
Abstract
Purpose
Acute monoamine depletion paradigms using alpha-methyl-para-tyrosine (AMPT) combined with single photon emission computed tomography (SPECT) have been used successfully to evaluate disturbances in central dopaminergic neurotransmission. However, severe side effects due to relatively high doses (4,500 to 8,000 mg) of AMPT have been reasons for study withdrawal. Thus, we assessed the effectiveness and tolerability of two alternative procedures, using lower doses of AMPT.
Methods
Six healthy subjects underwent three measurements of striatal dopamine D2 receptor (D2R)-binding potential (BPND) with SPECT and the selective radiolabeled D2R antagonist [123I]IBZM. All subjects were scanned in the absence of pharmacological intervention (baseline) and after two different depletion procedures. In the first depletion session, over 6 h, subjects were administered 1,500 mg of AMPT before scanning. In the second depletion session, over 25 h, subjects were administered 40 mg AMPT/kg body weight. We also administered the Subjective Well-being Under Neuroleptic Treatment Scale, a self-report instrument designed to measure the subjective experience of patients on neuroleptic medication.
Results
We found no change of mean D2R BPND after the first and short AMPT challenge compared to the baseline. However, we found a significant increase in striatal D2R BPND binding after the AMPT challenge adjusted for bodyweight compared to both other regimen. Although subjective well-being worsened after the prolonged AMPT challenge, no severe side effects were reported.
Conclusions
Our results imply a low-dosage, suitable alternative to the common AMPT procedure. The probability of side effects and study withdrawal can be reduced by this procedure.
Similar content being viewed by others

Introduction
Several neuropsychiatric disorders have been associated with disturbances of the catecholaminergic neurotransmitters dopamine (DA) and norepinephrine (NE), including schizophrenia [1], mood disorders [2, 3] and Parkinson’s disease [4]. Strategies to increase our knowledge of these neurotransmitter systems combining pharmacologic challenges with neuroimaging techniques like positron emission tomography (PET) and single photon emission computed tomography (SPECT) are extensively used. The development of such experimental procedures has allowed for the investigation of associations between the function of neurotransmitters and neuropsychiatric disorders. For example, employing such a challenge paradigm, it has been shown that there is an increased occupancy of DA D2 receptors (D2R) by endogenous DA in schizophrenic patients compared to the controls [5]. In addition, monoamine depletion studies demonstrate that, although monoamine systems are probably important in the vulnerability to mood lability, there is no simple direct causal relation between catecholamines and mood, as proposed in the monoamine hypothesis of mood disorders [3, 6, 7].
Catecholamine depletion paradigms have been used most frequently in two ways. First, dietary restriction of the catecholamine precursors phenylalanine and tyrosine has been used in the so-called acute tyrosine depletion or phenylalanine/tyrosine depletion (APTD) [6]. APTD involves the restriction of the precursor amino acid, phenylalanine and tyrosine, intake during 1 day, followed by the consumption of an amino acid mixture that lacks phenylalanine and tyrosine the next morning [6]. As this mixture stimulates protein synthesis, which requires phenylalanine and tyrosine, less of the amino acids phenylalanine and tyrosine are available for the brain [6]. Although the biochemical effects of this procedure in the brain remain unclear, it is believed that APTD mainly affects DA synthesis [6]. Experience with APTD challenges in combination with neuroimaging techniques is limited, and we are aware of only two such studies. In one PET study in seven healthy men, APTD induced an increased [11C]raclopride binding by a mean of 6% [8]. Second, Leyton et al. [9] presented a PET study in eight healthy men that provided evidence for APTD to decrease amphetamine-induced DA release. Except for limited experiences, disadvantages of APTD include an unpalatable taste [10] and nausea [11], and study subjects tend to report that they feel less good after this diet [12]. Another way to induce catecholamine depletion is by administration of alpha-methyl-para-tyrosine (AMPT). AMPT is a competitive inhibitor of the rate-limiting enzyme of catecholamine synthesis and tyrosine hydroxylase [13], and affects both DA and NE synthesis [6]. It has been suggested that AMPT produces a substantially greater impairment in DA release than tyrosine depletion does [11]. However, side effects, which are dose-related, may be serious and can be reason for withdrawal. For example, severe side effects that have been reported previously include serious psychiatric symptoms [14], crystalluria and acute dystonia [5, 15]. Common AMPT depletion procedures involve a 25- to 48-h study period in which study subjects administer a total amount of 4,500–8,000 mg AMPT [6]. Nevertheless, other studies showed significant depletion effects on indirect dopaminergic markers including measures of peripheral DA, its metabolites and the hormone prolactin (PRL) after lower doses of AMPT [16, 17]. For this, it could be hypothesized that, to induce measurable effects of DA depletion with PET or SPECT, lower dosages than the common 4,500–8,000 mg AMPT may be sufficient.
Moreover, lower doses of AMPT could possibly reduce side effects as well and would therefore allow testing subjects in complex neuropsychological tasks and imaging experiments. To estimate the effects of reduced dopaminergic neurotransmission, we administered a self-report instrument, the Subjective Well-being Under Neuroleptic Treatment Scale (SWN) [18–20]. For example, initial studies using this instrument provided evidence that negative subjective experience is related to high DA D2R occupancy in patients treated with antipsychotic medication, reflecting a hypodopaminergic state [21, 22].
The aim of this study was to assess the effectiveness and tolerability of two alternative procedures for the commonly used acute AMPT depletion challenge paradigm and simultaneous D2R SPECT imaging, using relatively low doses of AMPT.
Materials and methods
Subjects
The study protocol was approved by the Ethics Committee of the Academic Medical Centre of Amsterdam. Each participant gave written informed consent after explaining the full study procedure. Six healthy volunteers older than 18 years but younger than 40 years were included. The exclusion criteria were (1) current or past psychiatric history, (2) current or previous exposure to antipsychotic or stimulant medication, (3) lifetime history of alcohol or substance abuse or dependence, (4) concomitant or past severe medical conditions and (5) pregnancy, based on a clinical interview and the urine ßHCG test.
Depletion regimen
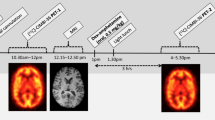
Each subject was scanned three times, once in the baseline state (D1) and twice after DA depletion (D2, D3) with an interval ranging from one to nine and from 49 to 110 weeks, respectively. DA depletion was induced by oral administration of AMPT. In a short AMPT challenge session using a low fixed dose of AMPT (D2), the total AMPT dose administered was 1,500 mg over 4 h. The first dose (500 mg) was given on the morning (D2T0). Subsequently, 500 mg AMPT was administered 2 h after baseline (D2T2) and 4 h after baseline (500 mg, D2T4). Scans were acquired 1 h after the last AMPT dose (D2T5).
In the second and more prolonged challenge session (D3), DA depletion was induced by oral administration of AMPT over 24 h. The exact AMPT dose was calculated on a per weight basis (40 mg/ kg body weight). The overall AMPT dose was spread equally in 250-mg capsules over four time points. Three doses were given 1 day before the scan: at baseline (D3T0), 6 h after baseline (D3T6) and 12 h after baseline (D3T12). The last AMPT dose was given 24 h after D3T0 (D3T24) and 1 h before the beginning of the scanning session (D3T25). To prevent the formation of AMPT crystals in the urine, subjects were instructed to drink plenty of fluids.
SPECT protocol
All subjects took potassium iodide orally (three doses of 40 mg on the day before imaging and 80 mg just before imaging) to block thyroid uptake of free radioactive iodide. The subjects underwent three measurements of D2R-binding potential (BPND) [23], with SPECT and the selective iodine-123-labeled D2R antagonist (S)-(–)-3-iodo-2-hydroxy-6-methoxy-N-[(1-ethyl-2-pyrrolidinyl)methyl]benzamide ([123I]IBZM), using the sustained equilibrium/constant infusion technique [24]. A total [123I]IBZM dose (specific activity > 200 MBq/nmol and radiochemical purity > 95%) of approximately 56 MBq was given as a bolus, followed by a continuous infusion for the duration of the experiment (180 min). The bolus to hourly infusion ratio was approximately 4.0 [25]. This protocol of administration induces a state of sustained binding equilibrium after 120 min [25]. SPECT data were acquired for approximately 60 min, from 120 to 180 min after the initiation of [123I]IBZM administration. SPECT studies were performed using a 12-detector single slice brain-dedicated scanner (Neurofocus 810, which is an upgrade of the Strichmann Medical Equipment) with a full-width at half maximum resolution of approximately 6.5 mm, throughout the 20 cm field-of-view (http://www.neurophysics.com). After positioning of the subjects with the head parallel to the orbitomeatal line, axial slices parallel and upward from the orbitomeatal line to the vertex were acquired in 5 mm steps. Each acquisition consisted of approximately 12–13 slices with 5 min scanning time per slice, acquired in a 64 × 64 matrix. The energy window was set at 135–190 keV. At the day of the imaging session, the participants were not allowed to consume coffee or alcohol because they have been associated with altered striatal DA release [26]. The first scan was obtained in the absence of pharmacological intervention (baseline scan), on the first day of the study (D1). The second and third scans were performed after DA depletion induced by oral administration of AMPT, as described previously. Thus, three measures of striatal D2R binding were obtained in each subject: at baseline (D1), in the short session (D2) after 1,500 mg of AMPT and in the prolonged depleted state (D3) after a body-weight-adjusted AMPT dose.
Image reconstruction and analysis
SPECT data were reconstructed and analyzed blind to clinical data by the same experienced investigator (J.B.). Attenuation correction of all images was performed as earlier described [27]. Images were reconstructed in 3D mode (http://www.neurophysics.com). For quantification, a region-of-interest (ROI) analysis was performed. Fixed ROIs for the striatum and occipital cortex were used. For the right and left striatum and left and right occipital cortex, a template with irregular ROIs, according to the contour of the striatum and occipital cortex, was positioned on four consecutive axial slices with highest striatal activity. Individual variation required movement of the fixed ROIs, without changing size and shape, within the template for optimal fitting. For the right occipital and left occipital cortices, irregular ROIs were drawn in one template. Mean striatal and mean occipital binding densities were averaged from right and left ROIs. BPND was calculated as the ratio of specific to non-specific activity (total activity in striatum minus activity in occipital cortex, divided by activity in occipital cortex).
Prolactin
Blood samples were taken at D2T0, D2T3 and D2T6 at the short scanning day and at D3T26 at the prolonged scanning day for determination of plasma PRL levels. The cannula was flushed with NaCl 0.9% to ensure that the cannula remained open. PRL was measured by time-resolved fluoroimmunoassay (DELFIA Prolactin, Wallac Oy, Turku, Finland). The samples were not run in one-assay run to mimic the real diagnostic procedure. The total assay variation ranged from 5.8–7.6%.
Subjective well-being during depletion
To determine subjective well-being, the short version of the SWN [18–20] (Dutch translation) was administered to the subjects at baseline (D2T0) after the administration of 1,500 mg AMPT (D2T6) and in the prolonged challenge session, 24 h after the first AMPT dose (D3T24). This scale with six response categories covers 20 statements on five subscales (mental functioning, self-control, emotional regulation, physical functioning, social integration).
Statistical analysis
Statistical analyses concerning the differences in BPND, SWN scores and PRL levels, at the different time points, were performed using the non-parametric Wilcoxon test for paired samples. Spearman’s rho correlation coefficients were calculated to investigate the relationship between BPND, SWN scores and PRL levels. A probability value of 0.05 two-tailed was selected as significance level. Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS, release 12.0.1 for Windows).
Results
Six healthy subjects completed the study. The age (mean ± standard deviation) of the subjects was 29.3 ± 6.95 years, respectively. There were three women and three men included. None of the subjects smoked. After AMPT administration, no serious adverse events like acute dystonia or crystalluria were present.
Striatal D2 binding
There was no significant difference in mean BPND binding at baseline (D1) and 5 h after the administration of 1,500 mg AMPT (D2T5, Fig. 1). The relative change of mean BPND compared to the baseline after a more prolonged challenge state (D3T25) with a body-weight-adjusted AMPT dose ranged between −2.1% and 20.4% with a mean relative increase of 8.8% ± 9.0%, which was statistically significant (n = 6, p = 0.046, Wilcoxon test for paired samples). In only one subject, the mean BPND was lower after the more prolonged challenge procedure than at baseline. In all subjects, the mean [123I]IBZM binding was higher in the prolonged challenge state compared to the short challenge state. There was a significant difference of mean BPND between the short challenge D2T5 and the more prolonged challenge D3T25 (p = 0.028).

Effect of alpha-methyl-para-tyrosine (AMPT) on the mean [123I]IBZM striatal dopamine D2 receptor (D2R)-binding potential (BPND). The D2R BPND was measured at baseline (D1T0), after the administration of 1,500 mg AMPT at 5 h after the first drug intake (D2T5) and after 40 mg AMPT/kg body weight, 25 h after the first drug intake (D3T25). The mean D2R BPND after 40 mg AMPT/kg was significantly different from baseline (p = 0.046) and D2T5 (p = 0.028), Wilcoxon test for paired samples
Prolactin
There was a significant increase (p = 0.028) of mean PRL levels from baseline (D2T0, n = 6, 10.6 ± 4.3 μg/l) after the administration of 1,500 mg AMPT at 3 h after the first drug intake (D2T3, n = 6, 89.0 ± 41.8 μg/l; Fig. 2). The levels decreased subsequently at D2T6 (n = 6, 47.2 ± 18.3, p = 0.028; compared with D2T3) in all subjects and stayed above baseline values (p = 0.028). The PRL levels (n = 4, 37.8 ± 12.6) after a body-weight-adjusted AMPT dose, 26 h after the first drug intake (D3T26), were not significantly different from baseline (p = 0.068). No correlations were detected between D2R BPND and PRL levels.

Mean plasma prolactin (PRL, µg/l) levels after alpha-methyl-para-tyrosine (AMPT) administration. The plasma levels were measured at baseline (D2T0) after the administration of 1,500 mg AMPT at 3 h (D2T3) and 6 h (D2T6) after the first drug intake and after 40 mg AMPT/kg body weight, 26 h after the first drug intake (D3T26). Error bars indicate SEM
Subjective well-being during dopamine depletion
SWN scores at baseline (D2T0) and after dopamine depletion (D2T6, D3T24) are displayed in Fig. 3. There were no differences in SWN scores at baseline and after the administration of 1,500 mg AMPT. After prolonged dopamine depletion, the mean total SWN scores dropped significantly (p = 0.028) by 31.5 ± 27.6 points compared to the baseline, indicating a worsening in subjective experience. There was a significant decline of the subscales mental functioning (p = 0.043), emotional regulation (p = 0.042) and physical functioning (p = 0.043). No correlations were detected between D2R BPND and SWN scores.

Effect of AMPT on subjective well-being as measured with the SWN. Mean SWN scores were measured at baseline (D2T0) after the administration of 1,500 mg AMPT at 6 h after the first drug intake (D2T6) and after 40 mg AMPT/kg body weight, 24 h after the first AMPT dose (D3T24). Error bars indicate SEM. mf mental functioning, er emotional regulation, pf physical functioning. Total and subscales presented showed a significant AMPT effect, p < 0.05; Wilcoxon test for paired samples
Discussion
In this study, we describe induction of acute monoamine depletion with two alternative procedures to the common AMPT procedure evaluated with [123I]IBZM SPECT using relatively low doses of AMPT. We found no change of mean striatal [123I]IBZM BPND after the first and short AMPT challenge compared to the baseline. However, this study showed that AMPT administration (40 mg/kg body weight, over 25 h) induced a significant increase (+8.8 ± 9.0%) in measured BPND in six healthy volunteers. For interpretation of the present work, the following issues must be considered.
The purpose of monoamine depletion paradigms is to investigate associations between the function of neurotransmitters and neuropsychiatric disorders in humans. The original AMPT procedure in humans was based on the assumption of complete synaptic DA depletion [28]. Under this assumption, the difference between [123I]IBZM SPECT scans before and after acute DA depletion provides a measure of the proportion of striatal D2R occupied by endogenous DA at baseline. In this initial procedure, AMPT was selected as the depleting agent because this drug was approved for human use and because AMPT effects are rapidly reversible. The dose and frequency to obtain DA depletion were based on findings from previous studies. In these studies, it was found that doses exceeding 1,000 mg daily result in an enzyme inhibition (tyrosine hydroxylase) of more than 50% and that stepwise increment of dosages up to 1,500 mg per day produce marked increases in inhibition of catecholamine production [29]. Another study showed a decrease of the DA metabolite homovanillic acid in cerebrospinal fluid with an interval ranging from 68% to 77% after 4,000 mg AMPT per day [30]. In these studies, it was also found that higher doses of AMPT did not induce significantly more inhibition of the enzyme tyrosine hydroxylase [13, 28]. With a half-life of about 4 h and a peak plasma concentration of about 2 h after oral administration, the ingestion of AMPT every 6 h for 2 days was expected to provide suitable plasma concentrations at steady state. Therefore, in the original AMPT procedure, a total dose of 8,000 mg AMPT over 2 days (1 g every 6 h) was administered orally. As in this study, the subjects presented extrapyramidal symptoms and as 80% D2R blockade is expected to provoke these symptoms, depletion was suggested in the 70% to 80% range [28].
As a lot of adverse effects were reported in the first depletion studies, Verhoeff et al. [17] reduced the total amount of administered AMPT to 4,500 mg over 28 h. Using PET and the radioligand [11C]raclopride, AMPT resulted in significant increase in D2R BP with a magnitude comparable with earlier findings, suggesting comparable changes in striatal DA concentration with lower AMPT doses. Ever since, administered AMPT dosages in neuroimaging challenge studies have been about 4,500 mg over 2 days. Nevertheless, though the following studies did not administer the total dose of 8,000 mg AMPT, side effects and study withdrawal were still a dilemma [14].
The occurrence of side effects due to these relatively high doses (4,500 to 8,000 mg) and the knowledge that AMPT does not completely block tyrosine hydroxylase [13, 28] raise the question of the necessity of maximum DA depletion to study the dysregulation of the DA system. We belief that a depletion paradigm is equally valuable to investigate whether patients with different neuropsychiatric disorders differ in the response to an adequate DA challenge. This requires that the effect of AMPT on striatal [123I]IBZM BPND should at least be significant and reliable.
Although the magnitude of the AMPT-induced change of striatal [123I[IBZM BPND in our sample is small, the change is significant. Moreover, our findings are in accordance with the findings of an IBZM SPECT study that showed a significant AMPT effect on mean striatal BPND (+9% ± 7%) in a sample of 18 healthy subjects with comparable mean age (31 ± 8 years), receiving a total dose of 8,000 mg AMPT, over 48 h [5]. Besides, studies have demonstrated that the between-study variability in the AMPT effect in general is quite large. For example, in other PET and SPECT studies in healthy subjects, with 4,000–8,000 mg AMPT over 48 h, mean differences in striatal D2R BPND ranged from +13% to +28% [17, 28, 31, 32]. The between-subject variability in the present study is large as well (ranges from −2.1% and 20.4%), which is also in agreement with findings by others. It has to be taken into account that these studies did not employ the same instrumentation and methodology. However, to our best knowledge, test–retest variability using the bolus plus constant infusion paradigm with IBZM SPECT after AMPT challenge has not been reported yet. Therefore, similarities and differences in the AMPT effect in the mentioned studies should be interpreted with caution.
Thus, our data suggest that, to induce acute DA depletion to measure acute changes in striatal synaptic DA concentration in vivo, this procedure with relative low doses of AMPT is a suitable alternative to the common AMPT procedure. The probability of side effects and study withdrawal can be reduced by this procedure. However, it is uncertain if the magnitude of striatal DA depletion achieved by this regimen is equally sufficient to demonstrate dysfunction of neurotransmitters in neuropsychiatric disorders as the original AMPT procedure. Future studies using this paradigm in psychiatric populations should address this issue. Moreover, although our present results (particularly the results obtained with the AMPT challenge adjusted for bodyweight) suggest that we induced a significant reduction of DA concentrations, including striatal synaptic DA, we do not know the extent of this reduction. As we did not observe extrapyramidal side effects, striatal DA depletion may be less than 70–80%. Additional studies are needed to estimate the actual depletion of striatal DA concentrations, which could be induced with this novel procedure. To do so, it might be of value to measure plasma AMPT levels in humans and induce comparable plasma levels in small laboratory animals. In the same animal experiment, microdialysis can be performed to assess the actual extracellular striatal DA concentrations. Although such a strategy can be used to estimate the effects on extracellular DA levels, it does not reflect changes on the synaptic level (for a discussion, see Schiffer et al. [33]). Alternatively, one may estimate the depletion by measures of the predominant DA metabolite homovanillic acid (HVA) in cerebrospinal fluid in humans, but it is expected that the magnitude of DA depletion is larger than HVA depletion [5].
In agreement with previous studies applying the AMPT paradigm in healthy volunteers [17, 29, 34, 35], AMPT administration increased serum PRL levels significantly shortly after its first administration, and PRL levels fell thereafter, even though more AMPT was administered. AMPT-induced DA depletion consistently produced a two- to ninefold increase in PRL levels [17, 29, 34, 35]. Previously, PRL has been used as a marker of the effectiveness of AMPT as an inhibitor of endogenous DA synthesis [35] because hypothalamic DA is known to inhibit PRL release at the level of the pituitary gland [36]. However, DA is not the only factor controlling PRL levels, and there is no direct relation between hypophysial stalk DA levels and serum PRL levels [36]. Thus, our findings, taken together with the results from the mentioned studies, suggest that, though an initial PRL response indicates acute DA depletion, it may not be a useful indicator of the adequacy of DA depletion in striatum.
Subjective experience worsened in the prolonged procedure, with effect on mental functioning, emotional regulation and physical functioning, as measured by the SWN scale. From studies with antipsychotics, we know that antagonism of dopaminergic neurotransmission is relevant for subjective experience, and higher striatal D2R occupancy by antipsychotics is related to worse subjective experience [37]. These type of subjective side effects have been labeled as ‘neuroleptic dysphoria’ [38] or neuroleptic-induced anhedonia [20]. In addition, subjective well-being during antipsychotic medication is associated with medication compliance [37], and discomfort is reason for study withdrawal in AMPT challenge studies [5, 39]. Thus, although a relatively low dose of AMPT was administered, subjective well-being worsened. Nevertheless, all the subjects completed the study, in contrast to some other AMPT challenge studies using higher AMPT doses.
The results of the present study should be interpreted in light of the following considerations. The order of scanning and depletion was not randomized. Therefore, we cannot rule out a time or order effect. In addition, the sample size is limited; however, the effect exceeds p < 0.05. Also, compared to PET, clinical SPECT investigations have the disadvantage of lower resolution. Finally, our findings will need to be replicated in independent studies.
In conclusion, this study demonstrates that a relatively low, body-weight-adjusted AMPT dose effectively reduced dopamine concentration in the brain. The probability of dose-related severe side effects and study withdrawal can be reduced by this procedure. Moreover, this safe and well-tolerated pharmacological challenge appears to be well-suited to study the relationship between the catecholaminergic function and neuropsychiatric conditions in future studies using neuropsychological tasks and functional neuroimaging.
References
Takahashi H, Higuchi M, Suhara T. The role of extrastriatal dopamine D2 receptors in schizophrenia. Biol Psychiatry 2006;59:919–28.
Dunlop BW, Nemeroff CB. The role of dopamine in the pathophysiology of depression. Arch Gen Psychiatry 2007;64:327–37.
Ruhé HG, Mason NS, Schene AH. Mood is indirectly related to serotonin, norepinephrine and dopamine levels in humans: a meta-analysis of monoamine depletion studies. Mol Psychiatry 2007;12:331–59.
Olanow CW, Obeso JA, Stocchi F. Continuous dopamine-receptor treatment of Parkinson’s disease: scientific rationale and clinical implications. Lancet Neurol 2006;5:677–87.
Abi-Dargham A, Rodenhiser J, Printz D, Zea-Ponce Y, Gil R, Kegeles LS, et al. Increased baseline occupancy of D2 receptors by dopamine in schizophrenia. Proc Natl Acad Sci 2000;97:8104–9.
Booij L, van der Does AJ, Riedel WJ. Monoamine depletion in psychiatric and healthy populations: review. Mol Psychiatry 2003;8:951–73.
Kapur S, Mann JJ. Role of the dopaminergic system in depression. Biol Psychiatry 1992;32:1–17.
Montgomery AJ, McTavish SF, Cowen PJ, Grasby PM. Reduction of brain dopamine concentration with dietary tyrosine plus phenylalanine depletion: an [11C]raclopride PET study. Am J Psychiatry 2003;160:1887–9.
Leyton M, Dagher A, Boileau I, Casey K, Baker GB, Diksic M, et al. Decreasing amphetamine-induced dopamine release by acute phenylalanine/tyrosine depletion: A PET/[11C]raclopride study in healthy men. Neuropsychopharmacology 2004;29:427–32.
Moja EA, Lucini V, Benedetti F, Lucca A. Decrease in plasma phenylalanine and tyrosine after phenylalanine-tyrosine free amino acid solutions in man. Life Sci 1996;58:2389–95.
McTavish SF, Mannie ZN, Harmer CJ, Cowen PJ. Lack of effect of tyrosine depletion on mood in recovered depressed women. Neuropsychopharmacology 2005b;30:786–91.
Harmer CJ, McTavish SF, Clark L, Goodwin GM, Cowen PJ. Tyrosine depletion attenuates dopamine function in healthy volunteers. Psychopharmacology (Berl) 2001;154:105–11.
Engelman K, Jequier E, Udenfriend S, Sjoerdsma A. Metabolism of alpha-methyltyrosine in man: relationship to its potency as an inhibitor of catecholamine biosynthesis. J Clin Invest 1968;47:568–76.
de Haan L, Booij J, Lavalye J, van Amelsvoort T, Linszen D. Subjective experiences during dopamine depletion. Am J Psychiatry 2005;162:1755.
Voruganti L, Slomka P, Zabel P, Costa G, So A, Mattar A, et al. Subjective effects of AMPT-induced dopamine depletion in schizophrenia: correlation between dysphoric responses and striatal D(2) binding ratios on SPECT imaging. Neuropsychopharmacology 2001;25:642–50.
Stine SM, Krystal JH, Petrakis IL, Jatlow PI, Heninger GR, Kosten TR, et al. Effect of alpha-methyl-para-tyrosine on response to cocaine challenge. Biol Psychiatry 1997;42:181–90.
Verhoeff NP, Kapur S, Hussey D, Lee M, Christensen B, Psych C, et al. A simple method to measure baseline occupancy of neostriatal dopamine D2 receptors by dopamine in vivo in healthy subjects. Neuropsychopharmacology 2001;25:213–23.
de Haan L, Weisfelt M, Dingemans PM, Linszen DH, Wouters L. Psychometric properties of the Subjective Well-Being Under Neuroleptics scale and the Subjective Deficit Syndrome Scale. Psychopharmacology (Berl) 2002;162:24–8.
Naber D. A self-rating to measure subjective effects of neuroleptic drugs, relationships to objective psychopathology, quality of life, compliance and other clinical variables. Int Clin Psychopharmacol 1995;10(Suppl 3):133–8.
Naber D, Moritz S, Lambert M, Pajonk FG, Holzbach R, Mass R, et al. Improvement of schizophrenic patients’ subjective well-being under atypical antipsychotic drugs. Schizophr Res 2001;50:79–88.
de Haan L, Lavalaye J, Linszen D, Dingemans PM, Booij J. Subjective experience and striatal dopamine D(2) receptor occupancy in patients with schizophrenia stabilized by olanzapine or risperidone. Am J Psychiatry 2000;157:1019–20.
de Haan L, van Bruggen M, Lavalaye J, Booij J, Dingemans PM, Linszen D. Subjective experience and D2 receptor occupancy in patients with recent-onset schizophrenia treated with low-dose olanzapine or haloperidol: a randomized, double-blind study. Am J Psychiatry 2003;160:303–09.
Innis RB, Cunningham VJ, Delforge J, Fujita M, Gjedde A, Gunn RN, et al. Consensus nomenclature for in vivo imaging of reversibly binding radioligands. J Cereb Blood Flow Metab 2007;27(9):1533–9.
Laruelle M, Abi-Dargham A, van Dyck CH, Rosenblatt W, Zea-Ponce Y, Zoghbi SS, et al. SPECT imaging of striatal dopamine release after amphetamine challenge. J Nucl Med 1995;36:1182–90.
Booij J, Korn P, Linszen DH, van Royen EA. Assessment of endogenous dopamine release by methylphenidate challenge using iodine-123 iodobenzamide single-photon emission tomography. Eur J Nucl Med 1997;24:674–7.
Kaasinen V, Aalto S, Nagren K, Rinne JO. Dopaminergic effects of caffeine in the human striatum and thalamus. Neuroreport 2004;15:281–5.
Booij J, Tissingh G, Boer GJ, Speelman JD, Stoof JC, Janssen AG, et al. [123I]FP-CIT SPECT shows a pronounced decline of striatal dopamine transporter labelling in early and advanced Parkinson’s disease. J Neurol Neurosurg Psychiatry 1997;62:133–40.
Laruelle M, D’Souza CD, Baldwin RM, Abi-Dargham A, Kanes SJ, Fingado CL, et al. Imaging D2 receptor occupancy by endogenous dopamine in humans. Neuropsychopharmacology 1997;17:162–74.
Engelman K, Horwitz D, Jéquier E, Sjoersma A. Biochemical and pharmacologic effects of (–methyltyrosine in man. J Clin Invest 1968;47:577–94.
Brodie HK, Murphy DL, Goodwin FK, Bunney WE Jr. Catecholamines and mania: the effect of alpha-methyl-para-tyrosine on manic behavior and catecholamine metabolism. J Clin Pharmacol Ther 1971;12:218–24.
Verhoeff NP, Hussey D, Lee M, Tauscher J, Papatheodorou G, Wilson AA, et al. Dopamine depletion results in increased neostriatal D(2), but not D(1), receptor binding in humans. Mol Psychiatry 2002;7(233):322–8.
Verhoeff NP, Christensen BK, Hussey D, Lee M, Papatheodorou G, Kopala L, et al. Effects of catecholamine depletion on D2 receptor binding, mood, and attentiveness in humans: a replication study. Pharmacol Biochem Behav 2003;74:425–32.
Schiffer WK, Volkow ND, Fowler JS, Alexoff DL, Logan J, Dewey SL. Therapeutic doses of amphetamine or methylphenidate differentially increase synaptic and extracellular dopamine. Synapse 2006;59:243–51.
McCann UD, Penetar DM, Shaham Y, Thorne DR, Gillin JC, Sing HC, et al. Sleep deprivation and impaired cognition. Possible role of brain catecholamines. Biol Psychiatry 1992;31:1082–97.
Plosker SM, Rabinovici J, Montalvo M, Jaffe RB. Endogenous catecholamines suppress thyrotropin secretion during the early follicular phase of the menstrual cycle. J Clin Endocrinol Metab 1995;80:2530–3.
Freeman ME, Kanyicska B, Lerant A, Nagy G. Prolactin: structure, function, and regulation of secretion. Physiol Rev 2000;80:1523–631.
de Haan L, Lavalaye J, van Bruggen M, van Nimwegen L, Booij J, van Amelsvoort T, et al. Subjective experience and dopamine D2 receptor occupancy in patients treated with antipsychotics: clinical implications. Can J Psychiatry 2004;49:290–6.
Fujita M, Verhoeff NP, Varrone A, Zoghbi SS, Baldwin RM, Jatlow PA, et al. Imaging extrastriatal dopamine D(2) receptor occupancy by endogenous dopamine in healthy humans. Eur J Pharmacol 2000;387:179–88.
Voruganti LN, Awad AG. Subjective and behavioural consequences of striatal dopamine depletion in schizophrenia-findings from an in vivo SPECT study. Schizophr Res 2006;88:179–86.
Acknowledgement
Grateful thanks go to the participants. The authors thank Merck & Co., Inc. for their gift of AMPT. The study was funded by the National Alliance for Research on Schizophrenia and Depression (NARSAD).
Statement of interest
None.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Boot, E., Booij, J., Hasler, G. et al. AMPT-induced monoamine depletion in humans: evaluation of two alternative [123I]IBZM SPECT procedures. Eur J Nucl Med Mol Imaging 35, 1350–1356 (2008). https://doi.org/10.1007/s00259-008-0739-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-008-0739-8