
Abstract
Purpose
The neurological outcome of cervical spondylotic myelopathy (CSM) may depend on multiple factors, including age, symptom duration, cord compression ratio, cervical curvature, canal stenosis, and factors related to magnetic resonance (MR) signal intensity (SI). Each factor may act independently or interactively with others. To clarify the factors in prognosis, we prospectively analyzed the outcomes of patients with myelopathy caused by soft disc herniation in correlation with magnetic resonance imaging (MRI) findings and other clinical parameters.
Materials and methods
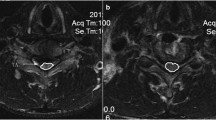
From June 2006 to July 2009, we performed surgical operations in 137 patients with CSM. Of these patients, 70 (51.1%), including 45 men and 25 women with ventral cord compression at one or two levels, underwent anterior cervical discectomy and fusion. The mean duration of follow-up was 32.7 months. We surveyed the cervical curvature index (CCI), canal stenosis (Torg–Pavlov ratio), cord compression ratio, the length of SI change on T2WI, and clinical outcome using the Japanese Orthopedic Association (JOA) score for cervical myelopathy. The MRI SI was evaluated by grade: grade 0, no change in signal intensity; grade 1, light signal change; and grade 2, bright signal change on the T2WI. Multifactorial effects were identified by regression analysis.
Results
The mean preoperative and postoperative JOA scores were 10.5 ± 2.9 and 14.9 ± 2.1, respectively (p < 0.05). The mean recovery rate based on the JOA score was 70.0 ± 20.1%. The respective preoperative JOA scores and recovery ratios(%) were 11.6 ± 2.3 and 81.5 ± 17.0% in 20 patients with SI grade 0; 10.8 ± 2.3 and 70.1 ± 17.3% in 25 patients with grade 1; and 9.2 ± 3.6 and 60.7 ± 20.9% in 25 patients with grade 2, respectively. Post-surgical neurological outcome showed no significant relationship to age, symptom duration, cervical alignment, stenosis, or cord compression.
Conclusions
Among the variables tested, preoperative neurological status and intramedullary signal intensity were significantly related to neurological outcome. The better the preoperative neurological status was, the better the post-operative neurological outcome. The SI grade on the preoperative T2WI was negatively related to neurological outcome. Hence, the severity of SI change and preoperative neurological status emerged as significant prognostic factors in post-operative CSM.






Similar content being viewed by others


References
Al-Mefty O, Harkey HL, Marawi I, Haines DE, Peeler DF, Wilner HI, Smith RR, Holaday HR, Haining JL, Russell WF, Harrison B, Middleton TH (1993) Experimental chronic compressive cervical myelopathy. J Neurosurg 79:550–561
Baba H, Furusawa N, Chen Q, Imura S, Tomita K (1995) Anterior decompressive surgery for cervical ossified posterior longitudinal ligament causing myeloradiculopathy. Paraplegia 33:18–24
Baba H, Uchida K, Maezawa Y, Furusawa N, Azuchi M, Imura S (1996) Lordotic alignment and posterior migration of the spinal cord following en bloc open-door laminoplasty for cervical myelopathy: a magnetic resonance imaging study. J Neurol 243:626–632
Batzdorf U, Flannigan BD (1991) Surgical decompressive procedures for cervical spondylotic myelopathy. A study using magnetic resonance imaging. Spine (Phila Pa 1976) 16:123–127
Benzel EC (1995) Cervical spondylotic myelopathy. J Neurosurg 83:942–943
Breig A, el-Nadi AF (1966) Biomechanics of the cervical spinal cord. Relief of contact pressure on and overstretching of the spinal cord. Acta Radiol Diagn (Stockh) 4:602–624
Carette S, Fehlings MG (2005) Clinical practice, cervical radiculopathy. N Engl J Med 353:392–399
Chatley A, Kumar R, Jain VK, Behari S, Sahu RN (2009) Effect of spinal cord signal intensity changes on clinical outcome after surgery for cervical spondylotic myelopathy. J Neurosurg Spine 11:562–567
Chiles BW 3rd, Leonard MA, Choudhri HF, Cooper PR (1999) Cervical spondylotic myelopathy: patterns of neurological deficit and recovery after anterior cervical decompression. Neurosurgery 44:762–769, discussion 769–770
Crandall PH, Batzdorf U (1966) Cervical spondylotic myelopathy. J Neurosurg 25:57–66
Edwards WC, LaRocca H (1983) The developmental segmental sagittal diameter of the cervical spinal canal in patients with cervical spondylosis. Spine (Phila Pa 1976) 8:20–27
Fessler RG, Steck JC, Giovanini MA (1998) Anterior cervical corpectomy for cervical spondylotic myelopathy. Neurosurgery 43:257–265, discussion 265-257
Fujiwara K, Yonenobu K, Ebara S, Yamashita K, Ono K (1989) The prognosis of surgery for cervical compression myelopathy. An analysis of the factors involved. J Bone Jt Surg Br 71:393–398
Gwinn DE, Iannotti CA, Benzel EC, Steinmetz MP (2009) Effective lordosis: analysis of sagittal spinal canal alignment in cervical spondylotic myelopathy. J Neurosurg Spine 11:667–672
Hirabayashi K, Miyakawa J, Satomi K, Maruyama T, Wakano K (1981) Operative results and postoperative progression of ossification among patients with ossification of cervical posterior longitudinal ligament. Spine (Phila Pa 1976) 6:354–364
Hukuda S, Xiang LF, Imai S, Katsuura A, Imanaka T (1996) Large vertebral body, in addition to narrow spinal canal, are risk factors for cervical myelopathy. J Spinal Disord 9:177–186
Ishihara A (1968) Roentgenographic studies on the normal pattern of the cervical curvature. Nippon Seikeigeka Gakkai Zasshi 42:1033–1044
Ito T, Oyanagi K, Takahashi H, Takahashi HE, Ikuta F (1996) Cervical spondylotic myelopathy. Clinicopathologic study on the progression pattern and thin myelinated fibers of the lesions of seven patients examined during complete autopsy. Spine (Phila Pa 1976) 21:827–833
King JT Jr, McGinnis KA, Roberts MS (2003) Quality of life assessment with the medical outcomes study short form-36 among patients with cervical spondylotic myelopathy. Neurosurgery 52:113–120, discussion 121
Kohno K, Kumon Y, Oka Y, Matsui S, Ohue S, Sakaki S (1997) Evaluation of prognostic factors following expansive laminoplasty for cervical spinal stenotic myelopathy. Surg Neurol 48:237–245
Koyanagi T, Hirabayashi K, Satomi K, Toyama Y, Fujimura Y (1993) Predictability of operative results of cervical compression myelopathy based on preoperative computed tomographic myelography. Spine (Phila Pa 1976) 18:1958–1963
Larsson EM, Holtas S, Nilsson O (1989) Gd-DTPA-enhanced MR of suspected spinal multiple sclerosis. AJNR Am J Neuroradiol 10:1071–1076
Matsuda Y, Miyazaki K, Tada K, Yasuda A, Nakayama T, Murakami H, Matsuo M (1991) Increased MR signal intensity due to cervical myelopathy. Analysis of 29 surgical cases. J Neurosurg 74:887–892
Mehalic TF, Pezzuti RT, Applebaum BI (1990) Magnetic resonance imaging and cervical spondylotic myelopathy. Neurosurgery 26:217–226, discussion 226-217
Mizuno J, Nakagawa H, Inoue T, Hashizume Y (2003) Clinicopathological study of "snake-eye appearance" in compressive myelopathy of the cervical spinal cord. J Neurosurg 99:162–168
Mizuno J, Nakagawa H, Iwata K, Hashizume Y (1992) Pathology of spinal cord lesions caused by ossification of the posterior longitudinal ligament, with special reference to reversibility of the spinal cord lesion. Neurol Res 14:312–314
Morimoto T, Yamada T, Nagata K, Matsuyama T, Sakaki T (1996) Intramedullary gadolinium-DTPA enhancement in a patient with cervical spondylotic myelopathy and an associated vascular lesion. Case report. Neurosurg Focus 1:e3
Morio Y, Teshima R, Nagashima H, Nawata K, Yamasaki D, Nanjo Y (2001) Correlation between operative outcomes of cervical compression myelopathy and mri of the spinal cord. Spine (Phila Pa 1976) 26:1238–1245
Morio Y, Yamamoto K, Kuranobu K, Murata M, Tuda K (1994) Does increased signal intensity of the spinal cord on MR images due to cervical myelopathy predict prognosis? Arch Orthop Trauma Surg 113:254–259
Murone I (1974) The importance of the sagittal diameters of the cervical spinal canal in relation to spondylosis and myelopathy. J Bone Joint Surg Br 56:30–36
Nilsson P, Sandberg-Wollheim M, Norrving B, Larsson EM (2007) The role of MRI of the brain and spinal cord, and CSF examination for the diagnosis of primary progressive multiple sclerosis. Eur J Neurol 14:1292–1295
Pavlov H, Torg JS, Robie B, Jahre C (1987) Cervical spinal stenosis: determination with vertebral body ratio method. Radiology 164:771–775
Ramanauskas WL, Wilner HI, Metes JJ, Lazo A, Kelly JK (1989) MR imaging of compressive myelomalacia. J Comput Assist Tomogr 13:399–404
Suzuki E, Nakamura H, Konishi S, Yamano Y (2002) Analysis of the spastic gait caused by cervical compression myelopathy. J Spinal Disord Tech 15:519–522
Sze G, Krol G, Zimmerman RD, Deck MD (1988) Intramedullary disease of the spine: diagnosis using gadolinium-DTPA-enhanced MR imaging. AJR Am J Roentgenol 151:1193–1204
Takahashi M, Sakamoto Y, Miyawaki M, Bussaka H (1987) Increased MR signal intensity secondary to chronic cervical cord compression. Neuroradiology 29:550–556
Takahashi M, Yamashita Y, Sakamoto Y, Kojima R (1989) Chronic cervical cord compression: clinical significance of increased signal intensity on MR images. Radiology 173:219–224
Uchida K, Nakajima H, Sato R, Yayama T, Mwaka ES, Kobayashi S, Baba H (2009) Cervical spondylotic myelopathy associated with kyphosis or sagittal sigmoid alignment: outcome after anterior or posterior decompression. J Neurosurg Spine 11:521–528
Wada E, Yonenobu K, Suzuki S, Kanazawa A, Ochi T (1999) Can intramedullary signal change on magnetic resonance imaging predict surgical outcome in cervical spondylotic myelopathy? Spine (Phila Pa 1976) 24:455–461, discussion 462
Yamazaki T, Yanaka K, Sato H, Uemura K, Tsukada A, Nose T (2003) Cervical spondylotic myelopathy: surgical results and factors affecting outcome with special reference to age differences. Neurosurgery 52:122–126, discussion 126
Yone K, Sakou T, Yanase M, Ijiri K (1992) Preoperative and postoperative magnetic resonance image evaluations of the spinal cord in cervical myelopathy. Spine (Phila Pa 1976) 17:S388–392
Yukawa Y, Kato F, Ito K, Horie Y, Hida T, Machino M, Ito ZY, Matsuyama Y (2008) Postoperative changes in spinal cord signal intensity in patients with cervical compression myelopathy: comparison between preoperative and postoperative magnetic resonance images. J Neurosurg Spine 8:524–528
Yukawa Y, Kato F, Yoshihara H, Yanase M, Ito K (2007) MR T2 image classification in cervical compression myelopathy: predictor of surgical outcomes. Spine (Phila Pa 1976) 32:1675–1678, discussion 1679
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article
Cite this article
Shin, J.J., Jin, B.H., Kim, K.S. et al. Intramedullary high signal intensity and neurological status as prognostic factors in cervical spondylotic myelopathy. Acta Neurochir 152, 1687–1694 (2010). https://doi.org/10.1007/s00701-010-0692-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-010-0692-8