
Abstract
Background
The Ommaya reservoir for intraventricular chemotherapy of leptomeningeal carcinomatosis (LMC) patients has been reported to have some complications. We introduced a Chemoport reservoir, with a solid non-collapsible, high-profile chamber as a the replacement for the Ommaya reservoir in LMC patients.
Objective
To evaluate the usefulness of Chemoport as an alternative to Ommaya for the intraventricular chemotherapy of LMC.
Methods
The medical records of 155 patients (89 Ommaya and 66 Chemoport) who underwent intraventricular chemotherapy via a subgaleal reservoir were reviewed. Chemoport was secured with engraving of skull.
Result
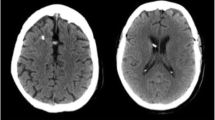
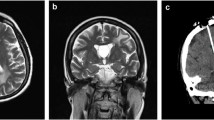
Reservoir malfunction, including one intracranial hemorrhage (ICH) under the burr hole occurred, in six patients. During the course of therapy, cerebrospinal fluid (CSF) infection was diagnosed in 19 patients and intraventricular hemorrhage with ICH was evident in three patients of the Ommaya group. Incidence of the above-mentioned complications showed no difference between the two groups. CSF leakage under a galeal flap or through a wound edge occurred more frequently in the Ommaya group (12 patients) than in the Chemoport group (two patients) and the difference was statistically significant (p = 0.03). One-hundred and four patients showed increased intracranial pressure (ICP) and 74 of them received additional CSF drainage to control increased ICP by either intermittent CSF drainage in both groups or continuous extraventricular drainage (EVD) of CSF using designated hooked needle only in the Chemoport group. Among the factors related to the control ICP, the number of chemotherapies, type of reservoir in favor of Chemoport, and EVD showed significantly improved control of ICP (p < 0.05).
Conclusion
Chemoport, as a reservoir for intraventricular chemotherapy, has superior ICP control at an equal or lower rate of complications compared with the Ommaya reservoir.


Similar content being viewed by others

References
Al-Anazi A, Bernstein M (2000) Modified stereotactic insertion of the Ommaya reservoir. Technical note. J Neurosurg 92:1050–1052
Blasberg RG, Patlak CS, Shapiro WR (1977) Distribution of methotrexate in the cerebrospinal fluid and brain after intraventricular administration. Cancer Treat Rep 61:633–641
Bleyer WA, Pizzo PA, Spence AM, Platt WD, Benjamin DR, Kolins CJ, Poplack DG (1978) The Ommaya reservoir: newly recognized complications and recommendations for insertion and use. Cancer 41:2431–2437
Chamberlain MC (1998) Radioisotope CSF flow studies in leptomeningeal metastases. J Neurooncol 38:135–140
Chamberlain MC, Kormanik P (1998) Carcinoma meningitis secondary to non-small cell lung cancer: combined modality therapy. Arch Neurol 55:506–512
Chamberlain MC, Kormanik PA (1996) Prognostic significance of 111indium-DTPA CSF flow studies in leptomeningeal metastases. Neurology 46:1674–1677
Chamberlain MC, Kormanik PA, Barba D (1997) Complications associated with intraventricular chemotherapy in patients with leptomeningeal metastases. J Neurosurg 87:694–699
Freilich RJ, Krol G, DeAngelis LM (1995) Neuroimaging and cerebrospinal fluid cytology in the diagnosis of leptomeningeal metastasis. Ann Neurol 38:51–57
Grossman SA, Trump DL, Chen DC, Thompson G, Camargo EE (1982) Cerebrospinal fluid flow abnormalities in patients with neoplastic meningitis. An evaluation using 111indium-DTPA ventriculography. Am J Med 73:641–647
Hitchins RN, Bell DR, Woods RL, Levi JA (1987) A prospective randomized trial of single-agent versus combination chemotherapy in meningeal carcinomatosis. J Clin Oncol 5:1655–1662
Jacobs A, Clifford P, Kay HE (1981) The Ommaya reservoir in chemotherapy for malignant disease in the CNS. Clin Oncol 7:123–129
Lemann W, Wiley RG, Posner JB (1988) Leukoencephalopathy complicating intraventricular catheters: clinical, radiographic and pathologic study of 10 cases. J Neurooncol 6:67–74
Lishner M, Perrin RG, Feld R, Messner HA, Tuffnell PG, Elhakim T, Matlow A, Curtis JE (1990) Complications associated with Ommaya reservoirs in patients with cancer. The Princess Margaret Hospital experience and a review of the literature. Arch Intern Med 150:173–176
Little JR, Dale AJ, Okazaki H (1974) Meningeal carcinomatosis. Clinical manifestations. Arch Neurol 30:138–143
Obbens EA, Leavens ME, Beal JW, Lee YY (1985) Ommaya reservoirs in 387 cancer patients: a 15-year experience. Neurology 35:1274–1278
Olson ME, Chernik NL, Posner JB (1974) Infiltration of the leptomeninges by systemic cancer. A clinical and pathologic study. Arch Neurol 30:122–137
Ommaya AK (1963) Subcutaneous reservoir and pump for sterile access to ventricular cerebrospinal fluid. Lancet 2:983–984
Ongerboer de Visser BW, Somers R, Nooyen WH, van Heerde P, Hart AA, McVie JG (1983) Intraventricular methotrexate therapy of leptomeningeal metastasis from breast carcinoma. Neurology 33:1565–1572
Sandberg DI, Bilsky MH, Souweidane MM, Bzdil J, Gutin PH (2000) Ommaya reservoirs for the treatment of leptomeningeal metastases. Neurosurgery 47:49–54, discussion 54–45
Shapiro WR, Posner JB, Ushio Y, Chemik NL, Young DF (1977) Treatment of meningeal neoplasms. Cancer Treat Rep 61:733–743
Wasserstrom WR, Glass JP, Posner JB (1982) Diagnosis and treatment of leptomeningeal metastases from solid tumors: experience with 90 patients. Cancer 49:759–772
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
Gwak et al. bring new technical advances using the non-collapsible chamber Chemoport compared with the “classical” Ommaya reservoir for intra-ventricular chemotherapy of leptomeningeal carcinomatosis (LMC). Although the implantation of the Chemoport needs more work to enable the incorporation of the bulky reservoir into the skull by drilling the outer table, it has many advantages, especially the thick Silastic dome can be repeatedly punctured with practically no time limit. Another important new issue is the possibility to drain continuously the CSF in case of raised ICP with a special hooked needle introduced transcutaneously in the Chemoport without the risk of having the needle being inadvertently pulled and therefore obtaining the same effect as an EVD.
Benedict Rilliet
Geneva, Switzerland
Comment
Metastases of the CNS becoming increasingly common as cancer patients live longer. In multiple metastases of the brain tissue, whole brain irradiation (WBC) is often so effective in melting the lesions that patients succumb to metastases elsewhere in the body.
Leptomeningeal dissemination ('neoplastic meningitis') usually by far more devastating and resistant to the present modes of treatment with survival ranges from 8–16 weeks (1). The management requires a multidisciplinary team to palliate CNS symptoms – according to the type of primary cancer – by WBC, systemic chemotherapy, and placement of ventricular reservoirs for both intrathecal chemotherapy and alleviation of hydrocephalus by repeated punctures.
Chemoport is usually introduced into a vein for transcutaneous delivery of chemotherapy. Korean colleagues in their well-written and detailed study compared the usefulness of Chemoport (n = 66) vs Ommaya reservoir (n = 89) in intraventricular chemotherapy of leptomeningeal carcinomatosis. They conclude that Chemoport – with designated hooked needle with plastic wings that prevent slipping – is more suitable for intermittent CSF drainage that many of these pateints require. Most importanty, the Chemoport reservoir may be punctured hundreds of times without leakage that typically pesters the thinner Ommaya reservoir. The implantion reguires more bone work but the use of Chemoport reservoir should be tested and reported by other neuro-oncology teams.
Juha E Jääskeläinen
Kuopio, Finland
1. Beauchesne P. Intrathecal chemotherapy for treatment of leptomeningeal dissemination of metastatic tumours. Lancet Oncol 2010;11:871-9. Review.
This retrospective study was approved by Institutional Review Board of National Cancer Center Korea (NCCNCS-11-436).
Rights and permissions
About this article
Cite this article
Gwak, HS., Lee, CH., Yang, H.S. et al. Chemoport with a non-collapsible chamber as a replacement for an Ommaya reservoir in the treatment of leptomeningeal carcinomatosis. Acta Neurochir 153, 1971–1978 (2011). https://doi.org/10.1007/s00701-011-1086-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-011-1086-2