
Abstract
Purpose
Intractable faecal incontinence (FI) and constipation is a challenging condition to manage in children. Transanal irrigation (TAI) is a non-operative treatment option. This study presents our experience with TAI with the aim of finding predictive factors of non-compliance.
Methods
This is an outcome and quality of life (QoL) study of a prospectively maintained database of patients < 17 years old commenced on TAI for intractable FI/constipation between 2008 and 2014. Outcome measures were: (1) compliance—classified as non-adopter (use of TAI stopped within 1 month after commencement) or adopter; (2) functional outcome—classified as responder (totally continent or occasional soiling) or non-responder; (3) Rintala score; and (4) QoL score (PedsQL™ 4.0 Generic Core Scale). Analysis to determine predictive factors was also performed.
Results
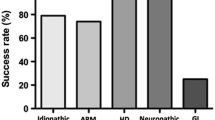
42 patients were started on TAI [74 % male, median age of commencement was 7 (3–16) years]. Underlying diagnoses were: idiopathic constipation (62 %), anorectal malformation (26 %), Hirschsprung disease (5 %), spina bifida (5 %) and gastroschisis (2 %). Median follow-up period was 14 (3–78) months. 24 % were non-adopters. 84 % of the adopters responded to treatment. Rintala scores (mean ± SD) pre- and post-TAI were 6.7 ± 3.5 and 11.2 ± 4.8, respectively (P < 0.001). QoL scores pre- and post-TAI were 55.6 ± 24.1 and 65.5 ± 23.7, respectively (P < 0.001). Median age at which TAI was commenced in the non-adopter and adopter group were 6 (IQR 4.5–8.25) and 8 (IQR 7–12), respectively (P = 0.008).
Conclusion
TAI is a safe and effective treatment for intractable constipation/FI in children. If tolerated, it can significantly improve quality of life. Age and underlying diagnosis are important factors when recommending TAI to children with intractable FI/constipation.



Similar content being viewed by others


References
National Institute for Health and Clinical Excellence (2010) Constipation: the diagnosis and management of idiopathic childhood constipation in primary and secondary care. www.nice.org.uk/CG099
Shandling B, Gilmour RF (1987) The enema continence catheter in spina bifida: successful bowel management. J Pediatr Surg 22:271
Rintala RJ, Lindahl H (1995) Is normal bowel function possible after repair of intermediate and high anorectal malformations? J Pediatr Surg 30:491–494
Varni JW, Seid M, Kurtin PS (2001) PedsQL 4.0: reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med Care 39:800–812
Corbett P, Denny A, Dick K et al (2014) Peristeen integrated transanal irrigation system successfully treats faecal incontinence in children. J Pediatr Urol 10:219–222
Alenezi H, Alhazmi H, Trbay M et al (2014) Peristeen anal irrigation as a substitute for the MACE procedure in children who are in need of reconstructive bladder surgery. Can Urol Assoc J 8:12–15
Pacilli M, Pallot D, Andrews A et al (2014) Use of Peristeen® transanal colonic irrigation for bowel management in children: a single-center experience. J Pediatr Surg 49:269–272
Nasher O, Hill RE, Peeraully R et al (2014) Peristeen transanal irrigation system for paediatric faecal incontinence: a single centre experience. Int J Pediatr. doi:10.1155/2014/954315
Choi EK, Shin SH, Im YJ et al (2013) The effects of transanal irrigation as a stepwise bowel management program on the quality of life of children with spina bifida and their caregivers. Spinal Cord 51:384–388
Märzheuser S, Karsten K, Rothe K (2015) Improvements in incontinence with self-management in patients with anorectal malformations. Eur J Pediatr Surg [Epub ahead of print]
Acknowledgments
We would like to thank Dr James Varni for giving us permission to use the PedsQL™ questionnaire for this non-funded academic project.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ng, J., Ford, K., Dalton, S. et al. Transanal irrigation for intractable faecal incontinence and constipation: outcomes, quality of life and predicting non-adopters. Pediatr Surg Int 31, 729–734 (2015). https://doi.org/10.1007/s00383-015-3735-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-015-3735-7