
Abstract
Introduction
In renal transplant patients, bone loss may be related to the drugs patients are taking but also to their past history of chronic kidney disease. The purpose of this study was to assess changes in BMD 2 years after an initial assessment (performed 9 months post transplantation) and the factors associated with these changes.
Methods
This longitudinal study included patients who had undergone a renal transplantation between 2005 and 2011, and who were followed up at the Lille Regional University Hospital. Patients were included if they had a first bone evaluation (including bone densitometry, spine X-rays and biological assessment) and at least another BMD assessment. The first assessment was performed on average 9 months post transplantation. A second assessment was performed at 2 years.
Results
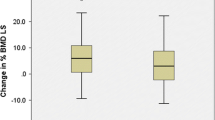
Two hundred fifty-nine out of 366 patients satisfied the inclusion criteria. The population included 96 women. Mean age at transplantation was 49.7 ± 12.1 years. Mean duration of dialysis was 3.2 ± 3.3 years. For 75 patients (29.0%), corticosteroid treatment was discontinued 7 days after transplantation without subsequent resumption during follow-up. Vertebral fractures assessed by X-rays at baseline were found in 28 patients (10.8%). According to the WHO classification, 106 patients (40.9%) patients had osteoporosis and 111 patients (42.8%) had osteopenia at the first assessment. Oral bisphosphonates were prescribed for 95 patients. The decision to prescribe bisphosphonates was taken jointly by rheumatologists and nephrologists based on BMD assessment, past history of fracture and corticosteroid management. In all patients, BMD gains at the second evaluation (2.2 ± 0.79 years) compared with baseline were significant (3.9 ± 6.6, 2.6% ± 7.6, 3.0 ± 7.2% at the lumbar spine, femoral neck and total hip respectively; p < 0.0001). The difference in gain between bisphosphonate-treated and untreated patients was significant (+ 5.0 ± 0.8% (p < 0.0001), + 2.5 ± 1.0% (p = 0.01) and + 2.7 ± 0.9% (p < 0.01) at the lumbar spine, femoral neck and total hip respectively. The patients who benefited early corticosteroid discontinuation had higher gains in BMD at the lumbar spine (+ 2.1 ± 0.9%; p = 0.02) and total hip (+ 2.0 ± 1.0%; p = 0.04) compared to those for whom corticosteroid therapy was maintained. Stepwise regression analysis (patients without bisphosphonates) showed associations between change in BMD (femoral neck) and duration of corticosteroid therapy, bone alkaline phosphatase level at baseline, and absence of vertebral fracture. No correlation was found between change in BMD and duration of dialysis or renal function.
Conclusion
Kidney transplant recipients have an increased risk of bone fragility in the year following transplantation. Bisphosphonates and early corticosteroid discontinuation can improve BMD.

Similar content being viewed by others


References
Couchoud C (2015) REIN Annual Rapport 2013
Eckardt K-U, Kasiske BL (2009) KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease-mineral and bone disorder (CKD-MBD). Kidney Int 76:S1–S2. https://doi.org/10.1038/ki.2009.188
Toussaint ND, Lau KK, Strauss BJ, Polkinghorne KR, Kerr PG (2008) Associations between vascular calcification, arterial stiffness and bone mineral density in chronic kidney disease. Nephrol Dial Transplant 23:586–593. https://doi.org/10.1093/ndt/gfm660
Danese MD, Kim J, Doan QV, Dylan M, Griffiths R, Chertow GM (2006) PTH and the risks for hip, vertebral, and pelvic fractures among patients on dialysis. Am J Kidney Dis 47:149–156. https://doi.org/10.1053/j.ajkd.2005.09.024
Coco M, Rush H (2000) Increased incidence of hip fractures in dialysis patients with low serum parathyroid hormone. Am J Kidney Dis Off J Natl Kidney Found 36:1115–1121. https://doi.org/10.1053/ajkd.2000.19812
Mittalhenkle A, Gillen DL, Stehman-Breen CO (2004) Increased risk of mortality associated with hip fracture in the dialysis population. Am J Kidney Dis 44:672–679. https://doi.org/10.1053/j.ajkd.2004.07.001
Kaneko TM, Foley RN, Gilbertson DT, Collins AJ (2007) Clinical epidemiology of long-bone fractures in patients receiving hemodialysis. Clin Orthop Relat Res 457:188–193. https://doi.org/10.1097/BLO.0b013e318031465b
Julian BA, Laskow DA, Dubovsky J, Dubovsky EV, Curtis JJ, Quarles LD (1991) Rapid loss of vertebral mineral density after renal transplantation. N Engl J Med 325:544–550. https://doi.org/10.1056/NEJM199108223250804
Rojas E, Carlini RG, Clesca P, Arminio A, Suniaga O, de Elguezabal K, Weisinger JR, Hruska KA, Bellorin-Font E (2003) The pathogenesis of osteodystrophy after renal transplantation as detected by early alterations in bone remodeling. Kidney Int 63:1915–1923. https://doi.org/10.1046/j.1523-1755.2003.00938.x
Nikkel LE, Hollenbeak CS, Fox EJ et al (2009) Risk of fractures after renal transplantation in the United States. [Miscellaneous Article]. Transplant 87:1846–1851. https://doi.org/10.1097/TP.0b013e3181a6bbda
Coco M, Glicklich D, Faugere MC, Burris L, Bognar I, Durkin P, Tellis V, Greenstein S, Schechner R, Figueroa K, McDonough P, Wang G, Malluche H (2003) Prevention of bone loss in renal transplant recipients: a prospective, randomized trial of intravenous pamidronate. J Am Soc Nephrol 14:2669–2676. https://doi.org/10.1097/01.ASN.0000087092.53894.80
Grotz WH, Mundinger FA, Rasenack J et al (1995) Bone loss after kidney transplantation: a longitudinal study in 115 graft recipients. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc—ur Ren Assoc 10:2096–2100
Giannini S, D’Angelo A, Carraro G et al (2001) Alendronate prevents further bone loss in renal transplant recipients. J Bone Miner Res 16:2111–2117. https://doi.org/10.1359/jbmr.2001.16.11.2111
Horber FF, Casez JP, Steiger U et al (1994) Changes in bone mass early after kidney transplantation. J Bone Miner Res 9:1–9. https://doi.org/10.1002/jbmr.5650090102
Gupta AK, Huang M, Prasad GVR (2012) Determinants of bone mineral density in stable kidney transplant recipients. J Nephrol 25:373–383. https://doi.org/10.5301/jn.5000015
Jha V, Govindarajan S, Khandelwal N, Sakhuja V (2011) Bone mineral density in patients with end-stage renal disease and its evolution after kidney transplantation. Indian J Nephrol 21:85–89. https://doi.org/10.4103/0971-4065.82140
Alshayeb HM, Josephson MA, Sprague SM (2013) CKD–mineral and bone disorder management in kidney transplant recipients. Am J Kidney Dis 61:310–325. https://doi.org/10.1053/j.ajkd.2012.07.022
Unal A, Kocyigit I, Sipahioglu MH, Tokgoz B, Kavuncuoglu F, Oymak O, Utas C (2010) Loss of bone mineral density in renal transplantation recipients. Transplant Proc 42:3550–3553. https://doi.org/10.1016/j.transproceed.2010.07.106
Nishioka S, Sofue T, Inui M, Nishijima Y, Moriwaki K, Hara T, Mashiba T, Kakehi Y, Kohno M (2014) Mineral and bone disorder is temporary in patients treated with early rapid corticosteroid reduction after kidney transplantation: a single-center experience. Transplant Proc 46:514–520. https://doi.org/10.1016/j.transproceed.2013.11.153
Nikkel LE, Mohan S, Zhang A, McMahon DJ, Boutroy S, Dube G, Tanriover B, Cohen D, Ratner L, Hollenbeak CS, Leonard MB, Shane E, Nickolas TL (2012) Reduced fracture risk with early corticosteroid withdrawal after kidney transplant: fewer fractures with ECSW after transplant. Am J Transplant 12:649–659. https://doi.org/10.1111/j.1600-6143.2011.03872.x
Long-term fracture risk following renal transplantation: a population-based study. Springer. https://doi.org/10.1007/s00198-003-1532-y
Orcel P (2005) Prevention and treatment of glucocorticoid-induced osteoporosis in 2005. Joint Bone Spine 72:461–465. https://doi.org/10.1016/j.jbspin.2005.09.002
Grotz W, Nagel C, Poeschel D, Cybulla M, Petersen KG, Uhl M, Strey C, Kirste G, Olschewski M, Reichelt A, Rump LC (2001) Effect of ibandronate on bone loss and renal function after kidney transplantation. J Am Soc Nephrol 12:1530–1537
Jeffery JR, Leslie WD, Karpinski ME et al (2003) Prevalence and treatment of decreased bone density in renal transplant recipients: a randomized prospective trial of calcitriol versus alendronate. [Miscellaneous Article]. Transplant 76:1498–1502
Fan SL-S, Kumar S, Cunningham J (2003) Long-term effects on bone mineral density of pamidronate given at the time of renal transplantation. Kidney Int 63:2275–2279. https://doi.org/10.1046/j.1523-1755.2003.00012.x
El-Agroudy AE, El-Husseini AA, El-Sayed M et al (2005) A prospective randomized study for prevention of postrenal transplantation bone loss. Kidney Int 67:2039–2045. https://doi.org/10.1111/j.1523-1755.2005.00306.x
Nowacka-Cieciura E, Cieciura T, Bączkowska T, Kozińska-Przybył O, Tronina O, Chudziński W, Pacholczyk M, Durlik M (2006) Bisphosphonates are effective prophylactic of early bone loss after renal transplantation. Transplant Proc 38:165–167. https://doi.org/10.1016/j.transproceed.2005.12.041
Conley E, Muth B, Samaniego M, Lotfi M, Voss B, Armbrust M, Pirsch J, Djamali A (2008) Bisphosphonates and bone fractures in long-term kidney transplant recipients. Transplantation 86:231–237. https://doi.org/10.1097/TP.0b013e318176b40f
Torregrosa JV, Fuster D, Pedroso S, Diekmann F, Campistol JM, Rubí S, Oppenheimer F (2007) Weekly risedronate in kidney transplant patients with osteopenia. Transpl Int 20:708–711. https://doi.org/10.1111/j.1432-2277.2007.00501.x
Stein EM, Ortiz D, Jin Z, McMahon DJ et al (2011) Prevention of fractures after solid organ transplantation: a meta-analysis. J Clin Endocrinol Metab 96:3457–3465. https://doi.org/10.1210/jc.2011-1448
Versele EB, Van Laecke S, Dhondt AW et al (2016) Bisphosphonates for preventing bone disease in kidney transplant recipients: a meta-analysis of randomized controlled trials. Transpl Int 29:153–164. https://doi.org/10.1111/tri.12691
Marcén R, Caballero C, Uriol O, Fernández A, Villafruela JJ, Pascual J, Martins J, Rodriguez N, Burgos FJ, Ortuño J (2007) Prevalence of osteoporosis, osteopenia, and vertebral fractures in long-term renal transplant recipients. Transplant Proc 39:2256–2258. https://doi.org/10.1016/j.transproceed.2007.07.073
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Nicolas SEGAUD: none.
Isabelle LEGROUX: none.
Marc HAZZAN has received honorarium and grants from Novartis, Astellas and Roche.
Christian NOEL: none.
Bernard CORTET has received consultancy fees, lecture fees and honorarium from Amgen, Eli Lilly, Expanscience, Ferring, Medtronic, Novartis, Roche Diagnostics and Servier.
Rights and permissions
About this article

Cite this article
Segaud, N., Legroux, I., Hazzan, M. et al. Changes in bone mineral density after kidney transplantation: 2-year assessment of a French cohort. Osteoporos Int 29, 1165–1175 (2018). https://doi.org/10.1007/s00198-018-4383-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-018-4383-2