
Abstract
Background
Predicting the fate of patients who are given a misdiagnosis of aneurysmal subarachnoid hemorrhage (aSAH) remains unclear. The purpose was to examine factors associated with initial misdiagnosis of aSAH and to investigate the impact of initial misdiagnosis of aSAH on clinical outcomes.
Methods
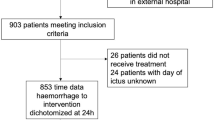
Between January 2007 and December 2015, medical records and radiographic data for 3118 consecutive patients with aSAH were reviewed. There were 33 patients who had been documented with an initial misdiagnosis of aSAH, and all met the following criteria: (1) failure to correctly identify aSAH upon initial presentation to health care professionals; and 2) subsequently documented aSAH after the initial misdiagnosis. After applying exclusion criteria, remaining 2898 patients were included in the control group.
Results
The most common cause of the misdiagnosis is failure to detect aSAH on the initial radiographic imaging. Misdiagnosis group showed lower initial Glasgow Coma Scale, better Hunt-Hess grade, and lower Fisher’s grade. Logistic regression analysis showed that initial HH grade (OR, 0.216; p = 0.014), initial Fisher’s grade (OR, 0.732; p = 0.036), and hospital type during initial contact (OR, 2.266; p = 0.042) were independently associated with misdiagnosis of aSAH.
Conclusions
Patients with initially good HH grade, lower Fisher’s grade, and visiting non-teaching hospital for initial contact were at risk of being misdiagnosed. Misdiagnosis of aSAH in patients with initial good HH grade did affect clinical outcomes negatively. The rebleeding rate was not significantly different between two groups. However, the mortality rate due to rebleeding was higher in MisDx group than in non-MisDx group.

Similar content being viewed by others

References
Barton CW (1994) Evaluation and treatment of headache patients in the emergency department: a survey. Headache 34:91–94
Brennan TA, Hebert LE, Laird NM, Lawthers A, Thorpe KE, Leape LL, Localio AR, Lipsitz SR, Newhouse JP, Weiler PC, Hiatt HH (1991) Hospital characteristics associated with adverse events and substandard care. JAMA 265:3265–3269
Broderick JP, Brott TG, Duldner JE, Tomsick T, Leach A (1994) Initial and recurrent bleeding are the major causes of death following subarachnoid hemorrhage. Stroke 25:1342–1347
Connolly ES Jr, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, Hoh BL, Kirkness CJ, Naidech AM, Ogilvy CS, Patel AB, Thompson BG, Vespa P (2012) Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 43:1711–1737
Edlow JA (2008) Diagnosing headache in the emergency department: what is more important? Being right, or not being wrong? Eur J Neurol 15:1257–1258
Guo LM, Zhou HY, Xu JW, Wang Y, Qiu YM, Jiang JY (2011) Risk factors related to aneurysmal rebleeding. World Neurosurg 76:292–298
Jakobsson KE, Sa ̈veland H, Hillman J, Edner G, Zygmunt S, Brandt L, Pellettieri L (1996) Warning leak and management outcome in aneurysmal subarachnoid hemorrhage. J Neurosurg 85:995–999
Kowalski RG, Claassen J, Kreiter KT, Bates JE, Ostapkovich ND, Connolly ES, Mayer SA (2004) Initial misdiagnosis and outcome after subarachnoid hemorrhage. JAMA 291:866–869
Lim YC, Kim CH, Kim YB, Joo JY, Shin YS, Chung J (2015) Incidence and risk factors for rebleeding during cerebral angiography for ruptured intracranial aneurysms. Yonsei Med J 56:403–409
Matsuda M, Watanabe K, Saito A, Matumura K, Ichikawa M (2007) Circumstances, activities, and events precipitating aneurysmal subarachnoid hemorrhage. J Stroke Cerebrovasc Dis 16:25–29
Mayer PL, Awad IA, Todor R, Harbaugh K, Varnavas G, Lansen TA, Dickey P, Harbaugh R, Hopkins LN (1996) Misdiagnosis of symptomatic cerebral aneurysm: prevalence and correlation with outcome at four institutions. Stroke 27:1558–1563
Naidech AM, Janjua N, Kreiter KT, Ostapkovich ND, Fitzsimmons BF, Parra A, Commichau C, Connolly ES, Mayer SA (2005) Predictors and impact of aneurysm rebleeding after subarachnoid hemorrhage. Arch Neurol 62:410–416
Neil-Dwyer G, Lang D (1997) Brain attack’–aneurysmal subarachnoid haemorrhage: death due to delayed diagnosis. J R Coll Physicians Lond 31:49–52
Ohkuma H, Tsurutani H, Suzuki S (2001) Incidence and significance of early aneurysmal rebleeding before neurosurgical or neurological management. Stroke 32:1176–1180
Ramirez-Lassepas M, Espinosa CE, Cicero JJ, Johnston KL, Cipolle RJ, Barber DL (1997) Predictors of intracranial pathologic findings in patients who seek emergency care because of headache. Arch Neurol 54:1506–1509
Roos YB, de Haan RJ, Beenen LF, Groen RJ, Albrecht KW, Vermeulen M (2000) Complications and outcome in patients with aneurysmal subarachnoid haemorrhage: a prospective hospital-based cohort study in the Netherlands. J Neurol Neurosurg Psychiatry 68:337–341
Schievink WI (1997) Intracranial aneurysms. N Engl J Med 336:28–40
Schievink WI, Wijdicks EF, Parisi JE, Piepgras DG, Whisnant JP (1995) Sudden death from aneurysmal subarachnoid hemorrhage. Neurology 45:871–874
Solenski NJ, Haley EC Jr, Kassell NF, Kongable G, Germanson T, Truskowski L, Torner JC (1995) Medical complications of aneurysmal subarachnoid hemorrhage: a report of the multicenter, cooperative aneurysm study. Participants of the Multicenter Cooperative Aneurysm Study Crit Care Med 23:1007–1017
Truelsen T, Bonita R, Duncan J, Anderson NE, Mee E (1998) Changes in subarachnoid hemorrhage mortality, incidence, and case fatality in New Zealand between 1981–1983 and 1991–1993. Stroke 29:2298–2303
van Gijn J, Kerr RS, Rinkel GJ (2007) Subarachnoid haemorrhage. Lancet 369:306–318
van Gijn J, Rinkel GJ (2001) Subarachnoid haemorrhage: diagnosis, causes and management. Brain 124:249–278
Vermeulen MJ, Schull MJ (2007) Missed diagnosis of subarachnoid hemorrhage in the emergency department. Stroke 38:1216–1221
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of retrospective study formal consent is not required.
Rights and permissions
About this article

Cite this article
Oh, Sy., Lim, Y.C., Shim, Y.S. et al. Initial misdiagnosis of aneurysmal subarachnoid hemorrhage: associating factors and its prognosis. Acta Neurochir 160, 1105–1113 (2018). https://doi.org/10.1007/s00701-018-3552-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-018-3552-6