
Abstract
Background
Despite updated guidelines, management of thyroid nodules remains controversial. We aim to check implementation of new guidelines by ear–nose–throat (ENT) surgeons and endocrinologists.
Methods
A questionnaire was e-mailed including demographic data and an index case: a healthy 26-year-old women with a 3-cm Bethesda III (B3) atypia of undetermined significance solitary nodule and eventually papillary thyroid cancer (PTC).
Results
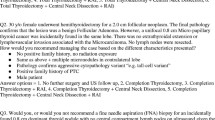
Respondent rate was 50.5%, 93 endocrinologists, 55 surgeons. For this case, 77.4% would repeat fine-needle aspiration (FNA), 25.3% order molecular analysis and 22.6% do surgery. If repeated FNA remained B3, 51% would choose surgery, 17.3% molecular analysis and 31.6% follow-up only. If repeated FNA was B6, 58.5% would recommend total (TTx) and 41.5% hemithyroidectomy (HTx). In pathologically confirmed PTC after HTx, 42.4% would recommend completion, 26.8% radioactive iodine (RAI) treatment. For a > = 4-cm tumor, 49.2% would recommend TTx. For a tumor 2–4 cm, 41% would recommend TTx. Variables favoring TTx were family history and radiation exposure. Only 17.4% would prefer TTx when small benign contralateral tumor is present. Reassessment at 1 year with undetectable thyroglobulin (Tg) included stimulated Tg (stTg) (72.5%), neck US only (27.5%) and combined US-stTg (59.4%); only 10.3% would order a diagnostic scan. For recurrence in two (13–9 mm) lymph nodes, 59.3% recommend reoperation, 16.3% RAI and 24.4% active surveillance. There were no major differences between endocrinologists and ENT surgeons.
Conclusions
We report a considerable lack of adherence to new guidelines, with only 50% recommending HTx for a 4-cm unifocal low-risk PTC tumor.

Similar content being viewed by others


References
Haugen BR, Alexander EK, Bible KC et al (2016) 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 26(1):1–133
Nabhan F, Ringel MD (2017) Thyroid nodules and cancer management guidelines: comparisons and controversies. Endocr Relat Cancer 24(2):R13–R26
Negro R, Attanasio R, Grimaldi F et al (2017) A 2016 Italian survey about guidelines and clinical management of thyroid nodules. Eur Thyroid J 6(2):75–81
Goichot B, Bouée S, Castello-Bridoux C et al (2017) Survey of clinical practice patterns in the management of 992 hyperthyroid patients in France. Eur Thyroid J 6(3):152–159
Burch HB, Burman KD, Cooper DS et al (2016) A 2015 survey of clinical practice patterns in the management of thyroid nodules. J Clin Endocrinol Metabolism 101(7):2853–2862
Brito JP, Castro MR, Dean DS et al (2015) Survey of current approaches to non-diagnostic fine-needle aspiration from solid thyroid nodules. Endocrine 49(3):745–751
Bernet V, Hupart K, Parangi S et al (2014 Apr) AACE/ACE disease state commentary: molecular diagnostic testing of thyroid nodules with indeterminate cytopathology. Endocr Pract 20(4):360–363
Cibas ES, Ali SZ (2009) The Bethesda system for reporting thyroid cytopathology. Am J Clin Pathol 132(5):658–665
Cibas ES, Baloch ZW, Fellegara G (2013) e al. A prospective assessment defining the limitations of thyroid nodule pathologic evaluation. Ann Intern Med 159(5):325–332
Matsuzu K, Sugino K, Masudo K et al (2014) Thyroid lobectomy for papillary thyroid cancer: long-term follow-up study of 1,088 cases. World J Surg 38(1):68
Barney BM, Hitchcock YJ, Sharma P et al (2011) Overall and cause specific survival for patients undergoing lobectomy, near total, or total thyroidectomy for differentiated thyroid cancer. Head neck 33(5):645–649
Mendelsohn AH, Elashoff DA, Abemayor E et al (2010) Surgery for papillary thyroid carcinoma: is lobectomy enough? Arch Otolaryngol Head Neck Surg 136(11):1055–1061
Haigh PI, Urbach DR, Rotstein LE (2005) Extent of thyroidectomy is not a major determinant of survival in low-or high-risk papillary thyroid cancer. Ann Surg Oncol 12(1):81–89
Nixon IJ, Ganly I, Patel SG et al (2012) Thyroid lobectomy for treatment of well differentiated intrathyroid malignancy. Surgery 151(4):571–579
Vaisman F, Shaha A, Fish S et al (2011) Initial therapy with either thyroid lobectomy or total thyroidectomy without radioactive iodine remnant ablation is associated with very low rates of structural disease recurrence in properly selected patients with differentiated thyroid cancer. Clin Endocrinol (Oxf) 75(1):112–119
Cooper DS, Doherty GM, Haugen BR et al (2009) Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association (ATA) guidelines taskforce on thyroid nodules and differentiated thyroid cancer. Thyroid 19(11):1167–1214
Mazeh H, Benavidez J, Poehls JL et al (2012) In patients with thyroid cancer of follicular cell origin, a family history of nonmedullary thyroid cancer in one first-degree relative is associated with more aggressive disease. Thyroid 22(1):3–8
Robenshtok E, Tzvetov G, Grozinsky-Glasberg S et al (2011) Clinical characteristics and outcome of familial nonmedullary thyroid cancer: a retrospective controlled study. Thyroid 21(1):43–48
Nixon IJ, Suárez C, Simo R et al (2016) The impact of family history on non-medullary thyroid cancer. Eur J Surg Oncol 42(10):1455–1463
Tuttle RM, Tala H, Shah J et al (2010) Estimating risk of recurrence in differentiated thyroid cancer after total thyroidectomy and radioactive iodine remnant ablation: using response to therapy variables to modify the initial risk estimates predicted by the new American Thyroid Association staging system. Thyroid 20(12):1341–1349
Mazzaferri EL, Robbins RJ, Spencer CA et al (2003) A consensus report of the role of serum thyroglobulin as a monitoring method for low-risk patients with papillary thyroid carcinoma. J Clin Endocrinol Metab 88(4):1433–1441
Phan HT, Jager PL, Van der Wal JE et al (2008) The follow-up of patients with differentiated thyroid cancer and undetectable thyroglobulin (Tg) and Tg antibodies during ablation. Eur J Endocrinol 158(1):77–83
Robenshtok E, Fish S, Bach A et al (2012) Suspicious cervical lymph nodes detected after thyroidectomy for papillary thyroid cancer usually remain stable over years in properly selected patients. J Clin Endocrinol Metab 97(8):2706–2713
Rondeau G, Fish S, Hann LE et al (2011) Ultrasonographically detected small thyroid bed nodules identified after total thyroidectomy for differentiated thyroid cancer seldom show clinically significant structural progression. Thyroid 21(8):845–853
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Or, K., Benbassat, C., Koren, S. et al. Adherence to ATA 2015 guidelines in the management of unifocal non-invasive papillary thyroid cancer: a clinical survey among endocrinologists and surgeons. Eur Arch Otorhinolaryngol 275, 2851–2859 (2018). https://doi.org/10.1007/s00405-018-5126-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-018-5126-x