
Abstract
Background
The objective of this study was to compare the three most prominent systems for stereotactic radiosurgery in terms of dosimetric characteristics: the Cyberknife system, the Gamma Knife Perfexion and the Novalis system.
Methods
Ten patients treated for recurrent grade I meningioma after surgery using the Cyberknife system were identified; the Cyberknife contours were exported and comparative treatment plans were generated for the Novalis system and Gamma Knife Perfexion. Dosimetric values were compared with respect to coverage, conformity index (CI), gradient index (GI) and beam-on time (BOT).
Results
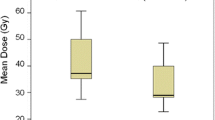
All three systems showed comparable results in terms of coverage. The Gamma Knife and the Cyberknife system showed significantly higher levels of conformity than the Novalis system (Cyberknife vs Novalis, p = 0.002; Gamma Knife vs Novalis, p = 0.002). The Gamma Knife showed significantly steeper gradients compared with the Novalis and the Cyberknife system (Gamma Knife vs Novalis, p = 0.014; Gamma Knife vs Cyberknife, p = 0.002) and significantly longer beam-on times than the other two systems (BOT = 66 ± 21.3 min, Gamma Knife vs Novalis, p = 0.002; Gamma Knife vs Cyberknife, p = 0.002).
Conclusions
The multiple focal entry systems (Gamma Knife and Cyberknife) achieve higher conformity than the Novalis system. The Gamma Knife delivers the steepest dose gradient of all examined systems. However, the Gamma Knife is known to require long beam-on times, and despite worse dose gradients, LINAC-based systems (Novalis and Cyberknife) offer image verification at the time of treatment delivery.

Similar content being viewed by others


References
Adler JR Jr, Chang SD, Murphy MJ, Doty J, Geis P, Hancock SL (1997) The Cyberknife: a frameless robotic system for radiosurgery. Stereotact Funct Neurosurg 69:124–128
Chen JC, Girvigian M, Greathouse H, Miller M, Rahimian J (2004) Treatment of trigeminal neuralgia with linear accelerator radiosurgery: initial results. J Neurosurg 101(Suppl 3):346–350
Claus EB, Bondy ML, Schildkraut JM, Wiemels JL, Wrensch M, Black PM (2005) Epidemiology of intracranial meningioma. Neurosurgery 57:1088–1095, discussion 1088–1095
Gevaert T, Levivier M, Lacornerie T, Verellen D, Engels B, Reynaert N, Tournel K, Duchateau M, Reynders T, Depuydt T, Collen C, Lartigau E, De Ridder M (2013) Dosimetric comparison of different treatment modalities for stereotactic radiosurgery of arteriovenous malformations and acoustic neuromas. Radiother Oncol 106:192–197
Leksell L (1951) The stereotaxic method and radiosurgery of the brain. Acta Chir Scand 102:316–319
Lindquist C, Paddick I (2007) The Leksell Gamma Knife Perfexion and comparisons with its predecessors. Neurosurgery 61:130–140, discussion 140–131
Ma L, Sahgal A, Descovich M, Cho YB, Chuang C, Huang K, Laperriere NJ, Shrieve DC, Larson DA (2010) Equivalence in dose fall-off for isocentric and nonisocentric intracranial treatment modalities and its impact on dose fractionation schemes. Int J Radiat Oncol Biol Phys 76:943–948
Mirimanoff RO, Dosoretz DE, Linggood RM, Ojemann RG, Martuza RL (1985) Meningioma: analysis of recurrence and progression following neurosurgical resection. J Neurosurg 62:18–24
Paddick I (2000) A simple scoring ratio to index the conformity of radiosurgical treatment plans. Technical note. J Neurosurg 93(Suppl 3):219–222
Paddick I, Lippitz B (2006) A simple dose gradient measurement tool to complement the conformity index. J Neurosurg 105(Suppl):194–201
Petti PL, Larson DA, Kunwar S (2008) Use of hybrid shots in planning Perfexion Gamma Knife treatments for lesions close to critical structures. J Neurosurg 109(Suppl):34–40
Conflicts of interest
V. Budach and M. Kufeld received travel and speech grants from Accuray Inc.
The other authors confirm that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
This article is the latest in a series of papers comparing different devices for stereotactic radiosurgery. The obvious aim of such papers is to see which one is “best”, perhaps with the aim of making purchase of these machines more attractive, or indeed for patients or referring doctors to choose one or other department for treatment.
Most of these papers suffer from the weakness that there is no simple answer to this question: the different comparison parameters favour one or another technology. This leaves the reader somewhat uncertain how to interpret the findings.
It is a strength of this paper that they calculated the necessary beam-on-time, which is not often shown in previous papers. This is a relevant feature for the delivery of the treatment on the day. Of course it is only part of the whole process, as the planning time is also vastly different (according to the information available to me it is the fastest using GammaPlan, the software utilised for Gamma Knife treatments. There is recent evidence to show that the biological equivalent dose (BED) depends on the length of time the radiation treatment is delivered, because of the fast component of cell repair that is in operation even during the treatment. As this factor is so dramatically different in the three technologies, experience with one machine (most clinical data are published with the Gamma Knife), cannot be automatically utilised for the faster LINAC based machines.
Andras Kemeny
Sheffield, UK
Hopewell JW, Millar WT, Lindquist C (2012) Radiobiological principles: their application to γ knife therapy. Prog Neurol Surg 25:39-54
David Kaul and Harun Badakhshi contributed equally to this study.
Rights and permissions
About this article

Cite this article
Kaul, D., Badakhshi, H., Gevaert, T. et al. Dosimetric comparison of different treatment modalities for stereotactic radiosurgery of meningioma. Acta Neurochir 157, 559–564 (2015). https://doi.org/10.1007/s00701-014-2272-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-014-2272-9