
Abstract
Introduction
Five billion people worldwide do not have timely access to surgical care. Cinterandes is one of the only mobile surgical units in low- and middle-income countries. This paper examines the methodology that Cinterandes uses to deliver mobile surgery.
Methods
Founding and core staff were interviewed, four missions were participated in, and internal documents and records were analysed between 1 May and 1 July 2014.
Results
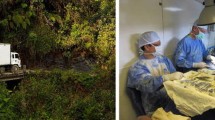
Cinterandes performed 7641 operations over the last 20 years (60% gastrointestinal/laparoscopic), travelling 300,000 km to remote areas of Ecuador. The mobile surgery programme was initiated by a local Ecuadorian surgeon in 1980. Funding was acquired from businesses, private hospitals, and individuals, to fund a low-cost surgical truck, simple equipment, and running costs. The mobile surgical unit is a 24-foot modified Isuzu truck containing a preparation room with general equipment storage and running water, together with an operating room including the operating table, anaesthetic and surgical equipment. Mission structure includes: patient identification by a network of local medical personnel in remote regions; pre-operative assessment at 1 week by core team via teleconsultations; four-day surgical missions; post-operative recovery in tents or a local clinic; post-operative follow-up care by local personnel and remote teleconsultations. The permanent core team includes seven members; lead surgeon, lead anaesthetist, operating-room technician, medical coordinator, driver, general coordinator, and receptionist. Additional support members include seven regular surgeons, residents, medical students, and volunteers.
Conclusion
Surgery is a very effective way to gain the trust of the community, due to immediate results. Trust opens doors to other programmes (e.g. family medicine). Surgery can be incorporated with all other aspects of health care, which can in turn be incorporated with all other aspects of human development, education, food production and nutrition, housing, work and productivity, communication, and recreation.








Similar content being viewed by others


References
Meara JG, Leather AJ, Hagander L et al (2015) Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet 386(9993):569–624
Weiser TG, Regenbogen SE, Thompson KD et al (2008) An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet 372(9633):139–144
Grimes CE, Bowman KG, Dodgion CM et al (2011) Systematic review of barriers to surgical care in low-income and middle-income countries. World J Surg 35:941–950
Grimes CE, Law RSL, Borgstein ES et al (2012) Systematic review of met and unmet need of surgical disease in rural sub-Saharan Africa. World J Surg 36:8–23
Rodas E, Vicuña AL, Rodas EB (2014) President, Founder, and Lead Surgeon. Cinterandes Foundation. 25 interviews with the author between 01/05/2014 and 01/07/2014. Personal communication
Cinterandes Foundation (1980–2014). Internal documents, reports, and databases. Cinterandes Central Office, Cuenca, Ecuador. Unpublished
Fontana M, Lucha P, Snyder M et al (1999) Surgery aboard ship: is it safe? Mil Med 164(9):613–615
Cheng LHH, McColl L, Parker G (2012) Thyroid surgery in the UK and on board the Mercy Ships. Br J Oral Maxillofac Surg 50(7):592–596
Sechriest VF, Lhowe DW (2008) Orthopaedic care aboard the USNS Mercy during operation unified assistance after the 2004 Asian Tsunami. J Bone Joint Surg Am 90(4):849–861
Price MD, Shalabi HT, Shalabi ST et al (2015) Is mobile surgery successful in overcoming patient barriers to surgery? Poster session presented at: Extreme Affordability Global Health Conference 2015, Centre for Global Surgery, University of Utah. 3rd Annual Conference. 10–11 April 2015; Salt Lake City, Utah, USA
Mora F, Cone S, Rodas E et al (2006) Telemedicine and electronic health information for clinical continuity in a mobile surgery program. World J Surg 30:1128–1134
Central Intelligence Agency (2015) Ecuador. In The World Factbook. www.cia.gov/library/publications/the-world-factbook/geos/ec.html. Last Accessed 17/04/2015
Shalabi HT, Price MD, Shalabi ST et al (2015) Cost-effectiveness of mobile surgery in low- and middle-income countries: an Ecuadorian case study. Oral presentation at: 46th World Congress of Surgery. International Society of Surgery. 23–27 August 2015; Bangkok, Thailand
Chao TE, Sharma K, Mandigo M et al (2014) Cost-effectiveness of surgery and its policy implications for global health: a systematic review and analysis. Lancet Glob Health 2:e334–e345
De Vries C, Price R (2010) Global surgery and public health: a new paradigm. Jones and Bartlett, Sudbury
Doorslaer V, O’Donnell O, Rannan-Eliya RP et al (2006) Effect of payments for health care on poverty estimates in 11 countries in Asia: an analysis of household survey data. Lancet 368(9544):1357–1364
Bickler SW, Weiser TG, Kassenbaum N et al (2014) Chapter 2: Global burden of surgical conditions. In: Disease control priorities, 3rd edn: Economic Evaluation for Health. World Bank, Washington
Acknowledgments
Dr. Edgar Rodas, founder and leader of Cinterandes since inception in 1980, sadly passed away on 2 March 2015. It is because of his visions and fortitude that Cinterandes has remained one of the most successful mobile surgical units in the developing world, dedicated to treating the poor and remote population. The methodology, concepts, and principles of Cinterandes examined in this paper were his visions and ideologies. This paper is dedicated in his memory. Further acknowledgements and thanks are made to Freddy Peralta (operating-room technician), Gonzalo Matute (driver and assistant), Carolina Donoso (general coordinator), Janeth Matute Mendoza (administration manager), and Dolores Rodas (visionary) for their substantial aid and initiatives in acquiring archived and current data and documents.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
HT Shalabi, MD Price, ST Shalabi, EB Rodas, AL Vicuña, B Guzhñay, RR Price, and E Rodas have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Shalabi, H.T., Price, M.D., Shalabi, S.T. et al. Mobile gastrointestinal and endoscopic surgery in rural Ecuador: 20 years’ experience of Cinterandes. Surg Endosc 31, 4964–4972 (2017). https://doi.org/10.1007/s00464-016-4992-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-016-4992-9