
Abstract
Background
There is no established method for defining when a surgeon reaches the proficiency plateau in performing a specific operation. The published literature refers to “learning curves” based on retrospective evaluation of operative time, conversion rates, morbidity etc., which lack objectivity and do not address individual human factors. A more useful study of the gain in proficiency by the individual surgeon for a particular operation may be obtained using observational clinical-human reliability assessment (OCHRA).
Methods
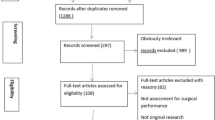
Following an 8-month fellowship in advanced laparoscopic surgery, the surgeon M.T. performed, independently at his own hospital, a prospective series of 20 palliative bypass operations for advanced gastric or pancreatic cancer. Unedited videotapes of gastro-jejunostomy (GJ) or cholecysto-jejunostomy (CJ) were analyzed independently in the training institution by the OCHRA technique.
Results
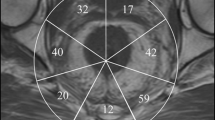
For this surgeon proficiency in executing laparoscopic palliative bypass was reached after the 14th anastomosis when efficient execution (reduction in operative time) was accompanied by significant reduction in technical errors and improved economy of movement (reduction of the economy of movement index from 7–5 to 3–2). The majority of errors were enacted in component tasks associated with intracorporeal suturing. The declining incidence of these errors with experience was an integral component of the proficiency-gain curve. The important performance-shaping factors identified were: concentration lapses (n = 1,321), misjudgments (n = 209), poor camera work (n = 193), fatigue (n = 128), and impaired coordination (n = 108).
Conclusions
This study has confirmed that OCHRA can describe quantitatively the proficiency-gain curve for a laparoscopic operation and indicate the plateau stage when the individual surgeon attains maximal performance in the execution of a specific procedure.



Similar content being viewed by others

References
Cuschieri A (2003) Lest we forget the surgeon. Sem Lap Surg 10:141–148
Cuschieri A (2006) Nature of human error: implications for surgical practice. Ann Surg 244:642–648
Kirwan B. Human reliability assessment. In: Wilson JR, Corlett EN (eds) Evalutaion of human work: a practical metodology, 2nd edn. Taylor & Francis, London, pp 921–968
Joice P, Hanna GB, Cuschieri A (1998) Errors during endoscopic surgery. A human reliability analysis. Appl Ergon 29:409–414
Tang B, Hanna GB, Joice P, Cuschieri A (2004) Identification and categorization of technical errors by observational clinical human reliability assessment (OCHRA) during laparoscopic cholecystectomy. Arch Surg 139:1215–1220
Reichenbach D, Tackett AD, Harris J, Diego C, Graviss EA, Dewan B, Vavra A, Stiles A, Fisher WE, Brunicardi FC, Sweeney JF (2006) Laparoscopic colon resection early on the learning curve. What is the appropriate setting? Ann Surg 243:730–737
O’Brien T, Tiptaft R, Glass J (2005) Defining the learning curves for percutaneous nephrolithotomy. J Urol 19:279–282
Bollens R, Sandhu S, Roumeguerre T, Quackela T, Shulman C (2005) Laparoscopic radical prostatectomy: the learning curve. Curr Opin Urol 15:79–92
Voitk AJ, Tsao SGS, Ignatius S (2001) The tail of the learning curve for laparoscopic cholecystectomy. Am J Surg 182:250–253
Archer SB, Brown DW, Smith D, Branum GD, Hunter JG (2001) Bile duct injury during laparoscopic cholecystectomy: results of a national survey. Ann Surg 234:549–559
Wruck D, Fleming I. Educational aspects of proficiency testing programs. http://www.caeal.ca/iad_PTCG(06)-17.pdf. Last accessed 15/03/07
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Talebpour, M., Alijani, A., Hanna, G.B. et al. Proficiency-gain curve for an advanced laparoscopic procedure defined by observation clinical human reliability assessment (OCHRA). Surg Endosc 23, 869–875 (2009). https://doi.org/10.1007/s00464-008-0088-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-008-0088-5