
Abstract
Objective
Clinical detection of gout can be difficult due to co-existent and mimicking arthropathies and asymptomatic disease. Understanding of the distribution of urate within the body can aid clinical diagnosis and further understanding of the resulting pathology. Our aim was to determine this distribution of urate within the extremities in patients with gout.
Materials and methods
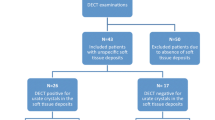
All patients who underwent a four-limb dual-energy computed tomography (DECT) scan for suspected gout over a 2-year period were identified (n = 148, 121 male, 27 female, age range, 16–92 years, mean = 61.3 years, median = 63 years). The reports of the positive cases were retrospectively analyzed and the locations of all urate deposition recorded and classified by anatomical location.
Results
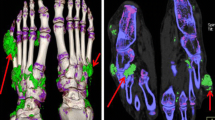
A total of 241 cases met the inclusion criteria, of which 148 cases were positive. Of these, 101 (68.2 %) patients had gout in the foot, 81 (56.1 %) in the knee, 79 (53.4 %) in the ankle, 41 (27.7 %) in the elbow, 25 (16.9 %) in the hand, and 25 (16.9 %) in the wrist. The distribution was further subcategorized for each body part into specific bone and soft tissue structures.
Conclusions
In this observational study, we provide for the first time a detailed analysis of extremity urate distribution in gout, which both supports and augments to the current understanding based on clinical and microscopic findings.


Similar content being viewed by others

References
Smith HS, Bracken D, Smith JM. Gout: current insights and future perspectives. J Pain. 2011;12(11):1113–29.
Janssens HJ, Janssen M, van de Lisdonk EH, Fransen J, van Riel PL, van Weel C. Limited validity of the American College of Rheumatology criteria for classifying patients with gout in primary care. Ann Rheum Dis. 2010;69(6):1255–6.
Kim KY, Ralph SH, Hunsche E, Wertheimer AI, Kong SX. A literature review of the epidemiology and treatment of acute gout. Clin Ther. 2003;25(6):1593–617.
Pascual E, Batlle-Gualda E, Martinez A, Rosas J, Vela P. Synovial fluid analysis for diagnosis of intercritical gout. Ann Intern Med. 1999;131(10):756–9.
Monu JU, Pope Jr TL. Gout: a clinical and radiologic review. Radiol Clin North Am. 2004;42(1):169–84.
McQueen FM, Doyle A, Dalbeth N. Imaging in gout—what can we learn from MRI, CT, DECT and US? Arthritis Res Ther. 2011;13(6):246.
Perez-Ruiz F, Dalbeth N, Urresola A. de ME, Schlesinger N. Imaging of gout: findings and utility. Arthritis Res Ther. 2009;11(3):232.
Bloch C, Hermann G, Yu TF. A radiologic reevaluation of gout: a study of 2,000 patients. AJR Am J Roentgenol. 1980;134(4):781–7.
Zhang W, Doherty M, Pascual E, Bardin T, Barskova V, Conaghan P, et al. EULAR evidence based recommendations for gout. Part I: Diagnosis. Report of a task force of the Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann Rheum Dis. 2006;65(10):1301–11.
Nicolaou S, Yong-Hing CJ, Galea-Soler S, Hou DJ, Louis L, Munk P. Dual-energy CT as a potential new diagnostic tool in the management of gout in the acute setting. AJR Am J Roentgenol. 2010;194(4):1072–8.
Dhanda S, Jagmohan P, Quek ST. A re-look at an old disease: a multimodality review on gout. Clin Radiol. 2011;66(10):984–92.
Choi HK, Burns LC, Shojania K, Koenig N, Reid G, Abufayyah M, et al. Dual energy CT in gout: a prospective validation study. Ann Rheum Dis. 2012;71(9):1466–71.
Glazebrook KN, Guimaraes LS, Murthy NS, Black DF, Bongartz T, Manek NJ, et al. Identification of Intraarticular and Periarticular Uric Acid Crystals with Dual-Energy CT: Initial Evaluation. Radiology. 2011;261(2):516–24.
Nicolaou S. Dual energy CT: In the detection of monosodium urate in patients with gouty arthropathy. Proceedings of the 96th Scientific Assembly and Annual Meeting of the Radiological Society of North America. 2010 Nov 3; 2010
Harris MD, Siegel LB, Alloway JA. Gout and hyperuricemia. Am Fam Physician. 1999;59(4):925–34.
Dalbeth N, Clark B, McQueen F, Doyle A, Taylor W. Validation of a radiographic damage index in chronic gout. Arthritis Rheum. 2007;57(6):1067–73.
Grahame R, Scott JT. Clinical survey of 354 patients with gout. Ann Rheum Dis. 1970;29(5):461–8.
Janssens HJ, Janssen M, van de Lisdonk EH, van Riel PL, van Weel C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomised equivalence trial. Lancet. 2008;371(9627):1854–60.
Roddy E, Zhang W, Doherty M. Are joints affected by gout also affected by osteoarthritis? Ann Rheum Dis. 2007;66(10):1374–7.
Garcia CO, Kutzbach AG, Espinoza LR. Characteristics of gouty arthritis in the Guatemalan population. Clin Rheumatol. 1997;16(1):45–50.
Zeng Q, Wang Q, Chen R, Xiao Z, Huang S, Xu J. Primary gout in Shantou: a clinical and epidemiological study. Chin Med J (Engl ). 2003;116(1):66–9.
Forbess LJ, Fields TR. The broad spectrum of urate crystal deposition: unusual presentations of gouty tophi. Semin Arthritis Rheum. 2012;42(2):146–54.
Surprenant MS, Levy AI, Hanft JR. Intraosseous gout of the foot: an unusual case report. J Foot Ankle Surg. 1996;35(3):237–43.
Levin MH, Lichtenstein L, Scott HW. Pathologic changes in gout; survey of eleven necropsied cases. Am J Pathol. 1956;32(5):871–95.
Dalbeth N, Kalluru R, Aati O, Horne A, Doyle AJ, McQueen FM. Tendon involvement in the feet of patients with gout: a dual-energy CT study. Ann Rheum Dis. 2013;72:1545–8.
Johnson TR, Fink C, Schonberg SO, Reiser MF. Dual Energy CT in Clinical Practice. 1st ed. New York: Springer; 2011.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mallinson, P.I., Reagan, A.C., Coupal, T. et al. The distribution of urate deposition within the extremities in gout: a review of 148 dual-energy CT cases. Skeletal Radiol 43, 277–281 (2014). https://doi.org/10.1007/s00256-013-1771-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-013-1771-8