
Abstract
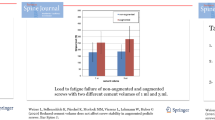
The goal of this cadaver study was to compare the stability of anterior vertebral body screws after implantation in soft or cured kyphoplasty cement. Anterior vertebral body screws were inserted in a total of 30 thoracolumbar vertebrae of ten different human specimens: ten screws were implanted in non-augmented vertebrae (group 1), ten screws were placed in soft cement (group 2), and ten screws were placed in cured cement (group 3). The screws were then tested for biomechanical axial pullout resistance. Mean axial pullout strength was 192 N (range: 10–430 N) in group 1, 364 N (range: 65–875 N) in group 2, and 271 N (range: 35–625 N) in group 3. The paired Student’s t-test demonstrated a significant difference between pullout strength of groups 1 and 2 (p= 0.0475). No significant difference was seen between pullout strength of groups 1 and 3 (p= 0.2646) and between groups 2 and 3 (p= 0.3863). We achieved a 1.9 times higher pullout strength with kyphoplasty augmentation of osteoporotic vertebrae compared with the pullout strength of non-augmented vertebrae. Implantation of anterior vertebral body screws in cured cement is a satisfactory method. With this method we found a 1.4 times higher pullout strength than non-augmented vertebrae.
Résumé
Le but de cette étude est de comparer la stabilité de vis implantées dans le corps vertébral de sujets cadavériques avec ou sans kyphoplastie par ciment. Méthode : 30 vertèbres thoraciques et lombaires sur dix sujets ont été ainsi implantées, 10 vis dans des vertèbres non traitées. Groupe 1 : 10 vis ont été placées dans du ciment mou et 10 vis (groupe 2) et 10 vis (groupe 3) dans du ciment dur. Les vis ont été évaluées sur le plan bio-mécanique et sur la résistance à l’arrachage. Résultat : la résistance à l’arrachage a été de 192 N dans le groupe 1, 1 364 N dans le groupe 2 et 271 N dans le groupe 3. Le test de Student a démontré une différence significative entre groupes 1 et 2 et les groupes 1 et 3, par contre, entre les groupes 2 et 3 il n’a pas été observé de différences significatives. Conclusion : la Kyphoplastie multiplie 1,9 fois la résistance des vertèbres ostéoportiques. Cette technique par inclusion de vis dans le corps vertébral, des vertèbres ainsi traitées est une méthode expérimentale suffisante.


Similar content being viewed by others
References
Bai Bo, Kummer J, Spivak J (2001) Augmentation of anterior vertebral body screw fixation by an injectable, biodegradable calcium phosphate bone substitute. Spine 26(24):2679–2683
Cohen JE, Lylyk P, Ceratto R, Kaplan L, Umanskyt F, Gomori JM (2004) Percutaneous vertebroplasty: technique and results in 192 procedures. Neurol Res 26(1):41–49
Cotten A, Boutry N, Cortet B (1998) Percutaneous vertebroplasty: state of the art. Radiographics 18:311–323
Gangi A, Kastler BA, Dietemann JL (1994) Percutaneous vertebroplasty guided by a combination of CT and fluoroscopy. Am J Neuroradiol 15:83–86
Garfin S, Hansen A, Reiley M (2001) New technologies in spine: kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine 26:1511–1515
Gertzbein SD, Robbins SE (1990) Accuracy of pedicular screw placement in vivo. Spine 15:11–14
Jensen ME, Evans AJ, Mathis JM (1997) Percutaneous polymethylmethacrylate vertebroplasty in the treatment of osteoporotic vertebral body compression fractures: technical aspects. Am J Neuroradiol 18:1897–1904
Kaneda K, Fujiya N, Satoh S (1986) Results with Zielke instrumentation for idiopathic thoracolumbar and lumbar scoliosis. Clin Orthop 205:195–203
Kostuik JP, Carl A, Ferron S (1989) Anterior Zielke instrumentation for spinal deformity in adults. J Bone Joint Surg Am 71:898–912
Kostuik JP, Errico TJ, Gleason TF (1986) Techniques of internal fixation for degenerative conditions of the lumbar spine. Clin Orthop 203:219–231
Moe JH, Purcell GA, Bradford DS (1983) Zielke instrumentation (VDS) for the correction of spinal curvature: analysis of results in 66 patients. Clin Orthop 180:133–153
Molloy S, Mathis JM, Belkoff SM (2003) The effect of vertebral body percentage fill on mechanical behavior during percutaneous vertebroplasty. Spine 28:1549–1554
Pfeifer BA, Krag MH, Johnson C (1994) Repair of failed transpedicular screw fixation: a biomechanical study comparing polymethylmethacrylate, milled bone, and matchstick bone reconstruction. Spine 19:350–353
Renner S, Lim T, Kim W, Katolik L, An H, Andersson G (2004) Augmentation of pedicle screw fixation strength using an injectable calcium phosphate cement as a function of injection timing and method. Spine 29(11):212–216
Sarzier JS, Evans AJ, Cahill DW (2002) Increased pedicle screw pullout strength with vertebroplasty augmentation in osteoporotic spines. J Neurosurg Spine 96(3):309–312
Tomita S, Molloy Sean M, Jasper L, Abe M, Belkoff S (2004) Biomechanical comparison of kyphoplasty with different bone cements. Spine 29(11):1203–1207
World Health Organisation Technical report (1994) Assessment of fracture risk and its application to screening for postmenopausal osteoporosis, series 843
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Linhardt, O., Lüring, C., Matussek, J. et al. Stability of anterior vertebral body screws after kyphoplasty augmentation. International Orthopaedics (SICOT) 30, 366–370 (2006). https://doi.org/10.1007/s00264-006-0100-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-006-0100-4