
Abstract
Objective
To assess the technical results of CT fluoroscopy-guided, radiofrequency-induced vertebral augmentation (StabiliT®) in terms of vertebral height restoration and polymethylmethacrylate (PMMA) leakages, occurring in 25 individual patients with vertebral compression fractures and osteolysis.
Materials and methods
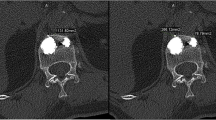
From 07/2010 to 08/2011, 25 patients (16 women, nine men; age 71 ± 14; range 41–89) with painful vertebral compression fractures due to osteoporosis (n = 19), metastases (n = 2) or multiple myeloma (n = 4) underwent vertebral augmentation with a radiofrequency-activated, high-viscosity polymethylmethacrylate (PMMA) bone cement (StabiliT® Vertebral Augmentation system; DFINE Europe GmbH, Mannheim) under local anesthesia. Thirty-four vertebrae (Th5–L5) were treated in 27 sessions under CT fluoroscopy guidance (128-row CT, Somatom Definition AS, Siemens, Erlangen) using a unilateral access and a cavity-creating osteotome prior to remote-controlled, hydraulically driven cement injection. 1/2/3 levels were treated in 21/5/1 session(s). Vertebral height change in the midsagittal plane (anterior, midvertebral, posterior endplate distance) and PMMA leaks were retrospectively evaluated using the postinterventional CT.
Results
All patients were successfully treated in the first session. Mean (MV ± SD) procedure time and amount of injected PMMA were 56 ± 14 min and 4.5 ± 1.4 ml, respectively. Mean anterior/midvertebral/posterior height gain was +7.1/+9.7/+0.4 %. Small local vertebral leaks were observed in 18/34 vertebrae (53 %) without any clinical sequelae. No major complications occurred.
Conclusions
CT fluoroscopy-guided, RF-induced vertebral augmentation with a high-viscosity bone cement (StabiliT®) was safe and technically successful in all patients. Using a hydraulic cement injection technique, a moderate restoration of anterior and midvertebral height was seen while the system was not markedly superior to standard vertebroplasty regarding the frequency of minor asymptomatic PMMA leaks.





Similar content being viewed by others


References
Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17(12):1726–33.
Lindsay R, Silverman SL, Cooper C, Hanley DA, Barton I, Broy SB, et al. Risk of new vertebral fracture in the year following a fracture. JAMA. 2001;285(3):320–3.
Galibert P, Deramond H, Rosat P, Le Gars D. Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty. Neurochirurgie. 1987;33(2):166–8.
Lieberman IH, Dudeney S, Reinhardt MK, Bell G. Initial outcome and efficacy of "kyphoplasty" in the treatment of painful osteoporotic vertebral compression fractures. Spine. 2001;26(14):1631–8.
Kayanja MM, Togawa D, Lieberman IH. Biomechanical changes after the augmentation of experimental osteoporotic vertebral compression fractures in the cadaveric thoracic spine. Spine J. 2005;5(1):55–63.
Hadjipavlou AG, Tzermiadianos MN, Katonis PG, Szpalski M. Percutaneous vertebroplasty and balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures and osteolytic tumours. J Bone Joint Surg. 2005;87(12):1595–604.
Gangi A, Sabharwal T, Irani FG, Buy X, Morales JP, Adam A. Quality assurance guidelines for percutaneous vertebroplasty. Cardiovasc Intervent Radiol. 2006;29(2):173–8.
Hohl C, Suess C, Wildberger JE, Honnef D, Das M, Muhlenbruch G, et al. Dose reduction during CT fluoroscopy: phantom study of angular beam modulation. Radiology. 2008;246(2):519–25.
Elgeti FA, Marnitz T, Kroncke TJ, Gebauer B. DFine radiofrequency kyphoplasty (RFK)–kyphoplasty with ultrahigh viscosity cement. Rofo. 2010;182(9):803–5.
Upasani VV, Robertson C, Lee D, Tomlinson T, Mahar AT. Biomechanical comparison of kyphoplasty versus a titanium mesh implant with cement for stabilization of vertebral compression fractures. Spine (Phila Pa 1976). 2010; 35(19):1783–1788.
Ghofrani H, Nunn T, Robertson C, Mahar A, Lee Y, Garfin S. An evaluation of fracture stabilization comparing kyphoplasty and titanium mesh repair techniques for vertebral compression fractures: is bone cement necessary? Spine (Phila Pa 1976). 2010;35(16):E768-773.
Rotter R, Martin H, Fuerderer S, Gabl M, Roeder C, Heini P, et al. Vertebral body stenting: a new method for vertebral augmentation versus kyphoplasty. Eur Spine J. 2010;19(6):916–923.
Shen GW, Wu NQ, Zhang N, Jin ZS, Xu J, Yin GY. A prospective comparative study of kyphoplasty using the Jack vertebral dilator and balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures. J Bone Joint Surg. 2010;92(9):1282–8.
Chen C, Chen L, Gu Y, Xu Y, Liu Y, Bai X, et al. Kyphoplasty for chronic painful osteoporotic vertebral compression fractures via unipedicular versus bipedicular approachment: a comparative study in early stage. Injury. 2010;41(4):356–359.
Grohs JG, Matzner M, Trieb K, Krepler P. Minimal invasive stabilization of osteoporotic vertebral fractures: a prospective nonrandomized comparison of vertebroplasty and balloon kyphoplasty. J Spinal Disord Tech. 2005;18(3):238–42.
Hulme PA, Krebs J, Ferguson SJ, Berlemann U. Vertebroplasty and kyphoplasty: a systematic review of 69 clinical studies. Spine. 2006;31(17):1983–2001.
Phillips FM, ToddWetzel F, Lieberman I, Campbell-Hupp M. An in vivo comparison of the potential for extravertebral cement leak after vertebroplasty and kyphoplasty. Spine. 2002;27(19):2173–8. discussion 2178–2179.
Vasconcelos C, Gailloud P, Martin JB, Murphy KJ. Transient arterial hypotension induced by polymethylmethacrylate injection during percutaneous vertebroplasty. J Vasc Interv Radiol. 2001;12(8):1001–2.
Harrington KD. Major neurological complications following percutaneous vertebroplasty with polymethylmethacrylate: a case report. The Journal of Bone and joint surgery. 2001; 83-A(7):1070–1073.
Mizrahi B, Shavit R, Domb A. Synthesis and characterization of polymeric implant for kyphoplasty. J Biomed Mater Res. 2008;86B(2):466–73.
Anselmetti GC, Zoarski G, Manca A, Masala S, Eminefendic H, Russo F, et al. Percutaneous vertebroplasty and bone cement leakage: clinical experience with a new high-viscosity bone cement and delivery system for vertebral augmentation in benign and malignant compression fractures. Cardiovasc Intervent Radiol. 2008;31(5):937–47.
Polikeit A, Nolte LP, Ferguson SJ. The effect of cement augmentation on the load transfer in an osteoporotic functional spinal unit: finite-element analysis. Spine (Phila Pa 1976). 2003; 28(10):991–996.
Campbell PG, Harrop JS. Incidence of fracture in adjacent levels in patients treated with balloon kyphoplasty: a review of the literature. Cur Rev Musculoskel Med. 2008;1(1):61–4.
Conflict of interest disclosure
The authors declare no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Trumm, C.G., Jakobs, T.F., Stahl, R. et al. CT fluoroscopy-guided vertebral augmentation with a radiofrequency-induced, high-viscosity bone cement (StabiliT®): technical results and polymethylmethacrylate leakages in 25 patients. Skeletal Radiol 42, 113–120 (2013). https://doi.org/10.1007/s00256-012-1386-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-012-1386-5