
Abstract
Background
An understanding of the relationship between patient factors and healthcare resource utilization represents a major point of interest for optimizing clinical care and overall net savings, yet maintaining financial margins for provider revenues. This study aims to review resource utilization after cholecystectomy in order to characterize patient factors associated with increased postoperative ED visits and 30-day readmissions.
Methods
A total of 53,632 open and laparoscopic cholecystectomies were reviewed from July 2009 to December 2010 in a large private payer claims database. ICD-9 and CPT codes were available for each event, as well as basic demographics. Data regarding 30-day postoperative resource utilization metrics (emergency department visits and inpatient hospitalizations) were analyzed and stratified by key patient comorbidities. Differences between subgroups were evaluated with univariate and multivariable methods.
Results
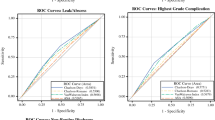
Of the 53,632 patients studied, 71.2 % (38,171) were female and 28.8 % (15,461) male. Resource utilization within 30 days of surgery included: 6.6 % (3538) of patients with an ED visit and 7.7 % (4103) with an inpatient hospitalization. The most common comorbidities in the study population were: hypertension, hyperlipidemia, GERD/hiatal hernia, and diabetes mellitus. Patients with heart failure, cirrhosis, and a history of MI or acute ischemic heart disease all had a significant association with postoperative ED visit and the highest likelihood of inpatient hospitalization. Angina, diabetes, and hypertension similarly increased both ED utilization and inpatient readmissions to a lesser but still significant extent. Although patients with GERD/hiatal hernia and sleep apnea had a significant association with ED use, they did not have an increased likelihood of readmission.
Conclusions
Patient comorbidity indexing plays a major role in clinical risk stratification and resource utilization for cholecystectomy. These factors should be considered in bundled reimbursement packages and in the creation of preventive postoperative ambulatory strategies given their role in determining potential resource utilization in the postoperative setting.
Similar content being viewed by others


Notes
Lengths of stay were calculated by subtracting discharge date from admission date. LOS of 0 days informs that the admission and discharge date were the same, suggesting discharge from the hospital before midnight on the same day as admission.
References
Everhart JE, Ruhl CE (2009) Burden of digestive diseases in the United States part I: overall and upper gastrointestinal diseases. Gastroenterology 136:376–386
Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T (2003) Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. JAMA 289:1639–1644
Stey AM et al (2014) Hospital costs by cost center of inpatient hospitalization for medicare patients undergoing major abdominal surgery. J Am Coll Surg. doi:10.1016/j.jamcollsurg.2014.10.021
Woods MS (1996) Estimated costs of biliary tract complications in laparoscopic cholecystectomy based upon Medicare cost/charge ratios. A Case Control Study Surg Endosc 10:1004–1007
Phillips EH (1993) Routine versus selective intraoperative cholangiography. Am J Surg 165:505–507
Livingston EH, Miller JAG, Coan B, Rege RV (2007) Costs and utilization of intraoperative cholangiography. J Gastrointest Surg 11:1162–1167
Flum DR, Flowers C, Veenstra DL (2003) A cost-effectiveness analysis of intraoperative cholangiography in the prevention of bile duct injury during laparoscopic cholecystectomy. J Am Coll Surg 196:385–393
Shi H-Y, Lee K-T, Uen Y-H, Chiu C-C, Lee H-H (2010) Changing approaches to cholecystectomy in elderly patients: a 10-year retrospective study in Taiwan. World J Surg 34:2922–2931
Zacks SL, Sandler RS, Rutledge R, Brown RS (2002) A population-based cohort study comparing laparoscopic cholecystectomy and open cholecystectomy. Am J Gastroenterol 97:334–340
Chen SL, Comstock MC, Taheri PA (2003) The added cost of urgent cholecystectomy to health systems. J Am Coll Surg 197:16–21
Schwaitzberg SD et al (2014) Threefold increased bile duct injury rate is associated with less surgeon experience in an insurance claims database : more rigorous training in biliary surgery may be needed. Surg Endosc. doi:10.1007/s00464-014-3580-0
Shi H-Y, Lee K-T, Chiu C-C, Lee H-H (2013) The volume-outcome relationship in laparoscopic cholecystectomy: a population-based study using propensity score matching. Surg Endosc 27:3139–3145
Lee K-T, Chang W-T, Huang M-C, Chiu H-C (2004) Influence of surgeon volume on clinical and economic outcomes of laparoscopic cholecystectomy. Dig Surg 21:406–412
Harrison EM et al (2012) Hospital volume and patient outcomes after cholecystectomy in Scotland : retrospective, national. Br Med J 344:1–14
Sinha S et al (2013) Epidemiological study of provision of cholecystectomy in England from 2000 to 2009: retrospective analysis of hospital episode statistics. Surg Endosc 27:162–175
Trends in Health Care Cost Growth and the Role of the Affordable Care Act (2013) http://whitehouse.gov/sites/default/files/docs/healthcostreport_final_noembargo_v2.pdf
Margolis JM et al (2014) Health care utilization and expenditures among Medicaid beneficiaries with neuropathic pain following spinal cord injury. J Pain Res 7:379–387
Carmona M et al (2013) Heart failure in primary care: co-morbidity and utilization of health care resources. Fam Pract 30:520–524
D’Apuzzo MR, Novicoff WM, Browne JA (2015) The John Insall award: morbid obesity independently impacts complications, mortality, and resource use after TKA. Clin Orthop Relat Res 473:57–63
Shi H-Y et al (2014) Trends and outcome predictors after traumatic brain injury surgery: a nationwide population-based study in Taiwan. J Neurosurg 121:1323–1330
Genther DJ, Gourin CG (2014) Effect of comorbidity on short-term outcomes and cost of care after head and neck cancer surgery in the elderly. Head Neck. doi:10.1002/hed.23651
Vertrees JC, Averill RF, Eisenhandler J, Quain A, Switalski J (2013) Bundling Post-Acute Care Services into MS-DRG Payments. Medicare Medicaid Res Rev 3:1–19
Centers for Medicare and Medicaid Services (2014) Bundled payments for care improvement initiative fact sheet. http://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2014-Fact-sheets-items/2014-07-31.html
Hughes JS et al (2004) Clinical Risk Groups (CRGs): a classification system for risk-adjusted capitation-based payment and health care management. Med Care 42:81–90
Casale AS et al (2007) ‘ProvenCareSM’: a provider-driven pay-for-performance program for acute episodic cardiac surgical care. Ann Surg 246:613–621 (discussion 621–3)
Hoballah JJ, Liao J, Salameh M, Weigel RJ (2008) Physician reimbursement for general surgical procedures in the last century: 1906–2006. J Am Coll Surg 206:670–677
Frazee RC et al (2014) Can laparoscopic cholecystectomy be performed with a positive margin at medicaid reimbursement rates? J Am Coll Surg 218:546–551
Skolnik NS, Ryan DH (2014) Pathophysiology, epidemiology, and assessment of obesity in adults. J Fam Pract 63:S3–S10
Martin B-J, Chen G, Graham M, Quan H (2014) Coding of obesity in administrative hospital discharge abstract data: accuracy and impact for future research studies. BMC Health Serv Res 14:70
Januel J et al (2011) Improved accuracy of co-morbidity coding over time after the introduction of ICD-10 administrative data. BMC Health Serv Res 11:194
Patient Protection and Affordable Care Act. H.R. 3590(111) http://thomas.loc.gov/cgi-bin/query/z?c111:H.R.3590.pp
Rao A et al (2014) Safety of elective laparoscopic cholecystectomy in patients on dialysis: an analysis of the ACS NSQIP database. Surg Endosc Other Interv Tech 28:2208–2212
Funding information
This work was supported by an unrestricted Grant from Ethicon Endosurgery.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Jacqueline Boehme and Sophia McKinley have no conflict of interest or financial ties to disclose. Michael Brunt receives institutional research support from Gore and Karl Storz Endoscopy. Tina Hunter is a Senior Director for Biostatistics and Health Outcomes Research at CTI Clinical Trials and Consulting. Daniel Jones receives support from Allurion, Intuitive Surgical, Uptodate, CineMed, and Wolters. Daniel Scott, MD receives support from Ethicon, Covidien, Karl Storz, Accelerated Technologies, Inc., and NeatStitch, Inc. Steven Schwaitzberg, MD receives support from Acuity Bio (ownership interest as advisory committee), Cambridge Endo (ownership interest as advisory committee), Endocore (consulting fee as independent contractor), Human Extensions (honoraria as consultant), Neatstitch (ownership interest as advisory committee), Olympus (consulting fee as consultant), Stryker (consulting fee as consultant), and Surgiquest (ownership interest as advisory committee).
Appendices
Appendix 1
See Table 8.
Appendix 2
See Table 9.
Appendix 3
See Table 10.
Appendix 4
See Table 11.
Appendix 5
See Table 12.
Rights and permissions
About this article

Cite this article
Boehme, J., McKinley, S., Michael Brunt, L. et al. Patient comorbidities increase postoperative resource utilization after laparoscopic and open cholecystectomy. Surg Endosc 30, 2217–2230 (2016). https://doi.org/10.1007/s00464-015-4481-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-015-4481-6