
Abstract
Purpose
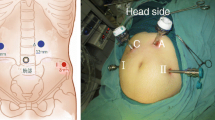
A robotic system was mainly designed to allow precise dissection in deep and narrow spaces. We report the clinical and oncologic outcomes of totally robotic total mesorectal excision for rectal cancer.
Methods
Between July 2009 and January 2012, 60 consecutive patients undergoing robotic surgery for rectal cancer at the Eulji University Hospital were included.
Results
The mean total operation time, docking time, and surgeon console time were 466.8 ± 115.6, 7.5 ± 6.7, and 261 ± 87.5 min, respectively. Oral intake of diet was started at 3.3 ± 0.9 days and the mean hospital stay was 8.6 ± 2.4 days. All 60 procedures were technically successful without the need for conversion to open or laparoscopic surgery. Complications included anastomotic leakage, anastomotic stricture, postoperative bleeding, ileus, and perineal wound infection in 3 (5 %), 1 (1.7 %), 2 (3.3 %), 2 (3.3 %), and 1 (1.7 %) patient, respectively. The mean distal resection margin and total number of lymph nodes harvested was 3.1 ± 1.7 cm and 20.1 ± 11.5, respectively. During the mean follow-up period of 48.5 months (range, 7–75), the 4-year overall and disease-free survival rates were 87.7 and 72.8 %, respectively.
Conclusions
A totally robotic approach for rectal cancer operations was a time-consuming procedure, although we already had a lot experience in laparoscopic colorectal surgery. However, the dexterity of the robotic surgery could enable the surgeon to expand the choice of surgical methods according to the condition of the rectal cancer without the need for conversion.





Similar content being viewed by others

References
Jayne DG, Guillou PJ, Thorpe H, Quirke P, Copeland J, Smith AM, Heath RM, Brown JM, Group UMCT (2007) Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC Trial Group. J Clin Oncol 25(21):3061–3068
Kang SB, Park JW, Jeong SY et al (2010) Open versus laparoscopic surgery for mid or low rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): short-term outcomes of an open-label randomised controlled trial. Lancet Oncol 11(7):637–645
van der Pas MH, Haglind E, Cuesta MA, Furst A, Lacy AM, Hop WC, Bonjer HJ, COlorectal cancer Laparoscopic or Open Resection II (COLOR II) Study Group (2013) Laparoscopic versus open surgery for rectal cancer (COLOR II): short-term outcomes of a randomised, phase 3 trial. Lancet Oncol 14(3):210–218
Kitano S, Inomata M, Sato A, Yoshimura K, Moriya Y, Japan Clinical Oncology Group Study (2005) Randomized controlled trial to evaluate laparoscopic surgery for colorectal cancer: Japan Clinical Oncology Group Study JCOG 0404. Jpn J Clin Oncol 35(14):1324–32
Bonjer HJ, Deijen CL, Haglind E, COLOR II Study Group (2015) A randomized trial of laparoscopic versus open surgery for rectal cancer. N Engl J Med 372(14):1324--1332
Choi DJ, Kim SH, Lee PJ, Kim J, Woo SU (2009) Single-stage totally robotic dissection for rectal cancer surgery: technique and short-term outcome in 50 consecutive patients. Dis Colon Rectum 52(11):1824–1830
Nagtegaal ID, van de Velde CJ, van der Worp E, Kapiteijn E, Quirke P, van Krieken JH, Cooperative Clinical Investigators of the Dutch Colorectal Cancer Group (2002) Macroscopic evaluation of rectal cancer resection specimen: clinical significance of the pathologist in quality control. J Clin Oncol 20(7):1729–1734
Baek SK, Carmichael JC, Pigazzi A (2013) Robotic surgery: colon and rectum. Cancer J 19(2):140–146
Cho MS, Baek SJ, Hur H, Min BS, Baik SH, Lee KY, Kim NK (2015) Short and long-term outcomes of robotic versus laparoscopic total mesorectal excision for rectal cancer: a case-matched retrospective study. Medicine (Baltimore) 94(11):e522
Park EJ, Cho MS, Baek SJ, Hur H, Min BS, Baik SH, Lee KY, Kim NK (2015) Long-term oncologic outcomes of robotic low anterior resection for rectal cancer: a comparative study with laparoscopic surgery. Ann Surg 261(1):129–137
Bernstein TE, Endreseth BH, Romundstad P, Wibe A, Norwegian Colorectal Cancer Registry (2012) What is a safe distal resection margin in rectal cancer patients treated by low anterior resection without preoperative radiotherapy? Colorectal Dis 14(2):e48–55
Goldstein NS, Sanford W, Coffey M, Layfield LJ (1996) Lymph node recovery from colorectal resection specimens removed for adenocarcinoma. Trends over time and a recommendation for a minimum number of lymph nodes to be recovered. Am J Clin Pathol 106(2):209–216
Park YA, Kim JM, Kim SA, Min BS, Kim NK, Sohn SK, Lee KY (2010) Totally robotic surgery for rectal cancer: from splenic flexure to pelvic floor in one setup. Surg Endosc 24(3):715–720
deSouza AL, Prasad LM, Marecik SJ, Blumetti J, Park JJ, Zimmern A, Abcarian H (2010) Total mesorectal excision for rectal cancer: the potential advantage of robotic assistance. Dis Colon Rectum 53(12):1611–1617
Quirke P, Durdey P, Dixon MF, Williams NS (1986) Local recurrence of rectal adenocarcinoma due to inadequate surgical resection. Histopathological study of lateral tumour spread and surgical excision. Lancet 328(8514):996–999
Wibe A, Rendedal PR, Svensson E, Norstein J, Eide TJ, Myrvold HE, Soreide O (2002) Prognostic significance of the circumferential resection margin following total mesorectal excision for rectal cancer. Br J Surg 89(3):327–334
Kang J, Kim H, Hur H, Min BS, Baik SH, Lee KY, Sohn SK, Kim NK (2013) Circumferential resection margin involvement in stage III rectal cancer patients treated with curative resection followed by chemoradiotherapy: a surrogate marker for local recurrence? Yonsei Med J 54(1):131–138
Hall NR, Finan PJ, Al-Jaberi T, Tsang CS, Brown SR, Dixon MF, Quirke P (1998) Circumferential margin involvement after mesorectal excision of rectal cancer with curative intent. Predictor of survival but not local recurrence? Dis Colon Rectum 41(8):979–983
Bernstein TE, Endreseth BH, Romundstad P, Wibe A, Norwegian Colorectal Cancer Group (2009) Circumferential resection margin as a prognostic factor in rectal cancer. Br J Surg 96(11):1348–1357
Baek JH, McKenzie S, Garcia-Aguilar J, Pigazzi A (2010) Oncologic outcomes of robotic-assisted total mesorectal excision for the treatment of rectal cancer. Ann Surg 251(5):882–886
Pigazzi A, Luca F, Patriti A, Valvo M, Ceccarelli G, Casciola L, Biffi R, Garcia-Aguilar J, Baek JH (2010) Multicentric study on robotic tumor-specific mesorectal excision for the treatment of rectal cancer. Ann Surg Oncol 17(6):1614–1620
Acknowledgments
The authors thank Prof. Seon-Han Kim (Department of Surgery, Korea University Anam Hospital, Korea University College of Medicine) for mentoring of the first robotic surgery, Prof. Jin Cheon Kim (Department of Surgery, University of Ulsan College of Medicine and Asan Medical Center) for teaching about surgical principles and methods for rectal cancer, Seung Yun Lee, M.D., (Eulji University Hospital) for outstanding video narration, and Jin Yeon Kim (Emily Carr University of Art + Design) for drawing the figures.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest or financial ties to disclose.
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Kim, CN., Bae, S.U., Lee, SG. et al. Clinical and oncologic outcomes of totally robotic total mesorectal excision for rectal cancer: initial results in a center for minimally invasive surgery. Int J Colorectal Dis 31, 843–852 (2016). https://doi.org/10.1007/s00384-016-2544-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-016-2544-3