
Abstract
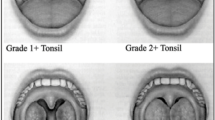
Unrelieved upper airway obstruction from highly prevalent adenotonsillar hypertrophy (ATH) has the potential of producing structural remodelling of the pulmonary vascular bed with resultant pulmonary hypertension (PH) and cor pulmonale. This cross-sectional study aimed to determine the local prevalence of PH and examine its clinical and radiological pointers among children with ATH. The airway obstruction was evaluated clinically by grading the nocturnal and daytime symptoms of ATH. A Brodsky scale and adenoid–nasopharynx ratio (AN ratio) were used to categorize tonsil and adenoid size, respectively. Mean pulmonary artery pressure (mPAP), was measured noninvasively for each child using Doppler echocardiography and PH was defined by mPAP ≥25 mmHg. Comparison of symptom scores, tonsil and adenoid size and demographic factors was made between children with mPAP ≥25 mmHg and those mPAP <25 mmHg using univariate and multivariate analysis. There was 22.8 % (18/79) prevalence of PH among the 26 children with only adenoid hypertrophy and 53 with ATH. Significant risk factors identified by logistic regression analysis associated with PH were daytime mouth breathing, daytime stertor, and AN ratio >0.75 (P = 0.002, 0.018, and 0.04, respectively), with more than sixfold and fourfold increase risk for daytime mouth breathing and daytime stertor, respectively. Obstructive breathing during sleep was significant only on univariate analysis. Prolonged symptom duration ≥24 months, large tonsils (grades 3 and 4), snoring and mouth breathing during sleep were not significant. This study demonstrated that pulmonary hypertension remains prevalent in children with ATH. Daytime mouth breathing and stertor as well as AN ratio >0.75 are the prime predictors of pulmonary hypertension, with an AN ratio cut-off point of 0.73 on ROC analysis.

Similar content being viewed by others


References
Lee P, Hwang B, Soong W, Meng CL (2013) The specific characteristics in children with obstructive sleep apnea and cor pulmonale. Sci World J 2012:1–6. doi:10.1100/2012/757283
Chang S, Chae K (2010) Obstructive sleep apnea syndrome in children: epidemiology, pathophysiology, diagnosis and sequelae. Korean J Pediatr 53:863–871
Durmowicz A, Stenmark K (1999) Mechanisms of structural remodelling in chronic pulmonary hypertension. Pediatr Rev 20:91–102
Tatlipinar A, Duman D, Uslu C et al (2011) The effects of obstructive sleep apnea syndrome due to adenotonsillar hypertrophy on the cardiovascular system in children. Turk J Pediatr 53:359–363
Miman MC, Kirazli T, Ozyurek R (2000) Doppler echocardiography in adenotonsillar hypertrophy. Int J Pediatr Otorhinolaryngol 54:21–26
Marangu D, Jowi C, Aswani J et al (2014) Prevalence and associated factors of pulmonary hypertension in Kenyan children with adenoid or adenotonsillar hypertrophy. Int J Pediatr Otorhinolaryngol 78:1381–1386
O’Driscoll DM, Foster AM, Ng MI et al (2009) Acute cardiovascular changes with obstructive events in children with sleep disordered breathing. Sleep 32:1265–1271
Kumar EB, Jaggarao NSV (1989) Adenotonsillar hypertrophy and cor pulmonale: clinical and echocardiographic correlation. Postgrad Med J 65:473–475
Sie KC, Perkins JA, Clarke WR (1997) Acute right heart failure due to adenotonsillar hypertrophy. Int J Pediatr Otorhinolaryngol 41:53–58
Orji FT, Ezeanolue BC (2008) Evaluation of adenoidal obstruction in children: clinical symptoms compared with roentgenographic assessment. J Laryngol Otol 122:1201–1205
Brodsky L (1989) Modern assessment of tonsils and adenoids. Pediatr Clin North Am 36:1551–1569
Fujioka M, Young LW, Girdany BR (1979) Radiographic evaluation of adenoidal size in children: adenoidal—nasopharyngeal ratio. Am J Radiol 133:401–404
Tatlipinar A, Biteker M, Meric K et al (2012) Adenotonsillar hypertrophy: correlation between obstruction types and cardiopulmonary complications. Laryngoscope 122:676–680
Colman R, Whittingham H, Tomlinson G et al (2014) Utility of the physical examination in detecting pulmonary hypertension. A mixed methods study. PLoS One 9(10):e108499. doi:10.1371/journal.pone.0108499
Sofer S, Weinhouse E, Tal A et al (1988) Cor pulmonale due to adenoidal or tonsillar hypertrophy in children. Noninvasive Diagn Follow Chest 93(1):119–122
Abdel-Aziz M (2011) Asymptomatic cardiopulmonary changes caused by adenoid hypertrophy. J Craniofac Surg 22:1401–1403
Yilmaz MD, Onrat E, Altuntaş A et al (2005) The effects of tonsillectomy and adenoidectomy on pulmonary arterial pressure in children. Am J Otolaryngol 26:18–21
Luke MJ, Mehrizi A, Folger GM et al (1966) Chronic nasopharyngeal obstruction as a cause of cardiomegaly, cor pulmonale and pulmonary edema. Pediatrics 37:762–768
Brown OE, Manning SC, Ridenour B (1988) Cor-pulmonale secondary to tonsillar and adenoid hypertrophy: management consideration. Int J Pediatr Otorhinolaryngol 16:131–139
Fasunla AJ, Onakoya PA, Ogunkunle OO et al (2011) Routine electrocardiography request in adenoidectomy: is it necessary? Indian J Otolaryngol Head Neck Surg 63:330–335
Muzumdar H, Arens R (2008) Diagnostic issues in pediatric obstructive sleep apnea. Proc Am Thorac Soc 5:263–273
Granzotto E, Aquino F, Flores J et al (2010) Tonsil size as a predictor of cardiac complications in children with sleep-disordered breathing. Laryngoscope 120(6):1246–1251
Bitar MA, Rahi A, Khalifeh M, Madanat LS (2006) A suggested clinical score to predict the severity of adenoidal obstruction in children. Eur Arch Otorhinolaryngol 263:924–928
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None declared.
Informed consent was obtained from all individual participants included in the study.
This article does not contain any studies with animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Orji, F.T., Adiele, D.K., Umedum, N.G. et al. The clinical and radiological predictors of pulmonary hypertension in children with adenotonsillar hypertrophy. Eur Arch Otorhinolaryngol 274, 1237–1243 (2017). https://doi.org/10.1007/s00405-016-4207-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-016-4207-y