
Abstract
We compared the use of glycerol and icthammol (G&I) ribbon gauze versus topical antibiotic and steroid drops in the management of otitis externa. Patients presenting with acute otitis externa were systematically recruited from attendance in the ENT emergency clinic. Exclusion criteria were age <18 years, diabetic patients, and those who had been previously treated for otitis externa by the department within the last month. A total of 43 patients were recruited with 48 infected ears, the mean patient age was 47 years, (range 18–80 years). Patients were randomised to either insertion of a G&I ribbon gauze or topical ear drops by means of a ballot with no stratification. All patients were reviewed 5 days later. Patients were asked to comment on their pain using the ten point visual analogue pain score. Oedema of the canal wall, presence of debris and visibility of the tympanic membrane were graded on microscopy. Patient satisfaction and return to work were assessed. There was a statistically significant decrease in the pain score between each visit for the entire group of patients and decrease in canal wall swelling (P < 0.001). There was no significant difference between drops and ribbon gauze in terms of pain relief, canal wall oedema, or aural discharge. Following microbiological analysis, 27.8% of bacteria were resistant to neomycin. The cost of treatment with G&I is less than a third of that for topical antibiotic–steroid drops and requires less patient compliance. Patient concerns with the ribbon gauze included its cosmetic appearance and loss of hearing and with drops included frequency of application. We recommend the use of G&I ribbon gauze as first-line treatment, particularly for those who have had allergies to carriers of drops, those that are poorly compliant or with poor manual dexterity, for example patients with rheumatic hands.
Similar content being viewed by others


Introduction
Otitis externa is one of the most common diagnoses made after referral to an acute otolaryngology service [1]. Acute otitis externa is characterised by otalgia, otorrhoea, conductive hearing loss and the presence of exudate in an oedematous ear canal. Historically, many factors have been suggested as predisposing factors, however, only swimming has been proven to increase the risk [2]. Common pathogens implicated in acute otitis externa include Pseudomonas aeruginosa (50%), Staphylococcus aureus (23%), anaerobes and gram-negative organisms (12.5%) and yeasts (12.5%) [3].
Since its first description, a variety of methods have been proposed for the management of otitis externa. Perhaps, one of the earliest forms of management was that of ear candling [4]. Topical medications, including astringents and alcohols have been used in otitis externa for many years. Topical antibiotics are now widely used for first-line management of acute otitis externa and are most often administered in combination with topical steroids.
When the external auditory meatus is so oedematous that the passage of topical medication is impossible, the canal may be stented open by the use of a wick or ribbon gauze. Commercially produced ear wicks, such as the Pope wick are expensive and can cost several pounds; they generally require removal after 2–3 days. Ribbon gauze by comparison is cheap, costing less than 50 p a roll, and may easily be removed without the use of specialist equipment or a microscope. A trial comparing resolution rates between otitis externa managed using wicks versus ribbon gauze revealed no significant difference [5].
The senior author has a great deal of experience using G&I coated ribbon gauze in the treatment of otitis externa and this management option is readily available within our outpatient department. Both icthammol and glycerol have therapeutic actions.
To our knowledge there has been no previous study comparing G&I with the more standard treatment of topical antibiotic ear drops. A literature search of the Ovid Medline database from 1950 to February 2007 using search terms glycerine, glycerol, icthammol, otitis and externa, revealed ono clinical trial of G&I.
Materials and methods
Local ethical approval was obtained prior to the commencement of this trial. Patients presenting with acute otitis externa were systematically recruited from attendance in the ENT emergency clinic by clinic doctors over a 3 month period. A diagnosis of otitis externa was made if the patient was symptomatic: describing otorrhoea, otalgia and hearing loss, and had signs of external auditory meatus inflammation or exudate. Exclusion criteria were age <18 years, diabetic patients, and those who had been previously treated for otitis externa by the department within the last month. Patients who had a history of skin allergy or signs of generalised skin disease prior to development of super-infection of the external auditory meatus were not included in the trial. Informed consent for inclusion in the trial was taken. Patients were asked to comment on their pain at presentation using the standard ten point visual analogue pain score.
Microscopic examination of the ear canal was performed in all cases and presence of debris, visibility of the tympanic membrane and tympanic membrane perforation was noted. Oedema of the canal wall was graded on a scale of 0–2, no oedema was graded 0, canal wall oedema without total obstruction was graded as 1, and total obstruction was graded as 2. Swabs were obtained for microscopy and microsuction performed in cases where debris was visible.
Patients were randomised to either insertion of a G&I coated ribbon gauze or topical ear drops by means of a ballot with no stratification. Patients randomised to receive topical drops were prescribed the local pharmacy recommended first-line treatment—Vista-methasone N (betamethasone sodium phosphate 0.1%, neomycin sulphate 0.5%) two drops three times a day. They were given a patient leaflet instructing the use of ear drops and were advised to take water precautions. Patients randomised to receive a G&I had a 25 cm length of ribbon gauze coated in 10 ml of 10% icthammol in glycerol inserted into the external auditory canal. The ribbon gauze was introduced into the canal via a speculum under microscopic observation. If the canal was very oedematous, the ribbon gauze was gently passed through the obstruction with crocodile forceps. All patients were reviewed by the same doctor 5 days later and the observations repeated. Patients were also asked to comment on any problems with their form of treatment. If the condition persisted at the second visit, the treatment was changed to antibiotic drops based on microbiology results and the patient followed up until the condition resolved.
Results
A total of 43 patients were recruited with 48 infected ears. The mean patient age was 47 years (range 18–80 years). The right ear was involved in 23 cases and the left in 25. This presentation was the first episode of otitis externa for 23 patients (53.5%). The length of symptoms before referral had a range of 2–49 days, with a median of 7 days. Two patients had tympanic membrane perforations, both of which were randomised to receive drops. Twenty-seven patients were randomised to receive drops and 21 to receive a ribbon gauze. The five patients with both ears infected received a ribbon gauze on a randomised side and drops on the other. One patient in the ribbon gauze group did not return for follow-up, on enquiry it appeared the ribbon gauze had been removed by the patient.
Following microbiological analysis, 26 patients swabs grew P. aeruginosa, 6 coliform species, 4 S. aureus, 2 Aspergillus nigrans and 10 had no growth.
The results were analysed using Wilcoxon Signed Ranks Tests. The study sample size of 47 (27 vs. 20) was sufficient to detect a difference between treatment of 0.75 standard deviations with 80% power and a level of significance of 0.05.
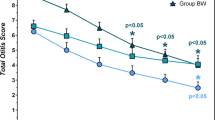
There was a statistically significant decrease in the pain score between each visit for the entire group of patients (Fig. 1), with mean pain scores (scale of 0–10, 10 most severe) at first visit 5.6 (SD 3.1) decreasing to 2.3 (SD 2.7) at second visit (P < 0.001). There was also a statistically significant decrease in oedema and obstruction of the auditory canal (Fig. 2, scale of 0–2, 2 most swelling) with mean score on first visit 0.9 (SD 0.7) and second visit 0.2 (SD 0.4) P < 0.001. Of all patients 90% required microsuction on their first visit and 50% on their second visit. It was impossible to visualise the tympanic membrane in 34 patients on first attendance due to both canal wall swelling and the presence of debris on the tympanic membrane (72.3%, 0.72, SD 0.5), this fell to 11 (23.4%, 0.23, SD 0.4) on second visit (P < 0.001). There was no significant change in the percentage of patients with otorrhoea or aural debris between visits (Fig. 3), 70% had discharge on the first visit (0.7, SD 0.5), compared with 60% (0.6, SD 0.5) on the second visit (P = 0.166). Fourteen (27.7%) of the patients had complete resolution at their second clinic appointment and did not require a further appointment, 9 from the group randomised to drops and 5 to ribbon gauze. Of the remaining 29 patients, 22 had resolution of the condition by the third visit and all by the fourth visit.

There was a statistically significant drop in the pain score between the two visits for both treatment groups, but there was no difference between groups

There was a statistically significant decrease in canal wall oedema between the two visits for both treatment groups, but there was no difference between groups

There was no statistically significant difference in discharge between the two visits for both treatment groups, or between groups
There was no statistical difference between the treatment groups for the change in all variables between the two clinic attendances.
Discussion
Our study comparing the use of antibiotic and steroid ear drops with a G&I ribbon gauze to treat otitis externa appeared to show that both treatments were effective in reducing pain and canal wall swelling, but there was no significant difference in any variables between the two forms of treatment. Topical antibiotics are now widely used for first-line management of acute otitis externa. Studies have shown that there is no significant difference in clinical efficacy between a topical antibiotic (gentamicin sulphate) and a topical antiseptic (aluminium acetate) for the initial treatment of otorrhoea [6]. This would concur with the findings of our study.
Icthammol is a product of bituminous shale, containing ammonium salts of sulphonic acid [7]. Icthammol is a black viscous substance that can be used in a variety of preparations such as creams, ointments and as a solution with glycerol. Icthammol has been used for its anti-inflammatory properties in a number of dermatological conditions, such as eczema and psoriasis [8]. Icthammol has been shown to have anti-bacterial activity against gram-positive organisms (S. aureus and Streptococcus pyogenes) [7, 9]. Icthammol also has an anti-inflammatory action, reducing secretion of chemotactic metabolites from leucocytes [10] and inhibiting macrophage migration [11]. Glycerol is hygroscopic and therefore has a dehydrating action on inflamed tissue [12]. It has not been shown to have any active antimicrobial effect [7, 8].
Our study revealed that 55.3% of cases had P. aeruginosa, 8.5% had S. aureus, 12.8% coliforms and 4.3% fungal species. These results would concur with those quoted in the literature [3]. It is likely that the failure of resolution of the condition by the second visit was due to the resistance of the bacteria to the treatment given. As previously mentioned, icthammol has limited effects on gram-negative bacteria, although there was complete resolution in two patients with Pseudomonas treated with G&I. There was a degree of resistance to neomycin within the cultured bacteria, with 10 patients of the 36 cultures being positive for bacterial growth with neomycin-resistant bacteria on culture. Nine of these patients did not have resolution of symptoms on the second visit. This does bring into question the choice of primary treatment. Neomycin was chosen as our antibiotic as it is our Microbiology Department’s guidance for first-line treatment for otitis externa based on local drug resistance. Our results indicate that these guidelines should be reassessed.
When choosing between the two forms of treatment, it is necessary to take many factors into account. Cost effectiveness is one important issue, each application of G&I ribbon gauze costs approximately 50 p, the current listed price for 10 ml of Vista-methasone N is £1.29. Another factor is antibiotic resistance. As G&I has a local effect on pH and osmolality in addition to a bactericidal effect, it is also unlikely to develop resistance, although further investigation is necessary.
The correct application of topical drops for otitis externa is important. Applying the drops three times a day is inconvenient, particularly for those working, and method of application varies. A study comparing the compliance between different topical antibiotic delivery systems showed a trend to overdose with dropper style bottles compared to spray delivery systems [13]. Application of topical ear drops does involve some degree of manual dexterity, coordination and flexibility. For the elderly or infirm with nobody to assist in the application of drops, compliance is likely to be poor. Compliance of treatment with ribbon gauze in situ is likely to be much higher as there is no need for any active intervention by the patient. The main limiting factor for the use of the ribbon gauze is that of patient satisfaction and inconvenience. Patients commented that they felt the gauze was unsightly and hearing in that ear remained poor for the 5 days of use. However, other patients liked the fact that they did not need to worry about remembering to apply the drops or interrupting their normal activities. Patients were questioned about discomfort of having the ribbon gauze inserted; none felt that it was significantly uncomfortable. Patients do need to return to the clinic to remove the gauze, necessitating two visits. It may be that patients receiving drops only require one visit and need to return only if they have a poor response to initial management. This is not currently our department policy, but could possibly be introduced with the emerging role of general practitioners with specialist interests (GPSI).
There are sources of potential error in this study. Due to the nature of the treatment, it was impossible to blind the patient or the investigator. It is clear to the patient whether they have a ribbon gauze inserted or need to apply drops. The investigator knows which treatment was used as even if the gauze was removed prior to assessment, the G&I solution leaves a visible coating on the external canal impossible to disguise. This may have led to bias in the objective measurement of canal wall oedema, although this was minimised by the use of well-defined assessment criteria.
Conclusion
Within our randomised trial of G&I ribbon gauze versus topical antibiotic drops, there was no significant difference in terms of pain relief, canal wall oedema, or aural discharge. We therefore recommend the use of G&I wicks as first-line treatment in all cases of otitis externa but especially in those allergic to carriers of drops, poorly compliant or have poor manual dexterity, for example patients with rheumatic hands. This treatment could be discussed with other patients in clinic and the option offered to avoid the regular insertion of topical medication.
References
Rowlands S, Devalia H, Smith C, Hubbard R, Dean A (2001) Otitis externa in UK general practice: a survey using the UK General Practice Research Database. Br J Gen Pract 51:533–538
Springer GL, Shapiro ED (1985) Fresh water swimming as a risk factor for otitis externa: a case controlled study. Arch Environ Health 40:202–206
Holten KB, Gick J (2001) Management of the patient with otitis externa. J Fam Pract 50(4):353–360 357–358
Seely DR, Quigley SM, Langman AW (1996) Ear candles: efficacy and safety. Laryngoscope 106:1226–1229
Pond F, McCarty D, O’Leary S (2002) Randomized trial on the treatment of oedematous acute otitis externa using ear wicks or ribbon gauze: clinical outcome and cost. J Laryngol Otol 116(6):415–419
Clayton MI, Osborne JE, Rutherford D, Rivron RP (1990) A double-blind, randomised, prospective trial of a topical antiseptic versus a topical antibiotic in the treatment of otorrhoea. Clin Otolaryngol 15(1):7–10
Nilssen E, Wormald PJ, Oliver S (1996) Glycerol and icthammol: medicinal solution or mythical potion? J Laryngol Otol 110:319–321
Millatd LG (1984) Eczema and psoriasis: what are the non-steroid alternatives? Dermatol Pract 3:23–27
Ahmed K, Roberts ML, Mannion PT (1995) Antimicrobial activity of glycerine-icthammol in otitis externa. Clin Otolaryngol 20:201–203
Williamson DS. Topical therapy (1979) In: Rook A, Williamson DS, Ebling FJG (Eds) Textbook of dermatology. Blackwell, Oxford, pp 2293–2328
Takeuchi K, Ito K, Namikawa S (1988) Anti-inflammatort activity of the dry distillation tar or delipidated soybean. Nippon Yakurigaku Zasshi 91(1):1–7
Reynolds JEF (1989) Martindale—the extra pharmacopoeia, 29th edn. The Pharmaceutical Press, London, pp. 1128–1129
Lancaster J, Matthews J, Williams RS, Thussey C, Kent SE (2003) Comparison between topical aural medications. Clin Otolaryngol 28(4):331–334
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hornigold, R., Gillett, D., Kiverniti, E. et al. The management of otitis externa: a randomised controlled trial of a glycerol and icthammol ribbon gauze versus topical antibiotic and steroid drops. Eur Arch Otorhinolaryngol 265, 1199–1203 (2008). https://doi.org/10.1007/s00405-008-0620-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-008-0620-1