfold and 50 μl of the serially diluted virus-antibody mixtures was added to the FcγR-expressing BHK cells and FcγR-negative BHK cells in 12-well plates. The plates were incubated for 60 minutes at 37 °C in 5 % CO2. One milliliter of maintenance medium consisting of 2 % FBS/ MEM and 1 % methylcellulose was added to the cells after virus absorption. The plates were incubated at 37 °C in 5 % CO2 for 5 days. After 5 days of incubation, cells were fixed with 5 % paraformaldehyde for 60 minutes at room temperature and washed with water. Methylene blue was used for staining, and plaques were counted. Viral titers were expressed as plaque-forming units per milliliter (p.f.u./ml) and were determined by the following formula: (mean number of plaques per well) × (dilution) / (inoculum volume). The fold enhancement values were determined by the following formula: (mean number of plaques in the presence of antibodies or serum sample) / mean number of plaques in the absence of antibodies or serum sample). The mean plus two standard deviations (SD) of the negative control was used as a cutoff to differentiate enhancing and non-enhancing activity [21, 38]. Each sample was tested in duplicate assays.
Results
Detection of DENV-2 infection-enhancement activity of monoclonal antibodies 6B6C, 4G2 and 3H12
Three DENV-reactive antibodies, 6B6C, 4G2 and 3H12, were tested for their capacity to enhance DENV-2 infection. ADE activity was detected for the three antibodies, when FcγR-expressing BHK cells were used, but not when FcγR-negative BHK cells were used (Tables 1, 2, 3). ADE activity was examined by adding undiluted and 1:10 serially diluted monoclonal antibodies to each of the virus titers (1 × 106 to 1 × 102 PFU/ml). We analyzed whether ADE activity was determined by the concentration of monoclonal antibodies or by the ratio of challenge DENV titer to antibody. ADE activity was constantly detected at defined dilutions of monoclonal antibodies, irrespective of the challenge DENV titers: mAb 6B6C at 1:103–1:104, 4G2 at 1:103–1:104, and 3H12 at 1:103-1:104 (Tables 1, 2, 3, Fig. 1). The results indicate that antibody concentration, rather than DENV-antibody ratio, determines the presentation of ADE activity.

Enhancement of DENV-2 infection by monoclonal antibodies. a mAb 6B6C, b mAb 4G2 and, c mAb 3H12. The mAbs were serially diluted tenfold. The following dilutions were used: a–1, b–1, and c–1, no dilution; a–2, b–2, and c–2, 1:10; a–3, b–3, and c–3, 1:100; a–4, b–4, and c–4, 1:1,000; a–5, b–5, and c–5, 1:10,000. Each of these tenfold serial dilutions was reacted with each dose of the serially diluted challenge virus (1 × 102- 1 × 106 PFU/ml). White bars indicate infection in the presence of mAb using FcγR-expressing BHK cells, and black bars indicate infection in the absence of mAb using FcγR-expressing BHK cells
Detection of DENV-2 infection-enhancement activity of early-phase patient serum samples without dilution and at low dilutions.
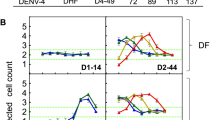
Heat-inactivated serum samples obtained from two patients at the early and late phases of secondary DENV-2 infection were used. The serum samples from patient 1 obtained on day 3 after the onset of disease exhibited ADE activity (3.07- to 27.40-fold enhancement) without dilution (Table 4, Fig. 2a). The level of enhancement of DENV-2 was higher (5.00- to 63.01-fold) at 1:10 dilution than other serum dilutions. The serum samples from patient 2 obtained on day 3 of infection constantly exhibited ADE activity (2.90- to 40.35-fold enhancement) without dilution and at 1:10-1:102 dilutions (Table 5, Fig. 3a). Thus, ADE activity was detected without dilution and at 1:10 dilution for early serum samples from patient 1, and without dilution and at 1:10 dilution for early serum samples from patient 2, using any of the challenge DENV titers of 1 × 102-1 × 106 PFU/ml. The results indicate that in the presence of FcγR, the concentration of reactive antibody, but not the DENV-antibody ratio, determines the presentation of ADE activity of human serum.

Enhancement of DENV-2 infection by serum samples from patient 1. a Early-phase serum sample. b Late-phase serum sample. The serum samples were serially diluted tenfold. The following dilutions were used: a–1 and b–1, no dilution; a–2 and b–2, 1:10; a–3 and b–3, 1:100; a–4 and b–4, 1:1,000; a–5 and b–5, 1:10,000. Each of these tenfold serial dilutions was reacted with each dose of the serially diluted challenge virus (1 × 102-1 × 106 PFU/ml). White bars indicate infection in the presence of patient sera using FcγR-expressing BHK cells, and black bars indicate infection in the absence of sera using FcγR-expressing BHK cells

Enhancement of DENV-2 infection by serum samples from patient 2. a Early-phase serum sample. b Late-phase serum sample. The serum samples were serially diluted tenfold. The following dilutions were used: a–1 and b–1, no dilution; a–2 and b–2, 1:10; a–3 and b–3, 1:100; a–4 and b–4, 1:1,000; a–5 and b–5, 1:10,000. Each of these tenfold serial dilutions was reacted with each dose of the serially diluted challenge virus (1 × 102-1 × 106 PFU/ml). White bars indicate infection in the presence of patient sera using FcγR-expressing BHK cells, and black bars indicate infection in the absence of sera using FcγR-expressing BHK cells
Detection of DENV-2 infection-enhancement activity of late-phase patient serum samples at high dilutions
No ADE activity (enhancement of up to 0.32-fold) was detected for late-phase undiluted serum samples (serum samples obtained from day 12 after onset of disease and day 6 after onset of disease, respectively) from patient 1 (Table 6) and patient 2 (Table 7) using FcγR-expressing cells. ADE activity was constantly detected only at higher serum dilutions (1:103–1:104) for either samples, using any of the challenge DENV titers of 1 × 102-1 × 106 PFU/ml (Fig. 2b and Fig. 3b). The results provide further evidence that the concentration of reactive antibody, but not the DENV-antibody ratio, determines the presentation of ADE activity.
Discussion
In the present study, assay parameters were defined for the in vitro ADE activity of monoclonal antibodies and human serum samples by a conventional plaque titration assay, using FcγR-expressing BHK cells at viral titers of 1 × 102 PFU/ml -1 × 106 PFU/ml. The plaque titers detected in heat-inactivated serum samples were <100 PFU/ml for patient 1 and patient 2. In comparison, virus titers in untreated serum samples were 3.4 × 106 PFU/ml for patient 1 and 7.5 × 106 PFU/ml for patient 2. The results indicate that the heat-inactivated serum samples were not a source of infectious virus in the assays.
A major strength of this method is the ability to detect ADE activity of all four DENV serotypes at a given virus concentration by conventional plaque assays [29, 39]. Here, ADE assessment using an FcγR-expression- based plaque assay makes it possible to visualize plaques and introduce flexibility into incubation times and experimental workflow, and also to determine virus growth directly in infected cells. ADE assays using non-adherent FcγR-expressing cells have been described previously and share some of the features described in the present study in terms the ability to detect ADE activity in undiluted human sera [21]. In the present study, ADE activity was detected using monoclonal antibodies and undiluted and diluted human serum samples, irrespective of challenge DENV titers (102-106PFU/ml). Thus, when using FcγR-positive BHK cells in ADE assays, the concentration of antibodies is a major parameter, whereas the DENV-antibody ratio is a comparatively minor parameter. These results suggest that appropriate titers of challenge DENV could be selected for the ADE assay with only a minimal effect on ADE activity.
Most DENV neutralizing antibodies are speculated to possess ADE activity in vitro at subneutralizing concentrations [40, 41]. The FcγR-expressing BHK cells detected ADE activity using an inoculation dose of as little as 5 PFU per reaction and using both diluted and undiluted serum samples. Additionally, virus growth was detected in cell culture supernatants using as low as 0.1 PFU per inoculation dose with an antibody that possesses ADE activity [39]. These results suggest that the FcγR-expressing BHK cells could provide a useful tool for the elucidation of the ADE mechanism in DENV infection using antibodies induced by either natural infection or vaccination, because the cells confer the ability to detect ADE activity over a wide range of virus concentrations.
The DENV infection-enhancement activity could be influenced by three conditions: virus concentration, antibody concentration, and virus serotype [40]. Although monocyte-lineage cells have proven useful in ADE studies, these cells require different virus titers for each DENV strain to elicit infection, and this may limit the utility of these assays to study ADE mechanisms. Previous studies have shown that ADE is present in undiluted sera during the early phase, but not during the late phase of the disease [21, 27]. Our study confirms the demonstration of ADE activity in the early serum samples without dilution [21, 43]. The FcγR-expressing BHK cells also detected infection-enhancement activity in sera that exhibited ADE activity in THP cells [42]. Additionally, ADE activity was detected at wide ranges of DENV concentrations (Tables 4, 5, 6, 7). Maternal antibodies have been reported to play a significant role in dengue pathogenesis in infants. In FcγR-positive monocytes, maternal dengue antibodies exhibit both virus neutralizing and infection-enhancement activity. These antibodies provide protection against DENV. However, as the antibodies decay, protective activity disappears and the remaining antibodies render infants susceptible to enhanced DENV infection [21, 44]. The DHF hospitalization curve among infants also resembles the titration curve for enhancing antibodies in vitro [45]. Using this schema, in the present study, antibodies were diluted to reflect in vivo antibody decay during DENV infection. Although samples from DHF patients were not included to demonstrate antibody decay in vivo, our study demonstrated that serum samples from patients during the late phase of infection have infection-enhancing activity when diluted, that undiluted serum samples from acute DENV patients have DENV infection-enhancing activity, and that our assay is potentially useful for the detection of infection-enhancing activity of serum samples from DENV patients. The degree of enhancement was also lower when low virus titers were used (Table 4e, Table 5e). These results suggest that antibody concentrations in excess may abrogate ADE, and this highlights the utility of the present assay in ADE studies that require low virus titers or an excess of antibody.
In summary, concentration of antibody rather than DENV-antibody ratio was determined to be the important parameter for the demonstration of DENV infection-enhancement activity using FcγR-expressing BHK cells. The results suggest that the precise definition of DENV titer is not needed in our ADE assay system. Additionally, advantages of the ADE assay based on FcγR-expressing BHK cells include (i) the ability to measure ADE activity by a direct plaque titration method, (ii) the ability to determine ADE activity in undiluted serum samples, (iii) the limited differences in background growth or similar infection threshold using different virus serotypes, and (iv) the ability to detect ADE activity irrespective of challenge DENV titers [39]. Thus, this assay is useful for defining ADE activity in antibody responses in DENV infections.
Abbreviations
- DENV:
-
Dengue virus
- DF:
-
Dengue fever
- DHF:
-
Dengue hemorrhagic fever
- ADE:
-
Antibody-dependent enhancement
- BHK cells:
-
Baby hamster kidney cells
- FcγR:
-
Fc gamma receptor
- PFU:
-
Plaque-forming unit
References
Colpitts TM, Rodenhuis-Zybert I, Moesker B, Wang P, Fikrig E, Smit JM (2011) prM-antibody renders immature West Nile virus infectious in vivo. J Gen Virol 92:2281–2285
Halstead SB, Mahalingam S, Marovich MA, Ubol S, Mosser DM (2010) Intrinsic antibody-dependent enhancement of microbial infection in macrophages: disease regulation by immune complexes. Lancet Infect Dis 10:712–722
Han JF, Cao RY, Deng YQ, Tian X, Jiang T, Qin ED, Qin CF (2011) Antibody dependent enhancement infection of enterovirus 71 in vitro and in vivo. Virol J 8:106
Meyer K, Banerjee A, Frey SE, Belshe RB, Ray R (2011) A weak neutralizing antibody response to hepatitis C virus envelope glycoprotein enhances virus infection. PLoS One 6:e23699
Takeda A, Sweet RW, Ennis FA (1990) Two receptors are required for antibody-dependent enhancement of human immunodeficiency virus type 1 infection: CD4 and Fc gamma R. J Virol 64:605–5610
Beltramello M, Williams KL, Simmons CP, Macagno A, Simonelli L, Quyen NT, Sukupolvi-Petty S, Navarro-Sanchez E, Young PR, de Silva AM, Rey FA, Varani L, Whitehead SS, Diamond MS, Harris E, Lanzavecchia A, Sallusto F (2010) The human immune response to Dengue virus is dominated by highly cross-reactive antibodies endowed with neutralizing and enhancing activity. Cell Host Microbe 8:271–283
Fried JR, Gibbons RV, Kalayanarooj S, Thomas SJ, Srikiatkhachorn A, Yoon IK, Jarman RG, Green S, Rothman AL, Cummings DA (2010) Serotype-specific differences in the risk of dengue hemorrhagic fever: an analysis of data collected in Bangkok, Thailand from 1994 to 2006. PLoS Negl Trop Dis 4:e617
Honda S, Saito M, Dimaano EM, Morales PA, Alonzo MT, Suarez LA, Koike N, Inoue S, Kumatori A, Matias RR, Natividad FF, Oishi K (2009) Increased phagocytosis of platelets from patients with secondary dengue virus infection by human macrophages. Am J Trop Med Hyg 80:841–845
Kurane I, Innis BL, Nisalak A, Hoke C, Nimmannitya S, Meager A, Ennis FA (1989) Human T cell responses to dengue virus antigens. Proliferative responses and interferon gamma production. J Clin Invest 83:506–513
Sierra B, Perez AB, Vogt K, Garcia G, Schmolke K, Aguirre E, Alvarez M, Kern F, Kourí G, Volk HD, Guzman MG (2010) Secondary heterologous dengue infection risk: Disequilibrium between immune regulation and inflammation? Cell Immunol 262:134–140
Sun P, Bauza K, Pal S, Liang Z, Wu SJ, Beckett C, Burgess T, Porter K (2011) Infection and activation of human peripheral blood monocytes by dengue viruses through the mechanism of antibody-dependent enhancement. Virology 421:245–252
Ubol S, Phuklia W, Kalayanarooj S, Modhiran N (2010) Mechanisms of immune evasion induced by a complex of dengue virus and preexisting enhancing antibodies. J Infect Dis 201:923–935
Cummings DA, Irizarry RA, Huang NE, Endy TP, Nisalak A, Ungchusak K, Burke DS (2004) Travelling waves in the occurrence of dengue haemorrhagic fever in Thailand. Nature 427:344–347
Guzman MG, Halstead SB, Artsob H, Buchy P, Farrar J, Gubler DJ, Hunsperger E, Kroeger A, Margolis HS, Martínez E, Nathan MB, Pelegrino JL, Simmons C, Yoksan S, Peeling RW (2010) Dengue: a continuing global threat. Nat Rev Microbiol 8:S7–S16
Murphy BR, Whitehead SS (2011) Immune response to dengue virus and prospects for a vaccine. Annu Rev Immunol 29:587–619
Boonnak K, Slike BM, Burgess TH, Mason RM, Wu SJ, Sun P, Porter K, Rudiman IF, Yuwono D, Puthavathana P, Marovich MA (2008) Role of dendritic cells in antibody-dependent enhancement of dengue virus infection. J Virol 82:3939–3951
Halstead SB, Venkateshan CN, Gentry MK, Larsen LK (1984) Heterogeneity of infection enhancement of dengue 2 strains by monoclonal antibodies. J Immunol 132:1529–1532
Kraus AA, Messer W, Haymore LB, de Silva AM (2007) Comparison of plaque- and flow cytometry-based methods for measuring dengue virus neutralization. J Clin Microbiol 45:3777–3780
Martin NC, Pardo J, Simmons M, Tjaden JA, Widjaja S, Marovich MA, Sun W, Porter KR, Burgess TH (2006) An immunocytometric assay based on dengue infection via DC-SIGN permits rapid measurement of anti-dengue neutralizing antibodies. J Virol Methods 134:74–85
Rodrigo WW, Alcena DC, Kou Z, Rose RC, Jin X, Schlesinger JJ (2009) An automated dengue virus microneutralization plaque assay performed in human Fcγ receptor-expressing CV-1 cells. Am J Trop Med Hyg 80:61–65
Kliks SC, Nisalak A, Brandt WE, Wahl L, Burke DS (1989) Antibody-dependent enhancement of dengue virus growth in human monocytes as a risk factor for dengue hemorrhagic fever. Am J Trop Med Hyg 40:444–451
Burke DS, Kliks S (2005) Antibody-dependent enhancement in dengue virus infections. J Infect Dis 193:601–603
Green S, Libraty DH, Laoprasopwattana K, Ennis FA, Rothman AL (2006) Reply to Halstead and to Burke and Kliks. J Infect Dis 193:603–604
Guy B, Chanthavanich P, Gimenez S, Sirivichayakul C, Sabchareon A, Begue S, Yoksan S, Luxemburger C, Lang J (2004) Evaluation by flow cytometry of antibody-dependent enhancement (ADE) of dengue infection by sera from Thai children immunized with a live-attenuated tetravalent dengue vaccine. Vaccine 22:3563–3574
Littaua R, Kurane I, Ennis FA (1990) Human IgG Fc Receptor II mediates antibody-dependent enhancement of dengue virus infection. J Immunol 144:3183–3186
Mady BJ, Erbe DV, Kurane I, Fanger MW, Ennis FA (1991) Antibody-dependent enhancement of dengue virus infection mediated by bispecific antibodies against cell surface molecules other than Fc gamma receptors. J Immunol 147:3139–3144
Laoprasopwattana K, Libraty DH, Endy TP, Nisalak A, Chunsuttiwat S, Vaughn DW, Reed G, Ennis FA, Rothman AL, Green S (2005) Dengue Virus (DV) enhancing antibody activity in preillness plasma does not predict subsequent disease severity or viremia in secondary DV infection. J Infect Dis 192:510–519
Morens DM, Larsen LK, Halstead SB (1987) Study of the distribution of antibody-dependent enhancement determinants on dengue 2 isolates using dengue 2-derived monoclonal antibodies. J Med Virol 22:163–167
Moi ML, Lim CK, Kotaki A, Takasaki T, Kurane I (2010) Development of an antibody-dependent enhancement assay for dengue virus using stable BHK-21 cell lines expressing Fc gammaRIIA. J Virol Methods 163:205–209
Ito M, Takasaki T, Kotaki A, Tajima S, Yuwono D, Rimal HS, dos Santos F, de Jesus MD, Lina BB, Tsuda Y, Lim CK, Nerome R, Calerés A, Shindo N, Drager RD, Andjaparidze A, Kurane I (2010) Molecular and virological analyses of dengue virus responsible for dengue outbreak in East Timor in 2005. Jpn J Infect Dis 63:181–184
Henchal EA, Gentry MK, McCown JM, Brandt WE (1982) Dengue virus-specific and flavivirus group determinants identified with monoclonal antibodies by indirect immunofluorescence. Am J Trop Med Hyg 31:830–836
Roehrig JT, Mathews JH, Trent DW (1983) Identification of epitopes on the E glycoprotein of Saint Louis encephalitis virus using monoclonal antibodies. Virology 128:118–126
Yamanaka A, Kosugi S, Konishi E (2007) Infection-enhancing and -neutralizing activities of mouse monoclonal antibodies against dengue type 2 and 4 viruses are controlled by complement levels. J Virol 82:927–937
Ito M, Takasaki T, Yamada K, Nerome R, Tajima S, Kurane I (2004) Development and evaluation of fluorogenic TaqMan reverse transcriptase PCR assays for detection of dengue virus types 1 to 4. J Clin Microbiol 42:5935–5937
Ito M, Yamada K, Takasaki T, Pandey B, Nerome R, Tajima S, Morita K, Kurane I (2007) Phylogenetic analysis of dengue viruses isolated from imported dengue patients: possible aid for determining the countries where infections occurred. J Trav Med 14:233–244
Moi ML, Lim CK, Kotaki A, Takasaki T, Kurane I (2011) Detection of higher levels of dengue viremia using FcγR-expressing BHK-21 cells than FcγR-negative cells in secondary infection but not in primary infection. J Infect Dis 203:1405–1414
World Health Organization (2009) Dengue: guidelines for diagnosis, treatment, prevention and control, new edition. Geneva: World Health Organization. http://whqlibdoc.who.int/publications/2009/9789241547871_eng.pdf Accessed 27 Dec 2012
Konishi E, Tabuchi Y, Yamanaka A (2010) A simple assay system for infection-enhancing and -neutralizing antibodies to dengue type 2 virus using layers of semi-adherent K562 cells. J Virol Methods 163:360–367
Moi ML, Lim CK, Tajima S, Kotaki A, Saijo M, Takasaki T, Kurane I (2011) Dengue virus isolation relying on antibody-dependent enhancement mechanism using FcγR-expressing BHK cells and a monoclonal antibody with infection-enhancing capacity. J Clin Virol 52:225–230
Morens DM, Halstead SB (1990) Measurement of antibody-dependent infection enhancement of four dengue virus serotypes by monoclonal and polyclonal antibodies. J Gen Virol 71:2909–2914
Pierson TC, Xu Q, Nelson S, Oliphant T, Nybakken GE, Fremont DH, Diamond MS (2007) The stoichiometry of antibody-mediated neutralization and enhancement of West Nile virus infection. Cell Host Microbe 1:135–145
Moi ML, Lim CK, Chua KB, Takasaki T, Kurane I (2012) Dengue virus infection-enhancing activity in serum samples with neutralizing activity as determined by using FcγR-Expressing cells. PLoS Negl Trop Dis 6(2):e1536
Moi ML, Takasaki T, Saijo M, Kurane I (2013) Dengue virus infection-enhancing activity of undiluted sera obtained from patients with secondary dengue virus infection. Trans R Soc Trop Med Hyg 107(1):51–58
Pengsaa K, Luxemburger C, Sabchareon A, Limkittikul K, Yoksan S, Chambonneau L, Chaovarind U, Sirivichayakul C, Lapphra K, Chanthavanich P, Lang J (2006) Dengue virus infections in the first 2 years of life and the kinetics of transplacentally transferred dengue neutralizing antibodies in Thai children. J Infect Dis 194(11):1570–1576
Halstead SB (2008) Pathogenesis: risk factors prior to infection. In: Halstead SB (ed) Dengue, 1st edn. Imperial College Prese, London, pp 226–227
Acknowledgements
We thank Dr. Eiji Konishi for generously providing us with the 3H12 monoclonal antibody. We also thank Dr. Jeffrey V. Ravetch (Rockefeller University, NY, USA) for generously providing us with the FcγRIIA cDNA, and Dr. Susheela Tridandapani (Ohio State University College of Medicine, Columbus, OH, USA) for assistance in obtaining the FcγRIIA cDNA. This work was supported by grants from Research on Emerging and Re-emerging Infectious Diseases (H23-shinkou-ippan 010) from the Ministry of Health, Labour and Welfare, Japan, a grant-in-aid for Scientific Research (Wakate B No. 23790515) from the Ministry of Education, Culture, Sports, Science and Technology of Japan, and a grant-in-aid from the Cooperative Research Grants of the Institute of Tropical Medicine, Nagasaki University (NEKKEN), 2012 (H24-ippan-16).
Conflicts of interest
None to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Moi, M.L., Takasaki, T., Saijo, M. et al. Determination of antibody concentration as the main parameter in a dengue virus antibody-dependent enhancement assay using FcγR-expressing BHK cells. Arch Virol 159, 103–116 (2014). https://doi.org/10.1007/s00705-013-1787-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00705-013-1787-3