
Summary
Surgical therapy of native infective endocarditis is still considered as a particular challenge, due to remaining morbidity and mortality up to 20%. Further risk analysis and characterization of clinical features is of great importance for further improvement of surgical results. The aim of this retrospective study was a risk analysis concerning clinical features of the pre–, intra– and postoperative period.
Between 02/1997 and 12/2003, 165 patients (130 male, 35 female, age 55.5 ± 13.8 years) were referred for surgical therapy of infective endocarditis at our institution. Preoperative, intraoperative and postoperative features were evaluated for their influence on the early postoperative course and the mid–term follow–up. In the majority of patients (pts) the aortic valve was infected (n = 83, 50.3% of pts), followed by mitral valve (n = 33; 20.0%), tricuspid valve (n = 10, 6.0%) and pulmonary valve (n = 2; 1.2%). Double valve affection was recorded in 37 pts (22.4%). Streptococci (n = 66, 40.0%) and staphylococci (n = 66, 40.0%) were the most common pathogens. The overall hospital mortality rate was 10.9% (n = 18), during follow–up (mean follow–up 3.3 ± 2.5 years) a further 20 pts (12.1%) died.
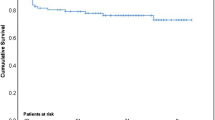
Main predictors for hospital mortality in multivariate analysis were older age (p = 0.01), prolonged ICU stay, prolonged intubation (p = 0.03; p = 0.02) and the continuous postoperative need of alpha–catecholamine medication (p < 0.01). Significant predictors of overall mortality were older age (> 70 years) and diabetes (p = 0.03; p = 0.03). Reinfection occurred in 6.1% of patients (n = 10). Actuarial freedom from recurrent infection was 97% at 1 year and 93.9% at 5 years. Surgical therapy of infective endocarditis is associated with good clinical results in the early and mid–term follow–up. Predictors of outcome particular include preoperative risk constellation or comorbidity (age, diabetes) and variables of the immediate postoperative course.
Similar content being viewed by others


References
Alexiou C, Langley SM, Stafford H et al (2000) Surgery for active culturepositive endocarditis: determinants of early and late outcome. Ann Thorac Surg 69:1448–1454
Bauernschmitt R, Jakob HG, Vahl C et al (1998) Operation for infective endocarditis: results after implantation of mechanical valves. Ann Thorac Surg 65:359–364
Chan KL (2002) Early clinical course and long–term outcome of patients with infective endocarditis complicated by perivalvular abscess. CMAJ 167:19–24
Chu VH, Cabell C, Benjamin DK et al (2004) Early predictors of in–hospital death in infective endocarditis. Circulation 199:1745–1749
Delay D, Pellerin M, Carrier M et al (2000) Immediate and long–term results of valve replacement for native and prosthetic valve endocarditis. Ann Thorac Surg 70:1219–1223
D'Udekem Y, David TE, Feindel CE et al (1997) Long–term results of surgery for infective endocarditis. Eur J Cardiothoracic Surg 11:46–52
Durack DT, Lukes AS, Bright DK (1994) New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. Duke Endocarditis Service. Am J Med 96:200–209
Greten T, von Hoch F, Enker J, von Hodenberg E (2001) Bakterielle Endokarditisprophylaxe. Z Kardiol 90 (Suppl 6):22–26
Grünenfelder J, Akins CW, Hilgenberg AD et al (2001) Long–term results and determinants of mortality after surgery for native and prosthetic valve endocarditis. J Heart Valve Dis 10:694–702
Hart RG, Forster JW, Luther MF et al (1990) Stroke in infective endocarditis. Stroke 21:695–700
Hasburn R, Vikram HR, Barakat LA et al (2003) Complicated left–sided native valve endocarditis in adults: risk classification for mortality. JAMA 289:1933–1940
Hoen B, Selton–Suty C et al (2002) Changing profile of infective endocarditis: results of a 1–year survey in France. JAMA 288:75–81
Horstkotte D (2000) Endocarditis: epidemiology, diagnosis and treatment. Z Kardiol 89(Suppl 4):2–11
Jault F, Gandjbakh I, Ram A et al (1997) Active native valve endocarditis: determinants of operative deaths and late mortality. Ann Thorac Surg 63:1737–1741
Mihaljevic T, Byrne JG, Cohn LH et al (2001) Long–term results of multivalve surgery for infective multivalve endocarditis. Eur J Cardiothoracic Surg 20:842–846
Mullany CJ, Chua YL, Schaff HV et al (1995) Early and late outcome after surgical treatment of culture–positive active endocarditis. Mayo Clin Proc 70:517–525
Netzer RO, Zollinger E, Seiler C et al (2000) Infective endocarditis: clinical spectrum, presentation and outcome: an analysis of 212 cases 1980–1995. Heart 84:25–30
Romano G, Carozza A, Della Corte A et al (2004) Native versus primary prosthetic valve endocarditis: comparison of clinical features and longterm outcome in 353 patients. J Heart Valve Dis 13:200–209
Task force on infective endocarditis of the European Society of Cardiology (2004) Guidelines on prevention, diagnosis and treatment of infective endocarditis. Eur Heart J 00:1–37
Tingleff J, Egeblad H, Gotzsche CO et al (1995) Perivalvular cavities in endocarditis: abscesses versus pseudoaneurysms? a transesophageal doppler echocardiographic study in 118 pts with endocarditis. Am Heart J 130:93–100
Vilacosta I, Graupner C, San Roman JA et al (2002) Risk of embolization after institution of antibiotic therapy of infective endocarditis. J Am Coll Cardiol 39:1489–1495
Vogt PR, Brunner–LaRocca HP (2001) Langzeitresultate der chirurgischen Behandlung der akuten Aortenklappenendokarditis. Z Kardiol 90(Suppl 6):27–34
Voss F, Bludau HB, Weretka S, Haller C (2000) Mitral valve endocarditis: an uncommon cause of myocardial infarction. Z Kardiol 92:686–688
Wallace SM, Walton BI, Kharbanda RK et al (2002) Mortality from infective endocarditis: clinical predictors of outcome. Heart 88:53–60
Werner D, Schellong S, Weise M et al (2000) Transösophageale Darstellung einer Koronarfistel bei gleichzeitiger Endocarditis lenta. Z Kardiol 88:229–232
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tugtekin, S.M., Alexiou, K., Wilbring, M. et al. Native infective endocarditis: Which determinants of outcome remain after surgical treatment?. Clin Res Cardiol 95, 72–79 (2006). https://doi.org/10.1007/s00392-006-0326-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-006-0326-6