
Abstract
Purpose
We examined risk factors that may have contributed to Cytomegalovirus (CMV) reactivation among patients who underwent lung transplantation (LTx).
Methods
We reviewed medical records of patients who underwent LTx at a tertiary healthcare hospital in South Korea between January 2013 and May 2017. We excluded patients who died within the first year after LTx and those lost to follow-up. CMV reactivation was defined as the detection of CMV titers above 3000 copies/ml regardless of specific symptoms after prophylaxis cessation.
Results
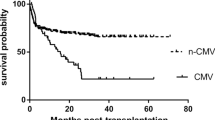
Of 89 patients included, 39 (43.8%) developed CMV reactivation. Of those 39 patients, 16 (41.0%) experienced additional CMV reactivation. Multivariate analysis identified lymphocyte counts below 1.0 × 103/μl (hazard ratio [HR] 49.33, p < 0.001) and use of steroids at more than twice the standard dose (HR 8.07, p < 0.001) as risk factors for CMV reactivation. The multivariate model also identified chronic kidney disease (CKD; HR 5.19, p = 0.016) and pneumonia (HR 17.22, p = 0.013) as risk factors for repetitive CMV reactivation.
Conclusion
This study suggests that lymphopenia and high doses of steroids may be important risk factors for CMV reactivation in LTx patients. Our results also suggest that repetitive CMV reactivation may be associated with CKD and pneumonia.





Similar content being viewed by others

Data Availability
Available on request.
References
Xue Y, Jiang L, Wan WG et al (2016) Cytomegalovirus pneumonia in patients with rheumatic diseases after immunosuppressive therapy: a single center study in China. Chin Med J (Engl) 129(3):267–273
Lumbreras C, Manuel O, Len O et al (2014) Cytomegalovirus infection in solid organ transplant recipients. Clin Microbiol Infect 20(Suppl 7):19–26
Bando K, Paradis IL, Komatsu K et al (1995) Analysis of time-dependent risks for infection, rejection, and death after pulmonary transplantation. J Thorac Cardiovasc Surg 109(1):49–57; (discussion 57–49)
Zamora MR, Davis RD, Leonard C (2005) Management of cytomegalovirus infection in lung transplant recipients: evidence-based recommendations. Transplantation 80(2):157–163
Zamora MR (2004) Cytomegalovirus and lung transplantation. Am J Transplant 4(8):1219–1226
Duncan SR, Paradis IL, Yousem SA et al (1992) Sequelae of cytomegalovirus pulmonary infections in lung allograft recipients. Am Rev Respir Dis 146(6):1419–1425
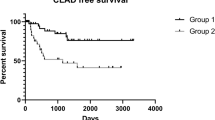
Estenne M, Maurer JR, Boehler A et al (2002) Bronchiolitis obliterans syndrome 2001: an update of the diagnostic criteria. J Heart Lung Transplant 21(3):297–310
Sharples LD, McNeil K, Stewart S et al (2002) Risk factors for bronchiolitis obliterans: a systematic review of recent publications. J Heart Lung Transplant 21(2):271–281
Tamm M, Aboyoun CL, Chhajed PN et al (2004) Treated cytomegalovirus pneumonia is not associated with bronchiolitis obliterans syndrome. Am J Respir Crit Care Med 170(10):1120–1123
Verleden SE, Vasilescu DM, Willems S et al (2014) The site and nature of airway obstruction after lung transplantation. Am J Respir Crit Care Med 189(3):292–300
Kotton CN, Kumar D, Caliendo AM et al (2018) The Third International consensus guidelines on the management of cytomegalovirus in solid-organ transplantation. Transplantation 102(6):900–931
Kotton CN, Kumar D, Caliendo AM et al (2013) Updated international consensus guidelines on the management of cytomegalovirus in solid-organ transplantation. Transplantation 96(4):333–360
Seo S, Cho Y, Park J (2009) Serologic screening of pregnant Korean women for primary human cytomegalovirus infection using IgG avidity test. Korean J Lab Med 29(6):557–562
Choi SR, Kim KR, Kim DS, Kang JM et al (2018) Changes in cytomegalovirus seroprevalence in Korea for 21 years: a single center study. Pediatr Infect Vaccine 25(3):123–131
Hibberd PL, Tolkoff-Rubin NE, Cosimi AB et al (1992) Symptomatic cytomegalovirus disease in the cytomegalovirus antibody seropositive renal transplant recipient treated with OKT3. Transplantation 53(1):68–72
Levin A, Stevens PE, Bilous RW et al (2013) Kidney Disease: improving global outcomes (KDIGO) CKD work group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 3(1):1–150
Fishman JA, Rubin RH (1998) Infection in organ-transplant recipients. N Engl J Med 338(24):1741–1751
Choi SR, Kim K-R, Kim DS et al (2018) Changes in cytomegalovirus seroprevalence in Korea for 21 years: a single center study. Pediatr Infect Vaccine 25(3):123–131
Schoeppler KE, Lyu DM, Grazia TJ et al (2013) Late-onset cytomegalovirus (CMV) in lung transplant recipients: can CMV serostatus guide the duration of prophylaxis? Am J Transplant 13(2):376–382
Takizawa Y, Inokuma S, Tanaka Y et al (2008) Clinical characteristics of cytomegalovirus infection in rheumatic diseases: multicentre survey in a large patient population. Rheumatology (Oxford) 47(9):1373–1378
Auphan N, DiDonato JA, Rosette C et al (1995) Immunosuppression by glucocorticoids: inhibition of NF-kappa B activity through induction of I kappa B synthesis. Science 270(5234):286–290
Girndt M, Sester U, Sester M et al (1999) Impaired cellular immune function in patients with end-stage renal failure. Nephrol Dial Transplant 14(12):2807–2810
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical Approval
The Institutional Review Board at Severance Hospital approved this study (IRB No.2013-0522-031).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kwak, S.H., Lee, S.H., Park, M.S. et al. Risk Factors for Cytomegalovirus Reactivation in Lung Transplant Recipients. Lung 198, 829–838 (2020). https://doi.org/10.1007/s00408-020-00380-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00408-020-00380-z