
Abstract
Objectives
To assess the effect of automatic tube potential selection (ATPS) on radiation dose, image quality, and lesion detectability in paediatric abdominopelvic CT and CT angiography (CTA).
Methods
A paediatric modular phantom with contrast inserts was examined with routine pitch (1.4) and high pitch (3.0) using a standard abdominopelvic protocol with fixed 120 kVp, and ATPS with variable kVp in non-contrast, contrast-enhanced, and CTA mode. The volume CT dose index (CTDIvol), contrast-to-noise ratio (CNR) and lesion detectability index (d’) were compared between the standard protocol and ATPS examinations.
Results
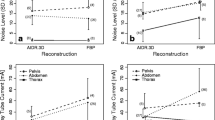
CTDIvol was reduced in all routine pitch ATPS examinations, with dose reductions of 27–52 % in CTA mode (P < 0.0001), 15–33 % in contrast-enhanced mode (P = 0.0003) and 8–14 % in non-contrast mode (P = 0.03). Iodine and soft tissue insert CNR and d’ were improved or maintained in all ATPS examinations. kVp and dose were reduced in 25 % of high pitch ATPS examinations and in none of the full phantom examinations obtained after a single full phantom localizer.
Conclusions
ATPS reduces radiation dose while maintaining image quality and lesion detectability in routine pitch paediatric abdominopelvic CT and CTA, but technical factors such as pitch and imaging range must be considered to optimize ATPS benefits.
Key Points
• ATPS automatically individualizes CT scan technique for each patient.
• ATPS lowers radiation dose in routine pitch pediatric abdominopelvic CT and CTA.
• There is no loss of image quality or lesion detectability with ATPS.
• Pitch and scan range impact the effectiveness of ATPS dose reduction.





Similar content being viewed by others

Abbreviations
- ATPS:
-
Automatic tube potential selection
- d’:
-
Lesion detectability index
References
Funama Y, Awai K, Nakayama Y et al (2005) Radiation dose reduction without degradation of low-contrast detectability at abdominal multisection CT with a low-tube voltage technique: phantom study. Radiology 237(3):905–910
Nakayama Y, Awai K, Funama Y et al (2005) Abdominal CT with low tube voltage: preliminary observations about radiation dose, contrast enhancement, image quality, and noise. Radiology 237(3):945–951
Marin D, Nelson RC, Schindera ST et al (2010) Low-tube-voltage, high-tube-current multidetector abdominal CT: improved image quality and decreased radiation dose with adaptive statistical iterative reconstruction algorithm – initial clinical experience. Radiology 254(1):145–153
Schindera ST, Winklehner A, Alkadhi H, et al (2013) Effect of automatic tube voltage selection on image quality and radiation dose in abdominal CT angiography of various body sizes: a phantom study. Clin Radiol 68(2): e79-86. http://www.sciencedirect.com/science/article/pii/S0009926012005259. Accessed January 17, 2014
Kalva SP, Sahani DV, Hahn PF, Saini S (2006) Using the K-edge to improve contrast conspicuity and to lower radiation dose with a 16-MDCT: a phantom and human study. J Comput Assist Tomogr 30(3):391–397
Yu L, Li H, Fletcher JG, McCollough CH (2010) Automatic selection of tube potential for radiation dose reduction in CT: a general strategy. Med Phys 37(1):234–243
Kalender WA, Deak P, Kellermeier M, van Straten M, Vollmar SV (2009) Application- and patient size-dependent optimization of x-ray spectra for CT. Med Phys 36(3):993–1007
Bischoff B, Hein F, Meyer T et al (2009) Impact of a Reduced Tube Voltage on CT Angiography and Radiation Dose: Results of the Protection 1 Study. JACC Cardiovasc Imaging 2(8):940–946
Nakayama Y, Awai K, Funama Y et al (2006) Lower tube voltage reduces contrast material and radiation doses on 16-MDCT aortography. AJR 187(5):W490–W497
Raman S, Johnson P, Deshmukh S, Mahesh M, Grant KL, Fishman EK (2013) CT dose reduction applications: available tools on the latest generation of CT scanners. J Am Coll Radiol 10(1):37–41
Young C, Owens C (2013) Pediatric computed tomography imaging guideline. Acta Radiol 54(9):998–1006
Siegel MJ, Schmidt B, Bradley D, Suess C, Hildebolt C (2004) Radiation dose and image quality in pediatric CT: effect of technical factors and phantom size and shape. Radiology 233(2):515–522
Yu L, Liu X, Leng S et al (2009) Radiation dose reduction in computed tomography: techniques and future perspective. Imaging Med 1(1):65–84
Yu L, Bruesewitz MR, Thomas KB, Fletcher JG et al (2011) Optimal tube potential for radiation dose reduction in pediatric CT: principles, clinical implementations, and pitfalls. Radiographics 31(3):835–848
Arch ME, Frush DP (2008) Pediatric body MDCT: a 5-year follow-up survey of scanning parameters used by pediatric radiologists. AJR 191(2):611–617
Grant K, Schmidt B (2011) CARE kV: Automated Dose-Optimized Selection of X-ray Tube Voltage, White Paper
Goetti R, Winklehner A, Gordic S et al (2012) Automated attenuation-based kilovoltage selection: preliminary observations in patients after endovascular aneurysm repair of the abdominal aorta. AJR 199(3):W380–W385
Hough DM, Fletcher JG, Grant KL et al (2012) Lowering kilovoltage to reduce radiation dose in contrast-enhanced abdominal CT: Initial assessment of a prototype automated kilovoltage selection tool. AJR 199(5):1070–1077
Eller A, May MS, Scharf M et al (2012) Attenuation-based automatic kilovolt selection in abdominal computed tomography: effects of radiation exposure and image quality. Invest Rad 47(10):559–565
Lee KH, Lee JM, Moon SK et al (2012) Attenuation-based automatic tube voltage selection and tube current modification for dose reduction at contrast-enhanced liver CT. Radiology 265(2):437–447
Mayer C et al (2014) Potential for radiation dose savings in abdominal and chest CT using automatic tube voltage selection in combination with automatic tube current modulation. AJR 203:292–299
Siegel MJ, Ramirez-Giraldo JC, Hildebolt C, Bradley D, Schmidt B (2013) Automated low- kilovoltage selection in pediatric computed tomography angiography. Phantom study evaluating effects on radiation dose and image quality. Invest Radiol 48(8):584–589
Siegel MJ, Hildebolt C, Bradley D (2013) Effects of automated kilovoltage selection technology on contrast-enhanced pediatric CT and CT angiography. Radiology 268(2):538–547
Kleinman PL, Strauss KJ, Zurakowski D, Buckley KS, Taylor GA (2010) Patient size measured on CT images as a function of age at a tertiary care children’s hospital. AJR 194(6):1611–1619
Wilson JM, Christianson OI, Richard S, Samei E (2013) A methodology for image quality evaluation of advanced CT systems. Med Phys 40(3):031908
Gang GJ, Lee J, Stayman JW et al (2011) Analysis of Fourier-domain task-based detectability index in tomosynthesis and cone-beam CT in relation to human observer performance. Med Phys 38(4):1754–1768
Brenner DJ, Hall EJ (2007) Computed tomography – an increasing source of radiation exposure. N Engl J Med 357(22):2277–2284
Brody AS, Frush DP, Huda W, Brent RL (2007) Radiation risk to children from computed tomography. Pediatrics 120(3):677–682
National Academies (2006) Biologic Effects of Ionizing Radiation (BEIR) Report VII: Health risks from exposure to low levels of ionizing radiation
Journy N, Ancelet S, Rehel JL, et al (2013) Predicted cancer risk induced by computed tomography examinations during childhood, by a quantitative risk assessment approach. Radiat Environ Biophys; epub. http://link.springer.com/article/10.1007%Fs00411-013-0491-8/fulltext.html. Accessed January 17, 2014
Samei E, Flynn MJ, Eyler WR (1997) Simulation of subtle lung nodules in projection chest radiography. Radiology 202(1):117–124
Acknowledgements
The scientific guarantor of this publication is Donald P. Frush. The authors of this manuscript declare relationships with the following companies: Juan C. Ramirez-Giraldo is an employee of Siemens Healthcare. Ehsan Samei has research grants from GE and Siemens. The authors state that this work has not received any funding. One of the authors has significant statistical expertise: Kingshuk Roy Choudhury. Institutional Review Board approval was not required because this is a phantom study. Methodology: prospective, experimental, performed at one institution.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Complete Data Experiment 1. Routine Pitch (1.4): Imaging parameter and image quality results of routine protocol with fixed 120 kVp versus automatic tube potential selection protocol (TIFF 128 kb)
Supplementary Material 2
Experiment 1. Routine Pitch (1.4): Analysis of variance† of CTDIvol, contrast-to-noise ratio, and detectability index for automatic tube potential selection examinations (TIFF 129 kb)
Supplementary Material 3
Complete Data Experiment 2. High Pitch (3.0): Imaging parameter and image quality results of routine protocol with fixed 120 kVp versus automatic tube potential selection protocol examinations (TIFF 133 kb)
Supplementary Material 4
Experiment 2. High Pitch (3.0): Analysis of variance† of CTDIvol, contrast-to-noise ratio, and detectability index for automatic tube potential selection examinations (TIFF 136 kb)
Supplementary Material 5
Complete Data Experiment 3. Full Phantom: Imaging parameter and image quality results of routine protocol with fixed 120 kVp versus automatic tube potential selection protocol examinations (TIFF 60 kb)
Appendix 1 Automatic Tube Potential Selection (ATPS) (CARE kV, Siemens Healthcare)
Appendix 1 Automatic Tube Potential Selection (ATPS) (CARE kV, Siemens Healthcare)
CARE kV is a commercially available ATPS software tool which automatically selects a combination of tube potential and tube current according to patient size, prescribed image quality, and examination indication. The patient size is estimated by the use of the CT radiograph localizer (topogram). To define the examination indication and to prescribe the reference image quality, the CARE kV tool uses three parameters: the quality reference mAs, the reference kVp, and the examination type. The quality reference mAs is needed by the automated exposure control system (CARE Dose 4D, Siemens Healthcare). The reference kVp is to be set according to an institution’s established routine clinical protocols, which in conjunction with the defined quality reference mAs are known to provide consistent image quality for a reference patient weighting 70 kg. The examination indication is defined with an incremental slider bar with settings 1 to 12. Lower settings (1–4) are best suited for non-contrast examinations where CARE kV expects the user will accept little or no increase in image noise. Mid-range settings (5–8) are best suited for contrast-enhanced examinations where CARE kV assumes the user will accept a small increase in image noise that will be balanced by a boost of iodine contrast when a lower kVp is selected. Higher settings (9–12) are best suited for CTA examinations where the user expects gains in iodine contrast at lower kVp to offset increased image noise at the lower kVp values. CARE kV aims to maintain the desired CNR as defined by the reference kVp and quality reference mAs.
Appendix 2 Image Analysis with IMQUEST analysis software
Image analysis software developed specifically for the proprietary phantom was used for image analysis. Square ROIs were drawn by a single investigator (40 mm side length for contrast evaluation and 50 mm side length for noise evaluation) with semiautomated measurement of image contrast (contrast = HUinsert - HUpolytethylene body) and image noise (noise = pixel standard deviation of ROIs placed within the uniform phantom body). Contrast-to-noise ratios (CNR = contrastinsert /noise) were calculated for the iodine and soft tissue inserts. A previously validated lesion detectability index, d’, for the iodine and soft tissue inserts was calculated, presented in a simplified format:
where W is the task function, set for the detection of a reference 5 mm designer nodule [31]; TTF is the task transfer function, a measure of system resolution as a function of spatial frequency; E is the Eye Filter, reflecting human visual response characteristics at a typical 60 cm viewing distance; and NPS is the noise power spectrum, a measure of the magnitude and texture characteristics of noise. The d’ values were adjusted to represent a reference feature contrast of 50 Hounsfield Units at 120 kVp for the 12 cm phantom.
Rights and permissions
About this article

Cite this article
Brinkley, M.F., Ramirez-Giraldo, J.C., Samei, E. et al. Effects of automatic tube potential selection on radiation dose index, image quality, and lesion detectability in pediatric abdominopelvic CT and CTA: a phantom study. Eur Radiol 26, 157–166 (2016). https://doi.org/10.1007/s00330-015-3817-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-015-3817-x