
Abstract
Purpose
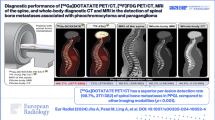
It is challenging to differentiate unilateral aldosterone-producing adenoma (APA) from bilateral idiopathic adrenal hyperplasia (IAH) and nonfunctional adrenal adenoma (NFA) in primary aldosteronism (PA). In a first primarily ex vivo study detection, CXC chemokine receptor type 4 (CXCR4) expression has been shown to be a valuable tool for the detection of APA. In this study, we aimed to clinically evaluate CXCR4 imaging with 68Ga-pentixafor PET/CT for detecting APA.
Methods
We prospectively recruited 36 patients with clinical suspicion of PA. All patients underwent 68Ga-pentixafor PET/CT. Positive lesions were defined based on higher tracer uptake in adrenal nodular(s) shown on CT than the normal adrenal. These lesions were referred for adrenalectomy subsequently. All patients received clinical follow-up. Semi-quantitative analysis using maximum standardized uptake value (SUVmax), lesion-to-liver ratio (LLR), and lesion-to-contralateral ratio (LCR) has also been performed. PET/CT results were correlated with clinical presentation and follow-up.
Results
Thirty-nine adrenal lesions in 36 patients were found; 25 APA, 4 IAH, and 10 NFA according to histopathology and clinical assessment. Sensitivity, specificity, and accuracy of 68Ga-pentixafor PET/CT in distinguishing APA by visualization were 100%, 78.6%, and 92.3% respectively. The SUVmax of APA (21.34 ± 9.41, n = 25) was significantly higher than that of non-APA lesions (6.29 ± 2.10, n = 14, P < 0.0001). An optimal threshold of SUVmax = 11.18 was determined for predicting APA with a sensitivity of 88.0%, specificity of 100%, and an accuracy of 92.3%. A cutoff value for LCR of 2.12 yielded a sensitivity of 100% and a specificity of 92.9%, whereas a cutoff value for LLR of 2.36 reached at both 100% of sensitivity and specificity. All patients with (removed) positive lesions benefited from surgery.
Conclusion
68Ga-Pentixafor PET/CT may be used to non-invasively detect APA in PA patients.




Similar content being viewed by others


References
Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(5):1889–916.
Monticone S, D’Ascenzo F, Moretti C, Williams TA, Veglio F, Gaita F, et al. Cardiovascular events and target organ damage in primary aldosteronism compared with essential hypertension: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2018;6(1):41–50.
Monticone S, Burrello J, Tizzani D, Bertello C, Viola A, Buffolo F, et al. Prevalence and clinical manifestations of primary aldosteronism encountered in primary care practice. J Am Coll Cardiol. 2017;69(14):1811–20.
Li LL, Gu WJ, Dou JT, Yang GQ, Lv ZH, et al. Incidental adrenal enlargement: an overview from a retrospective study in a Chinese population. Int J Endocrinol. 2015;2015:192874.
Nanba AT, Nanba K, Byrd JB, Shields JJ, Giordano TJ, Miller BS, et al. Discordance between imaging and immunohistochemistry in unilateral primary aldosteronism. Clin Endocrinol. 2017;87(6):665–72.
Rossi GP. Update in adrenal venous sampling for primary aldosteronism. Curr Opin Endocrinol Diabetes Obes. 2018;25(3):160–71.
Okamura K, Okuda T, Shirai K, Abe I, Kobayashi K, Ishii T, et al. Persistent primary aldosteronism despite iatrogenic adrenal hemorrhage after adrenal vein sampling. J Clin Med Res. 2018;10(1):66–71.
Layden BT, Hahr AJ, Elaraj DM. Primary hyperaldosteronism: challenges in subtype classification. BMC Res Notes. 2012;5:602.
Powlson AS, Gurnell M, Brown MJ. Nuclear imaging in the diagnosis of primary aldosteronism. Curr Opin Endocrinol Diabetes Obes. 2015;22(3):150–6.
Heinze B, Fuss CT, Mulatero P, Beuschlein F, Reincke M, Mustafa M, et al. Targeting CXCR4 (CXC chemokine receptor type 4) for molecular imaging of aldosterone-producing adenoma. Hypertension. 2018;71(2):317–25.
Walenkamp AME, Lapa C, Herrmann K, Wester HJ. CXCR4 ligands: the next big hit? J Nucl Med. 2017;58(Suppl 2):77S–82S.
Williams TA, Lenders JWM, Mulatero P, Burrello J, Rottenkolber M, Adolf C, et al. Outcomes after adrenalectomy for unilateral primary aldosteronism: an international consensus on outcome measures and analysis of remission rates in an international cohort. Lancet Diabetes Endocrinol. 2017;5(9):689–99.
Itcho K, Oki K, Kobuke K, Yoshii Y, Ohno H, Yoneda M, et al. Aberrant G protein-receptor expression is associated with DNA methylation in aldosterone-producing adenoma. Mol Cell Endocrinol. 2018;461:100–4.
O’Shea PM, Griffin TP, Denieffe S, Fitzgibbon MC. The aldosterone to renin ratio (ARR) in the diagnosis of primary aldosteronism (PA): promises and challenges. Int J Clin Pract. 2019;73(7):e13353.
Käyser SC, Dekkers T, Groenewoud HJ, van der Wilt GJ, Carel Bakx J, van der Wel MC, et al. Study heterogeneity and estimation of prevalence of primary aldosteronism: a systematic review and meta-regression analysis. J Clin Endocrinol Metab. 2016;101(7):2826–35.
Young WF, Stanson AW, Thompson GB, Grant CS, Farley DR, van Heerden JA. Role for adrenal venous sampling in primary aldosteronism. Surgery. 2004;136(6):1227–35.
Yen RF, Wu VC, Liu KL, Cheng MF, Wu YW, Chueh SC, et al. 131I-6beta-iodomethyl-19-norcholesterol SPECT/CT for primary aldosteronism patients with inconclusive adrenal venous sampling and CT results. J Nucl Med. 2009;50(10):1631–7.
Wang T, Satoh F, Morimoto R, Nakamura Y, Sasano H, Auchus RJ, et al. Gene expression profiles in aldosterone-producing adenomas and adjacent adrenal glands. Eur J Endocrinol. 2011;164(4):613–9.
Burton TJ, Mackenzie IS, Balan K, Koo B, Bird N, Soloviev DV, et al. Evaluation of the sensitivity and specificity of (11)C-metomidate positron emission tomography (PET)-CT for lateralizing aldosterone secretion by Conn’s adenomas. J Clin Endocrinol Metab. 2012;97(1):100–9.
Mendichovszky IA, Powlson AS, Manavaki R, Aigbirhio FI, Cheow H, Buscombe JR, et al. Targeted molecular imaging in adrenal disease-an emerging role for metomidate PET-CT. Diagnostics (Basel). 2016;6(4). https://doi.org/10.3390/diagnostics6040042.
Kreissl MC, Schirbel A, Fassnacht M, Haenscheid H, Verburg FA, Bock S, et al. [(1)(2)(3)I]Iodometomidate imaging in adrenocortical carcinoma. J Clin Endocrinol Metab. 2013;98(7):2755–64.
Hahner S, Kreissl MC, Fassnacht M, Haenscheid H, Bock S, Verburg FA, et al. Functional characterization of adrenal lesions using [123I]IMTO-SPECT/CT. J Clin Endocrinol Metab. 2013;98(4):1508–18.
Nanba K, Tsuiki M, Sawai K, Mukai K, Nishimoto K, Usui T, et al. Histopathological diagnosis of primary aldosteronism using CYP11B2 immunohistochemistry. J Clin Endocrinol Metab. 2013;98(4):1567–74.
Acknowledgments
We are grateful to Dr. Celso E. Gomez-Sanchez (Department of Medicine, University of Mississippi Medical Center, Jackson, Mississippi), who kindly provided us antibodies against CYP11B2.
Funding
This work was sponsored in part by the National Natural Science Foundation of China (Grant No. 81571713), CAMS Innovation Fund for Medical Sciences (CIFMS). Grant No. 2016-I2M-4-003, CAMS initiative for innovative medicine (No. CAMS-2018-I2M-3-001). The National Natural Science Foundation of China (81601529), the Tianjin Natural Science Foundation (18JCQNJC11600).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
SCINTOMICS owns the IP on Pentixafor. All other authors declare that they have no conflict of interest.
Ethical approval
The clinical institutional review board approved this study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Endocrinology
Rights and permissions
About this article

Cite this article
Ding, J., Zhang, Y., Wen, J. et al. Imaging CXCR4 expression in patients with suspected primary hyperaldosteronism. Eur J Nucl Med Mol Imaging 47, 2656–2665 (2020). https://doi.org/10.1007/s00259-020-04722-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-020-04722-0